UGS Urogenital Schistosomiasis, this entity refers to the presence of Schistosoma ova in the urinary tract and genital tract of both men and women. However, on the North Coast there was a significant association between SCA and genital and urinary Schistosoma oocytes (p=0.005).
CHAPTER ONE 1.1 Introduction
Aims and Objectives
List of Manuscripts Paper 1
Short Communication
CHAPTER TWO
Introduction
Epidemiology of schistosomiasis
Life Cycle and Pathology
Children are predisposed to infection due to factors such as poor hygiene related to excretion and their tendency to play in contaminated water (Wright 1986). The male and female worm pair remain as a "monogamous pair" together for their lifetime, with the female producing eggs and the male fertilizing them (Gryseels et al.
Schistosoma in the urogenital tracts
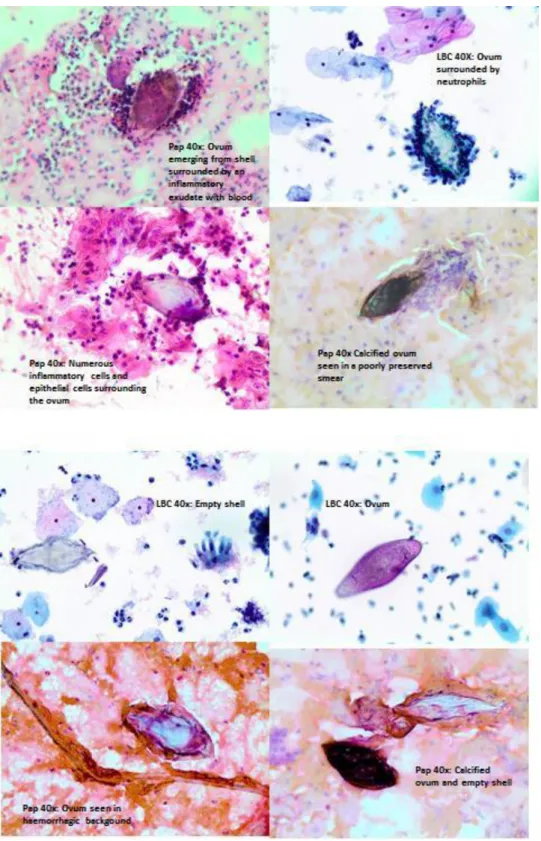
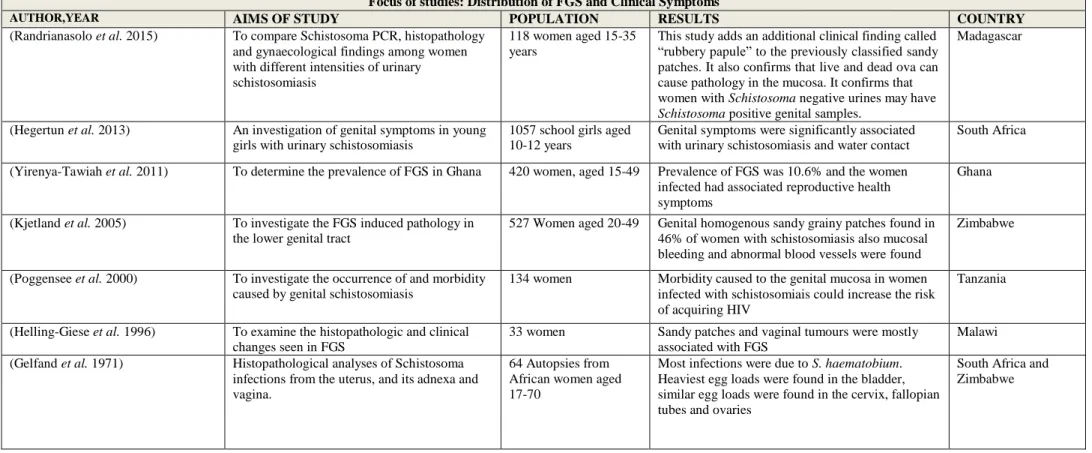
Oocytes were found throughout the female genital tract: in the ovaries; fallopian tubes; uterus and placenta; cervix and vagina (Poggensee et al. 2001b; Kjetland, Leutscher and Ndhlovu 2012). In this study, sand spots and vaginal tumors were found to be mostly associated with FGS (Helling-Giese et al. 1996).
Female genital schistosomiasis and cervical cancer
This study adds an additional clinical finding called gummy papule" to the previously classified sandy spots. To investigate the reversibility of lower genital tract abnormalities in women with Schistosoma infections after treatment with praziquantel.
Epidemiology of Cervical Cancer
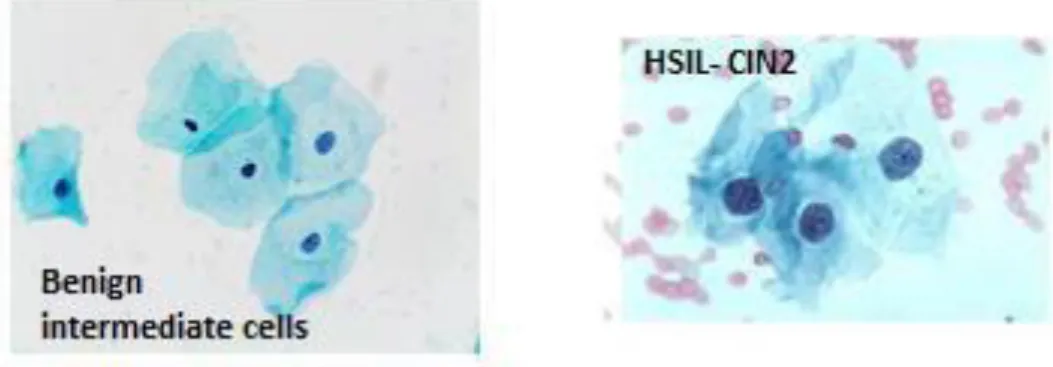
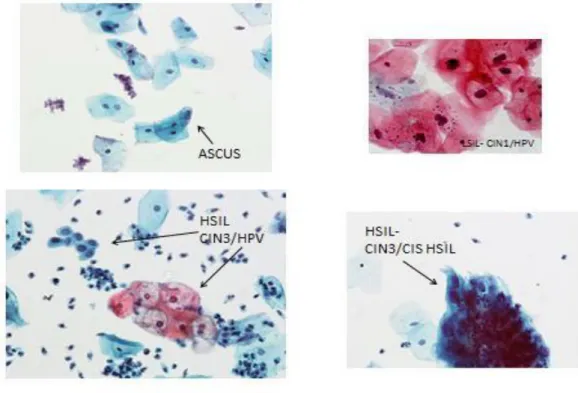
Since HPV is so strongly associated with dysplasia and is often indistinguishable from CIN1/mild dysplasia, it is placed in the same category under low-grade squamous cell carcinoma. Conversely, severe dysplasia and carcinoma-in-situ dysplasia also known as high-grade squamous intraepithelial lesion (HSIL) are more likely to persist and progress to invasive cancer.
Risk Factors for cervical cancer
Cervical screening among young women is therefore a subject of much debate in light of the theory that lesions tend to disappear. In developing countries such as South Africa, where young women are at risk of both HIV and schistosomiasis, and cervical cancer is the second most common cancer, it is important to raise awareness of the effects of HPV among young women at risk of these diseases.
Implications for cervical cancer and HIV
In addition, the following risk factors were identified from the results of the reanalysis of twelve invasive cervical cancer studies (Berrington and Green 2007). There are concerns about overdiagnosis and overtreatment among young women (Szarewski and Sasieni 2004).
Association of schistosomiasis with HIV
Anti-schistosomal Treatment
While mass treatment is effective in killing the adult worms responsible for egg laying, it is not known what effect it has on FGS lesions. One study showed that treatment given to women with FGS lesions in adulthood appeared to leave the lesions unchanged (Kjetland et al. 2006).
Diagnosing FGS
Molecular techniques such as PCR in feces and urine have also been established (Verweij et al. 2007); A challenge with immunological markers is that they cannot be used to distinguish between past and present infections (Obeng et al. 2008).
Urine and stool microscopy
Egg quantification has been shown to be important in monitoring schistosomiasis treatment programs (Kosinski et al. 2011). Urine microscopy is a relatively inexpensive and easy diagnostic test, but requires repeated sampling and careful examination to enable high sensitivity and specificity especially in light infections (Obeng et al. 2008).
Real-time polymerase chain reaction (PCR) in Urine and Cervico-vaginal lavage The use of PCR to detect schistosomiasis began with the amplification of DNA sequences in
While urine and fecal samples are well-established tests for the detection of Schistosoma DNA using real-time PCR, a previous study on genital schistosomiasis conducted among rural Zimbabwean women explored the use of cervico-vaginal lavage samples for Schistosoma DNA. DNA examined (Kjetland et al. 2009b). ). The sample size in this study was small and further research is needed to validate these assumptions (Kjetland et al. 2009b).
Cytology
In this study, the use of PCR in the detection of schistosomiasis was investigated in urine and vaginal lavage samples. The use of schistosome DNA in urine and cervico-vaginal lavage samples was investigated in paper 2.
Alternative cervical cancer screening tools to cytology
The worldwide prevalence of HPV in cervical cancer is 99.7%, and the association of so-called high-risk (probably oncogenic) HPV with cervical cancer makes HPV the highest attributable and specific factor for any major human cancer (Walboomers et et al. 1999). ). One limitation of this approach is that it is not always accurate in identifying precancerous conditions.
Management of Premalignant Cytologic Findings
Summary
CHAPTER THREE
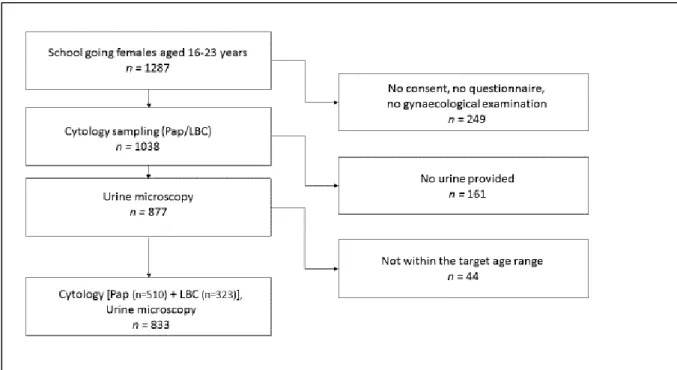
Materials and methods 3.1. Study setting and design
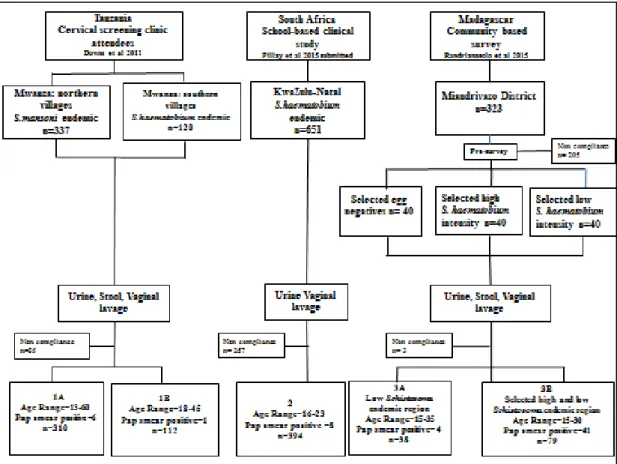
Two areas Ugu and Ilembe/Uthungulu located along the Indian Ocean south and north of the city of Durban were included in the study. The districts of Ilembe and Uthungulu are located on the north coast of KwaZulu-Natal and this area of the study houses a population of approximately 570 000 people.
Ethics and Permissions
The individual district prevalences for HIV among antenatal women were as follows: 38.3% in Ugu district, and 37.4% and 38.5% in Ilembe and Uthungulu districts, respectively (Directorate of Epidemiology 2013).
Data collection
Participants who gave their consent underwent a semi-structured private interview conducted by research assistants in “isiZulu”, the local language, including history of water contact, red urine and genital symptoms. The fractions were stored in the dark at 4°C for up to one week and then stored at -80°C for several months before being transported to the Netherlands in frozen conditions for DNA isolation and detection.
Laboratory Analysis 1 Schistosoma PCR analysis
- Pap smears and liquid-based cytology samples
Traditional Pap smears were collected by scraping a wooden spatula from the cervix and the cervical surface of the fornices. Traditional pap smears were collected from all the participants from Ugu district and 519 of the participants from Ilembe district.
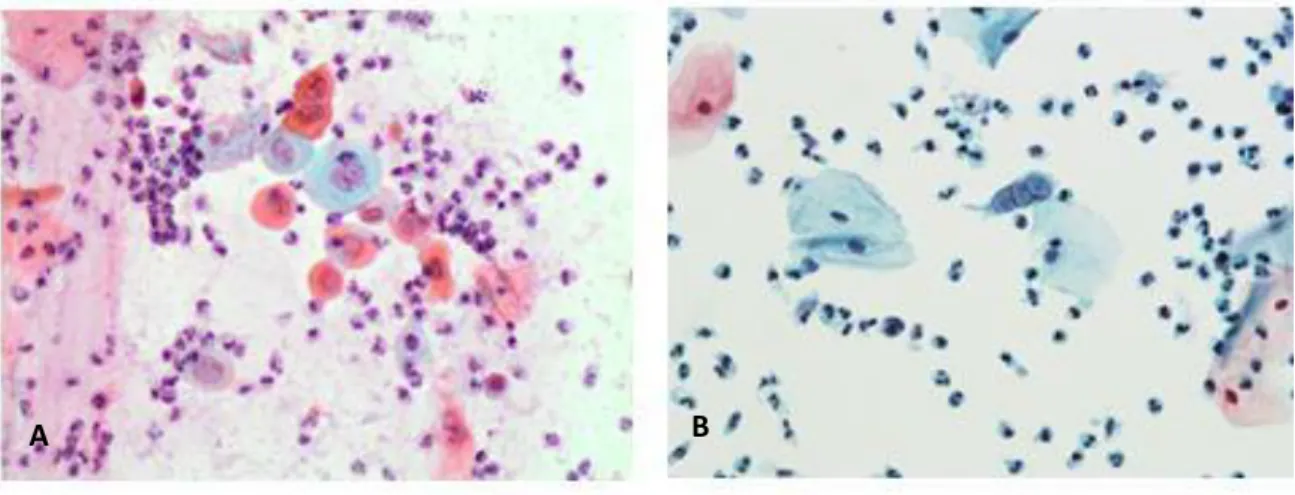
LBC 40x: excess background material is removed and cells are well preserved and easily visualized
- Statistical analyses
- Linking of objectives and papers
- CHAPTER FOUR 4.1 Paper 1
- Paper 2
- CHAPTER FIVE
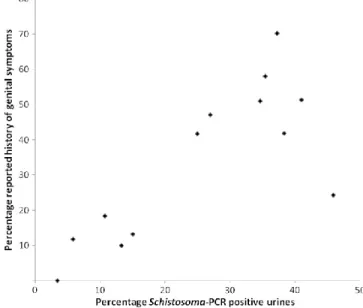
In the Netherlands, DNA isolation and PCR setup were performed at the Leiden University Medical Center with a custom-built automated liquid handling station (Hamilton, Bonaduz, Switzerland). The PCR analysis of urine samples on the first day showed Schistosoma DNA in 25.4% of the samples. Four of the 36 microscopy-positive urine samples were missed in South Africa; these samples showed positive results in the Netherlands.
Cervical cytology as a diagnostic tool for female genital
Paper 3
CHAPTER SIX
Informed consent was part of the inclusion procedure and menstruating women were excluded from participation (Downs et al. 2011). Full details of the study design, ethical aspects, sample collection and main results have been described elsewhere (Holmen et al. 2015) (Pillay, 2015 submitted). None of them were positive in the lavage Schistosoma PCR, one showed Schistosoma DNA in the urine and two of them in the feces.
CHAPTER SEVEN 7.1 Paper 4
We also wanted to compare two diagnostic methods for cytological evaluations [Pap smears and Liquid-based cytology (LBC)] and investigate DNA analysis in the remaining LBC sample as a tool for risk assessment for high-risk HPV types. Importantly, HPV genotyping in the remaining LBC samples worked very well in the 10 cases diagnosed as HSIL. When ova of the parasite Schistosoma haematobium become stuck in the genital mucosa, they cause immunological and tissue changes.
Squamous cell atypia
CHAPTER EIGHT 8.1 Paper 5-Short Communication
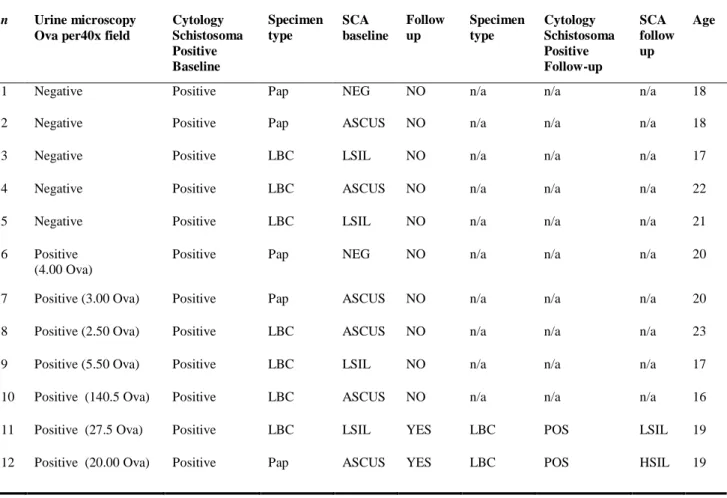
Preliminary findings of the effect of prior treatment with Praziquantel on squamous cell atypia are described in young women at risk of female genital schistosomiasis. The purpose of writing this brief notice is to consider the purpose of the study on the effect of anti-schistosomal treatment with Praziquantel on squamous cell atypia (SCA). At the start of the research, it was postulated that the mass drug administration (MDA) would be rolled out in the study settings and that we could measure the effect of cervical atypia in relation to mass treatment at baseline and after treatment.
Short Communication
- CHAPTER NINE 9.1 Unpublished Cytology Results
- Synthesis
- CHAPTER TEN
- Limitations
- CHAPTER ELEVEN
- Conclusions and Recommendations
Squamous atypia was found among some of the women who reported previous anti-schistosomal treatment (Figure 2). Most of the squamous atypia in our study were in the LSIL category; it was too. Of the young women in the study sample, 41% on the South Coast had one child while 63% had one child on the North Coast.
HIV and pre-neoplastic and neoplastic lesions of the cervix in South Africa: a case-control study. A study of female genital schistosomiasis of the lower reproductive tract in the Volta Basin of Ghana.
TEEN QUESTIONNAIRE
- Isikole / school
- Igama lesikole sebanga eliphansi ophuma kuso / Name of the primary school you came from
- Uyasebenza na? njenge?/Are you working? As?
- Wazalelwaphi? / Where were you born ?
- Inkolo / Religious affiliation [Christian] [Muslim] [Shembe] [Leganyana] [Methodist]
- Ulimi lwasekhaya / Home Language [Zulu] [Xhosa] [English] [Other ALLERGY
- Ugcine nini ukuya esikhathini? / LMP (First day of last menstural period)
- Waqala uneminyaka emingaki ukuya esikhathini? / Age of your first menstruation?
- Ubanaso isilumo kangangokuba kumele uhlale ekhaya? / Do you normally have painful periods so that you have to stay home from school? [yebo] [cha]
- Ubanaso isilumo esikwenza ufise ukuthatha amaphilisi ezinhlungu? / Do you normally have painful periods so that you wish to take painkillers? [yebo] [cha]
- Indlela yokuhlela / Contraceptive method
- Uya ngendlela efanayo nyanga zonke / Are your periods regular [yebo] [cha] [NA= Post Partum / if injectable contraceptive / pills]
- Uya izinsuku ezingaki esikhathini? / How many days does your period normally last?
- Kuye kwenzeke wophe ungalindele? / Do you have times of unexpected bleeding or spotting in between your normal periods? [yebo] [cha] [NA= Post Partum / if injectable
- Ujwayele ukopha kakhulu kuze kube namahluli? / Do you normally have periods with heavy bleeding and clots? [yebo] [cha] [NA= Post Partum / if injectable contraceptive /
- Wake walashelwa isichenene nini?/ Have you ever been treated for Bilharzia, when?
- Urinary symptoms
- Manje ngizokubuza ngezinhlobo zezinto ozenzayo noma owake wazenza ngamanzi, uzenza noma wazenza kangakanani, uhlala isikhathi esingakanani emanzini nokuthi umzimba
- Kukhona isikhathi empilweni yakho owake wahlangana nalamanzi? [yebo] [cha]
- Usuke wathintana namanzi omfula noma idamu ngonyaka odlule (2013) noma kulonyaka (2014)? / Did you have contact with the river or dam in 2013 or 2014? [yebo]
- Kubukeka kunjani ukuphuma ngaphansi kuwena? / How is your current discharge?
- Usuke wabanazo izinhlungu esinyeni? [yebo] [cha] Uma kungu Yebo sicela uchaze: / Have you ever experienced abdominal pain? If YES, please explain
- Uke wakusebenzisa okulandelayo kuleli sonto eledlule / Have you used the following the last week( the last 7 days): Ikhondomu yabesilisa / male condom [yebo] [cha]
- Uyazi ukuthi ziyini izifo zocansi STI? / Do you know what an STI is? [yebo] [cha] [angazi]
- Wake walashelwa izifo zocansi ngenyanga edlule? / Have you been treated for an STI the last 4 weeks? [yebo] [cha] [angazi]
- Ucabanga ukuthi unaso isifo socansi njengamanje? / Do you think you have an STI now?
- Waqala uneminyaka emingaki ukwenza ucansi? / What was your age when you had sex for the first time? | | |
- Uma ubanezinhlungu wenza ucansi chaza ukungaphatheki kahle kwakho: / If you have pain during sex, please describe the discomfort
- Hloboluni locansi owake walwenza? / What kind of sex have you had?
- Ucabanga ukuthi kujwayelekile ukopha kancane emva kokwenza ucansi / Do you think it is normal to have a little bleeding after sex? [yebo] [cha] [angazi]
- Uke wabona wopha emva kocansi? / Have you ever seen bleeding after sex?
- Uyalwenza ucansi ngesinye iskhathi uma usesikhathini / Do you sometimes have intercourse during your menstrual period [yebo] [cha]
- Uke uzizwe ucindezelekile ukwenza ucansi nomuntu ngenxa yezipho/imali akunike yona? / Have you ever felt pressured to have sex, because of the gifts or money you have been given ?
- Wake wahlukunyezwa ngokocansi noma waphoqwa ukwenza ucansi / Have you ever been sexually abused or forced to have intercourse? [yebo] [cha] IF YES
- Sekuke kwenzeka kulezinsuku ezintathu ezidlule? / Has it happened the last 3 days? [yebo]
- a) Wayeneminyaka emingaki umaqondana wakho omdala kunabo bonke? / How old was your oldest partner? |
- Uma ucabanga wake waba nomaqondana onesandulela ngculazi / Do you think you have had an HIV positive partner ? [yebo] [cha] [angazi]
- Uke waba nnmaqondana odla imishanguzo / Have you ever had a partner who is taking ARV’s?
- Unaye umaqondana njengamanje? / Do you have a steady partner at the moment? [yebo] [cha]
- Ezinyangeni ezintathu ezedlule ugcina ukwenza ucansi waphuza utshwala noma
- Wake wahlolelwa isandulela ngculazi / Have you been tested for HIV? [yebo] [cha]
- Ungakhululeka ukungitshela ngesimo sengculazi, ingabe unaso isandulela ngculazi? Would you feel comfortable telling me your status, do you have HIV? [yebo] [cha] [angazi] [Patient
- Uyayithatha imishanguzo? / Are you taking ARV’s? [yebo] [cha]
- Ungathanda ukuthi sinihlelele iqembu lokululekana nabanye abafundi abanesimo esifana nesakho?/Would you like us to organise a support group for HIV positive learners and would
- Ingabe abangani bakho bayazisebenzisa izidakamizwa? / Do your friends use drugs? [yebo]
- Uyazisebenzisa izidakamizwa? / Do you use drugs ? [yebo] [cha]
- Wake wasebenzisa okunye noma okungaphezulu kwalokhu okulandelayo? / Have you ever used one or more of the following
- Qala ngomdala kunabobonke endlini: / Start with the oldest in the household
Do you usually have painful periods so you have to stay home from school? [yebo] [cha] painful periods so you have to stay home from school? [yebo] [cha]. Would you feel comfortable telling me your status, do you have HIV? [yebo] [cha] [angazi] [Patient you feel safe to tell me your status, do you have HIV? [yebo] [cha] [angazi] [Patient refused information]. Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No.
REDUCING BILHARZIA PROJECT
Personal data page 1. Isibongo / Surname(s )
- Ujwayele ukulala kangakanani lapha? sonke isikhathi ingxenye yesikhathi / How often do you sleep here? (All the time / Most of the time)
- Ingabe ikhona enye indawo ohlala kuyo ngezimpelasonto, amaholide noma ezinye izinsuku? yebo cha Uma kungu CHA → 11/ _/Is there another place where
- Unaso esinye isihlobo esisondele kuwe esihlala kwenye indlu? yebo cha uma kung CHA → 12 / Do you have any other close relative living in another
- Uma ungase ube nohambo noma usuke kulendawo, ubani ongaba nemininingwane yakho yokukuthinta (ngaphandle kwalena engenhla)? /If you
- Awukakamusho/yiphathi u/ekamama wakho noma ubaba wakho okuzalayo
Ingabe uhlala endaweni efanayo nawe? Ingabe uyaxhumana nobaba/umama wakho? . yebo cha ngeke kwenzeke lokho.. yebo cha NA . yebo cha ngeke kwenzeke lokho.. yebo cha NA . ii) Umama/ubaba wakho uhlala eduze kwalapho uhlala khona? . yebo cha ngeke kwenzeke lokho.. yebo cha NA . yebo cha akwenzeki lokho. Ingabe ubaba/umama wakho uhlala eduze nawe? . iii) Yiliphi izinga eliphezulu lemfundo kamama/uyihlo? . /Iyiphi imfundo ephakeme kanyoko/ubaba wakho?
Family and living
- Wahlala isikhathi esingakanani lapho? Isikhathi esingaphansi konyaka 1-5 iminyaka ngaphezulu kuka 5 weminyaka /For how long did you live there?(Less than 1
- Ngubani omandla ekunihlinzekeni/pheni ekhaya? (igama nobuhlobo) /Who is the main provider in the household? (name and relation)
- Uwatholaphi amanzi okuphuza? emfuleni empompini/womphakathi esiphethwini esivikelekile esiphethwini esingavikelekile kuxubene
- Ingabe amantombazane ekilasini lakho ayabhukuda emfuleni noma edamini ezinsukwini ezishisayo? yebo cha angazi / Do girls in your class swim in the
- Ingabe umngane wakho omkhulu uyakwenza lokho? yebo cha angazi
- Uyakwenza wena? yebo cha / Do you do this? (Yes, no)
- Ingabe uyazi siyini isichenene? yebo cha anginasiqiniseko /Do you know what Bilharzia is? (Yes, no, unsure)
- Ingabe kukhona emndenini onaso noma owake wabanesichenene yebo cha Angazi / Has anyone in your family ever had Bilharzia?
- Usuqalile ukuya esikhathini? Yebo cha /Have you started menstruating?
- Umbono kabani owazisa kakhulu mayelana nezophuza (ukusebenzisa utshwala) (abazali noma ogogo /ababheki abafowenu /odadewenu
- Wake wabuphuza utshwala? Yebo cha akukhompendulo /Have you ever drunk alcohol? Yes, no, NR
- Ubuphuza utshwala ezinyangeni ezintathu ezedlule? yebo cha akwenzeki /Have you been drinking alcohol the past 3 months? (Yes, no, NA)
- Ingabe abangani bakho bayazisebenzisa izidakamizwa? yebo cha angazi / Do your friends use drugs? (Yes, no, DK)
- Uyazisebenzisa izidakamizwa? yebo cha / Do you use drugs?(Yes, no) 3.Wake wasebenzisa
- Umbono kabani owazisa kakhulu mayelana nokuziphatha kwezocansi ? abazali umkhulu ogogo u bheki u owenu uda ewenu
- Wawungakanani ngesikhathi wenza ucansi lwesitho sowesifazane okokuqala ngqa? (iminyaka) / How old were you when you had vaginal sexual intercourse for the first
- Empilweni yakho usuwenze ucansi nabantu besilisa abangaki?
- Ezinyangeni ezintathu ezedlule usuwenze ucansi nabantu besilisa abangaki?
- Uke waphuza uphuzo oludakayo noma izidakamizwa ngaphambi kokuba wenze ucansi ngesikhathi ugcina? ebo cha NA / Did you drink alcohol or use
- Esikhathini sokugcina wenza ucansi ikhona indlela owayisebenzisayo ukuvikela ukukhulelwa? (khetha impendulo ibe yinye) / The last time you had sexual
- Ingabe kukhona owake wakunika imali, izinto noma wakwenzela okuthile ngokwenza ucansi?yebo cha / Has someone ever given you money, things or favours
- Ingabe kukhona owake wakuphoqa ukuba wenze ucansi? yebo cha
- Ezinyangeni ezingu 12 ezedlule uke wazizwa udangele uphelelwa yithemba cishe zonke izinsuku amasonto amabili noma ngaphezulu kulandelana
- Manje ngifuna sikhulume ngemizwa yakho esontweni eledlule
- Imibuzo elandelayo ingendlela ozizwa ngayo ngawe. Ngizofunda
Yes Yes Yes Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Ewe Hayi Hayi Ewe Hayi Ewe Hayi Ewe Hayi. Ngaba loo nto iya kukuyekisa ukuyenza kwakhona? Le mibuzo ilandelayo imalunga nempilo yakho. ewe hayi andiqinisekanga/ Ngaba uyazi ukuba yintoni na iBilharzia. I-14d Depo-Provera (inaliti yokuthintela ukukhulelwa) I-Depo-Provera (inaliti) Ewe Hayi 14e Ukuyeka Ewe Hayi 14f Ezinye iindlela (chaza) Ewe Hayi.