This study aimed to evaluate the effect of psychoeducation on medication adherence and symptom management for clients with bipolar affective disorder attending psychiatric clinics in Ethekwini Health District in KwaZulu-Natal Province. The clients were assessed in the areas of their knowledge, medication adherence and symptom management (Pre-test).
Background to the problem
The term 'psychiatric rehabilitation' is being routinely used in the mental health field (Anthony & Lieberman, 1986). The South African government acknowledges that mental health services have been neglected in the past.
Problem statement
Purpose of the study
Objectives of the study
Research question
Psychoeducation and medication compliance
Furthermore, unpleasant side effects and patients' denial of the presence or severity of the disease contribute to medication nonadherence (Crane et al., 1996). According to Powel, Yeaton, Hill & Silk (2001), successful disease management relies on understanding the diagnosis, the ability to make informed choices about treatment and the motivation to actively participate in the treatment process.
THEORETICAL FRAMEWORK
The knowledge that clients had about their illness, medication and symptom management after the course constituted/reflected the informational component of this model. In this study, the behavioral skills required were self-medication skills and symptom management skills, and the ability to strengthen and maintain these skills.

Conclusion
The group was then exposed to six sessions of psychoeducation, which covered the following topics: a) Bipolar affective disorder and the course of the disease, b) Medications and side effects of medications, c) Self-healing skills, d) Relapse and e) Symptom management techniques. However, the researcher conducted a pilot study on 10 clients with bipolar affective disorder who were not part of the study. The researcher also sought to control for identified extraneous variables in order to determine as much as possible the true nature of the relationship between the independent and dependent variables under investigation.
The variables controlled in this study were classified into respondent characteristics and external factors. If the clients in the experimental group were given any other information or education during the experiment. Clients with bipolar affective disorder attended six sessions of psychoeducation, which lasted one hour and thirty minutes, on the following topics: a) bipolar affective disorder and the course of the disease;.
Population
The initial setting of the study was Escoval House Community Psychiatric Clinic, but in the recruitment process. The Escoval House is located downtown, while the Austerville Clinic is located in the Austerville location. Every fourth file of a client with bipolar affective disorder was selected and included in the study until the required sample was reached.
Clients who agreed to participate in a six-week psychoeducational group and met the study criteria were included in the group and signed a consent form. The researcher administered the questionnaires to the participants and helped them understand the items in the questionnaire. The information took place in the waiting room of the clinic in the afternoon, when few clients came to the clinic.
Ethical considerations
Introduction
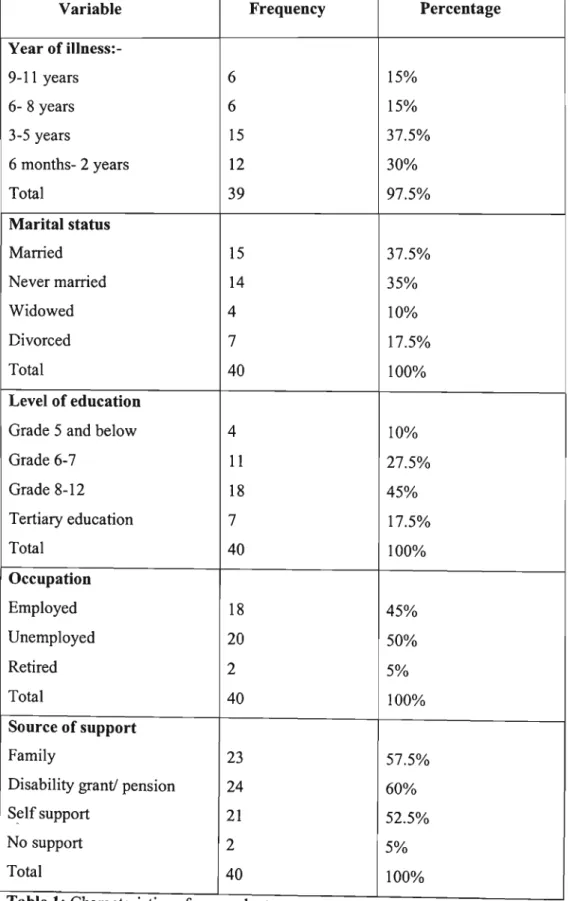
Sample realisation and description
Although this is the case, the response rate still varied from question to question as some respondents did not answer all questions in the pre-test as well as in the post-test findings.
Gender
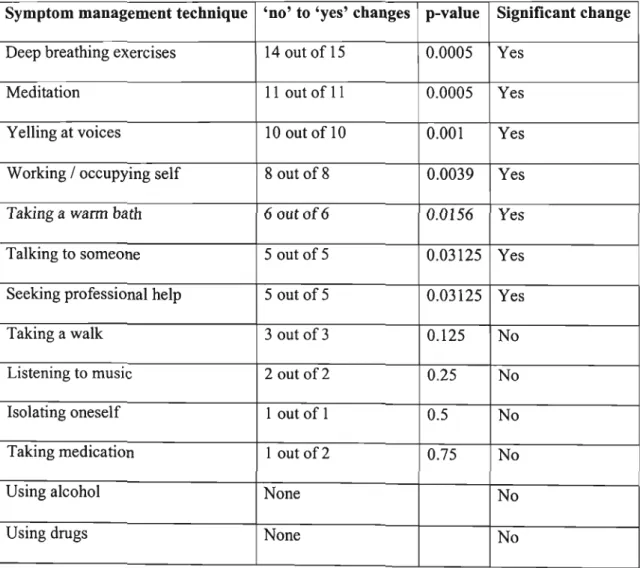
This was done because knowledge is the basis of any behavior change, including medication adherence and symptom management. The mean number of symptom management techniques known pre- and post-course are 4.81 and 6.93, respectively. A paired Hest shows that the course resulted in a significant increase in the mean number of symptom management techniques known (t=5.27 with a p-value of 0.000008).
The average number of symptom management techniques used before and after the course is 4.19 and 3.94 respectively. A paired Hest shows that the course resulted in a significant decrease in the mean number of symptom management techniques used (t= 1.488 with a p-value of 0.074 is weak evidence in favor of a decrease). The tables below summarize the results for t-tests for the difference between the means for the use of symptom management techniques before and after education for the four social variables considered.
Conclusion
In this study, a few social variables were selected and tested to examine their relationships with knowledge, medication adherence, and symptom management, because if they were not, they would contaminate the rest of the study. Although the number of female respondents is not equal to the number of male respondents, the difference is not statistically significant and this is consistent with literature indicating that the disorder affects both sexes equally (Griswold & Pessar, 2000). The findings of the study revealed that gender had no impact on the respondents' knowledge, medication adherence and symptom management with p-values < and 0.872 respectively). These p-values are greater than the set p-value «0.05), so they are not statistically significant. The study also revealed that marital status had no influence on the respondents' knowledge about their illness, their adherence to treatment and their knowledge and use of symptom management techniques to manage their illness with p-values < and 0.700. respectively).
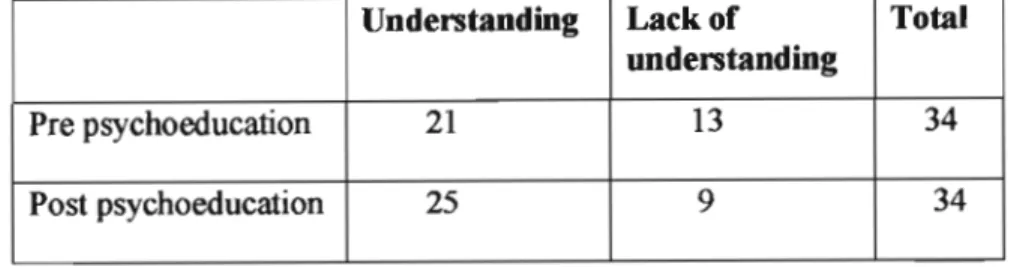
On the other hand, the findings of the study showed that the level of education had a significant influence on the respondents' knowledge and use of symptom management. The findings of this study showed that psychoeducation improved respondents' knowledge of mental illness in general with a p-value > 0.05. The research also revealed a significant change in respondents' knowledge of their diagnosis after training. The study also found that the number of respondents who did not know their diagnosis dropped from 7 to 2 after the training.
Medication compliance
Reasons for defaulting on treatment
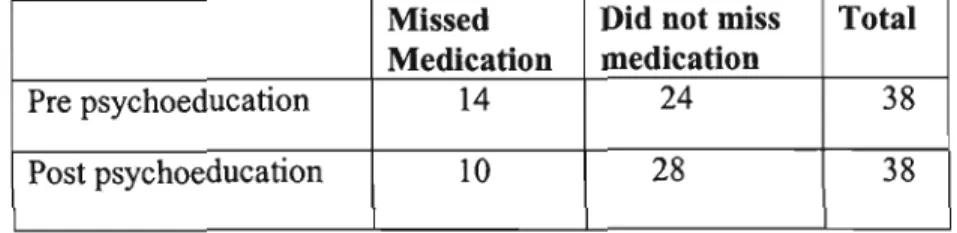
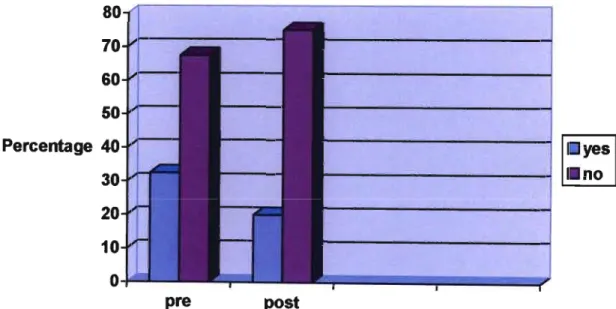
Some underlying factors for unintentional nonadherence include complex medication regimens that clients do not understand, inability to pay for medication, When clients understand their symptoms and need for medication, and also if they have clear and unambiguous instructions, they are more likely to take on increased responsibility for their own care, which can increase the likelihood of compliance with the regimen. medication (Crane et al, 1996). This study found that only one respondent missed medication intentionally (he did not want to take the medication) while the other five respondents stated that the reason for missing medication before education was that they had not visited the clinic when they were supposed to. . therefore, they had no medication. In this study.
Changes in medication regimens or complicated regimens are some of the main reasons for nonadherence to treatment (Lehne et al., 1994). In this study, only 8 respondents (20%) reported that their medication was changed during the psychoeducation period.
Attitudes towards medication
The results of this study in the area of use of symptom management techniques are not surprising, as there was no major relapse during the training period, therefore, even if the respondents had new knowledge and skills about symptom management techniques, the chances of using the new skills were. low. However, in the current study, it was noted that the training had no effect on manic symptoms experienced by the respondents. The results also revealed that there was a significant improvement in the symptoms of depression experienced by respondents after psychoeducation.
There is a need for other forms of psychoeducation to be researched in the South African environment, for example individual psychoeducation and family psychoeducation. Randomized study of family-oriented psychoeducation and pharmacotherapy in the outpatient management of bipolar disorder. An evaluation of the implementation and effectiveness of two treatment and organizational strategies in the rehabilitation of long-term psychiatric patients.
DATA COLLECTION INSTRUMENTS Questionnaire -1
Mark all that apply to you) and indicate in the dotted lines how often you take the medication you have marked. Indicate the extent to which you have felt or behaved in the past week by circling one of the numbers that follow.
TEACHING SCHEDULE FOR PSYCHOEDUCATION
Celebrate Relapse -What is Relapse 1:30 PM - Lecture - Flipcharts and - Early Warning Signs of 3:00 PM - Discussion Markers.
READING MATERIAL ON BIPOLAR AFFECTIVE DISORDER
Any or all of these can prevent relapse or reduce its severity (Royal Brisbane Mental Health Services 2001). It is important that you learn to distinguish warning signs from any persistent symptoms, and from medication side effects that you may experience. Many people have their own individual early warning signs that they and their families can recognize. If you think back on your previous relapse, you may be able to identify the warning signs that you didn't recognize as warning signs at the time.
Remember that the earlier your warning signs are detected, the more likely you can prevent a recurrence or reduce its severity. It's important to have a helper to help you recognize your warning signs of a relapse, help monitor the severity of your warning signs, and agree to tell you if they think you're feeling unwell. There are a number of strategies that can help you deal with the warning signs or symptoms of a relapse.
Ethical Clearance
KWAZULU-NATA
KWAZULU-NATAL
10 NOV 2004~S\Y
The title of the study is: Effects ofPsycbo edllQtioO00Medicatioo Compliaoce a.d Symptom Maoagemeot for Clieots withb Bipolar Disorder Atteodiog Escova. The study will involve six weeks of teaching sessions and participants will be asked to complete two. I am a student studying for a master's degree in Mental Health Nursing at the University of Kwazulu-Natal.
The study is looking at how education can help you manage your medication and the problems you have because of your illness. I will teach you about the disease you have and its treatment and management. The results of the study will be for academic purposes and can be used for future planning of programs in this clinic. You will be provided with money for transportation to and from the clinic on the day of the lesson.