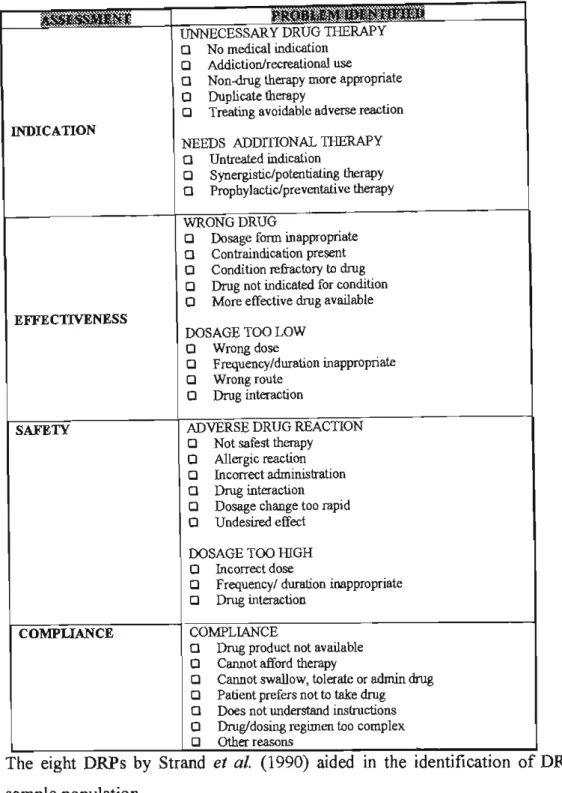
A Prescription Intervention Form (PIF) was used to inform the prescriber about DRP and to make recommendations to change drug therapy to overcome DRP. The most common DRPs were those dealing with drug safety (56.6%); effectiveness of drug therapy (20.8%);.
MOTIVATION FOR THE STUDy
Other studies have shown that 32,000 hip fractures and 16,000 car accidents resulting in injuries are caused by side effects in older patients each year. Drug-related problems (DRPs) are common among older patients in the community and hospitals and are responsible for hospital admissions.
AIMSAND OBJECTIVES OF THE STUDY
RESEARCH ATh1S
STUDY OBJECTIVES
CHARACTERISTICS OF DISEASE IN OLDAGE
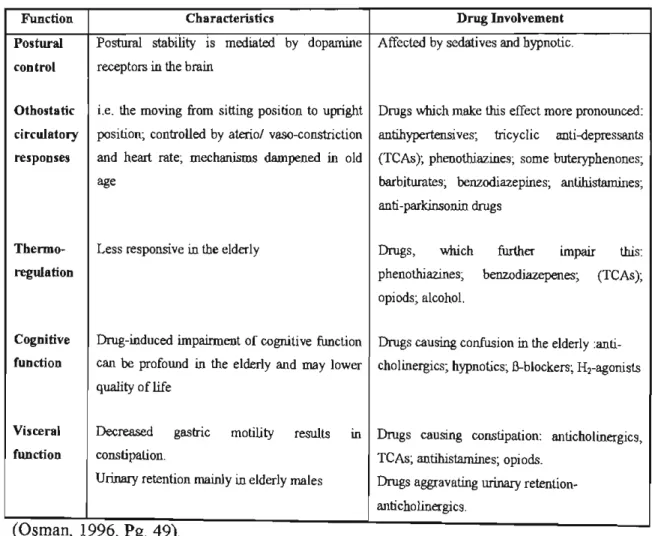
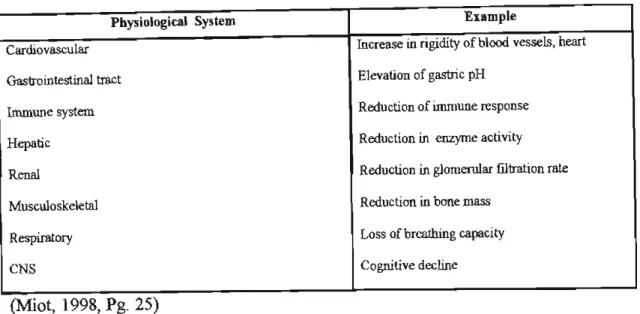
- PHYSIOLOGICAL SYSTEMS wmCH MAY BE AFFECTED WITH AGEING
- DRUG BIOA V AILABILITY AND AGEING
- PHARMACOKINETICS
- MULTIPLE PATHOLOGY INTHEELDERLY
- NON-DIAGNOSIS OF TREATABLE AILMENTS
Renal function is often impaired in the elderly, although there is great variability between patients. 1t12 may be prolonged in the elderly, which should be taken into account when determining the intervals between doses.
MEDICAL CONDITIONS OR DISORDERS IN GERIATRICS
- COMMON DISORDERS IN THE ELDERLY
- DISORDERS wmCHPRESENT ATYFICALLYINTHEELDERLY
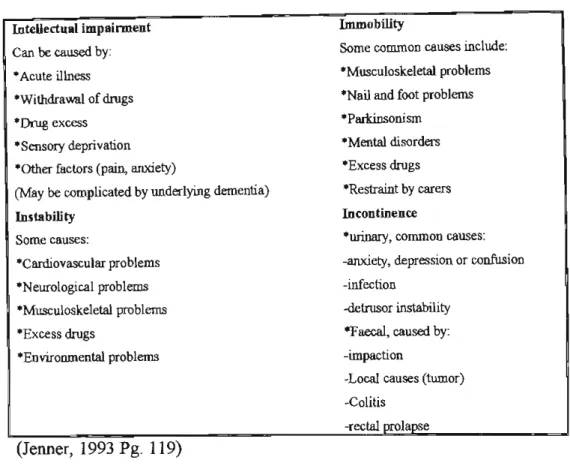
Bladder control problems are common in the elderly with urge incontinence being the most common type. In the case of the elderly, the primary objectives are to keep the patient asymptomatic.
DRUG-RELATED PROBLEMS IN GERIATRICS
- DRUG-RELATED PROBLEMS
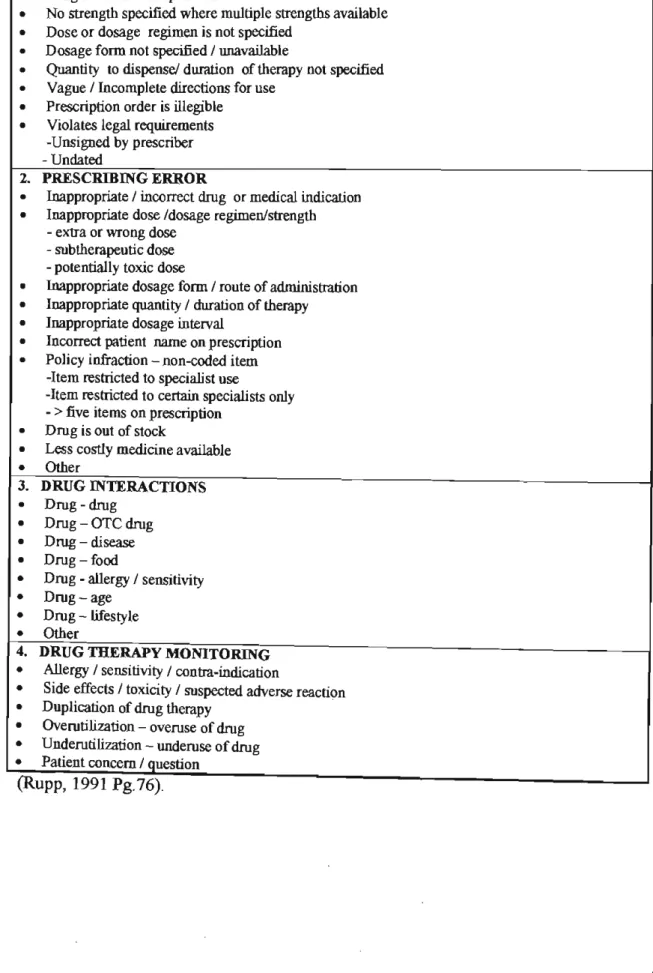
- CATEGORIES OF DRUG-RELATED PROBLEMS
- NUTRITIONAL DRUG-RELATED PROBLEMS
The use of tricyclic antidepressants in the elderly is not recommended due to anticholinergic side effects. Traditional doses of neuroleptics used in elderly patients may be too high and should be reduced.
POLYPHARMACY IN THE ELDERLY
- Factors contributing to polypharmacy
- Dangers of Polypharmacy
Pressures for increased drug use among the elderly will continue to increase with improved disease diagnosis and the marketing of drugs to treat symptoms and diseases. Use of inappropriate doses (eg, excessive doses of stronger diuretics, which can cause postural hypotension and cause falls in the elderly). The use of multiple medications in the elderly results in iatrogenic disease, drug interactions, and decreased medication compliance.
Although warnings about the use of multiple medications in the elderly are frequently sounded, pressure to prescribe even more drugs will continue in the future.
NONCOMPLIANCE IN THE ELDERLy
- Factors relating to Noncompliance in the Elderly
- Strategies to improve compliance
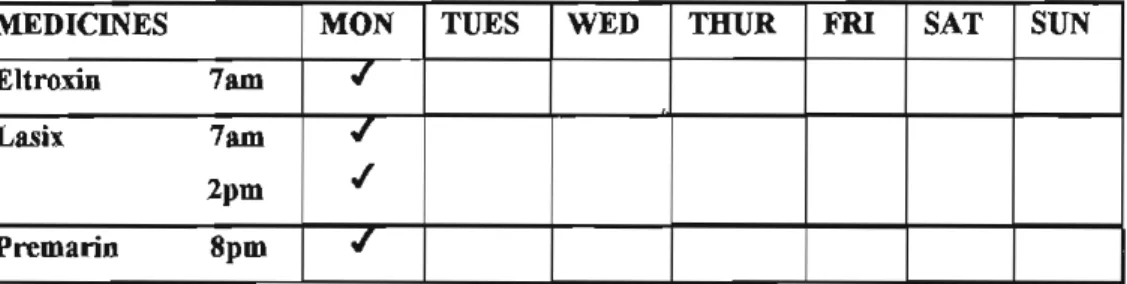
It is important that the patient feels that he is actively participating in the care of his health. Make sure the patient understands and accepts the diagnosis and the need for the medication and taking the medication as directed. Tactfully explore whether the patient has the ability to remember to take the medication and ways to improve the patient's memory for taking the medication.
The pharmacist is in a position to know which medicine the patient has been prescribed as well as which OTC.
PRESCRIBING ERRORS IN THE ELDERLy
- OVERCOMING PRESCRIBING ERRORS
Using a potentially toxic drug when one with less risk of toxicity would also work (eg, using phenylbutazone in patients with osteoarthritis or rheumatoid arthritis when other nonsteroidal anti-inflammatory drugs would be less dangerous). The most serious consequence of inappropriate prescribing in hospitals is the increase in the number and severity of adverse reactions. In preventing the misuse of geriatric drugs, the physician, pharmacist and patient each play an important role.
Too often, one or both of these critical elements are missing in elderly care.
PRESCRIPTION MONITORING FOR ELDERLY PATIENTS
- PRESCRIPTION MONITORING USING PRESCRIBING INFORMATION ALONE
- PRESCRIPTION MONITORING CRITERIA
By using bronchodilator prescriptions to identify elderly patients with airway obstruction, pharmacists can reduce unnecessary steroid side effects by ensuring that the patient's response is objectively assessed or monitored (eg, peak velocity of respiratory flow, spirometry, walking distance) and recommending discontinuation of steroids in non-responders. Atrial fibrillation (AF) is a known risk factor for stroke, and this risk is greater in elderly patients. Studies have suggested that III benzodiazepine use in elderly patients is often unnecessary and is associated with decreased cognitive impairment and hospitalization.
Evidence-based criteria for prescribing monitoring for older patients are listed in the 'Prescribing Guidelines for Geriatric Patients' (Appendix 4).
MONITORING GERIATRIC DRUG THERAPy
- Practical considerations in monitoring geriatric drug therapy
Older patients can also take responsibility for their own health through counseling and information about medication administration and the use of OTe medications (Jenner, 1993; Sause, 1996). Older people use more 'over-the-counter' drugs, possibly 40 percent of all daily medications. That is why the healthcare provider plays an important role in monitoring medication use in the elderly.
A challenge for primary care is the recognition of acute illness in the elderly with multiple pathologies and the good management of these complex patients.
PHARMACEUTICAL CARE OF THE ELDERLy
- THE PHARMACEUTICAL CARE APPROACH TO MEDICATION IN ELDERLY PATIENTS 71
- CHOOSING THE MOST APPROPRIATE DRUG TREATMENT FOR ELDERLY PATIENTS
- PHARMACEUTICAL CARE PROCESS FOR THE ELDERLY
Furthermore, unlike most existing pharmaceutical services, the pharmaceutical care process dictates that a written document be generated that captures the drug-related problems, the recommended solutions, and the patient-specific outcomes that actually result from the individualized pharmacotherapy. Regular monitoring of treatment, where possible by direct contact with the patient, is required to ensure compliance and appropriate periodic review. Treatment failure may be due to the patient not taking their medication within the proper schedule.
To complete the pharmaceutical care process, interventions must be documented and the patient's progress monitored (FIP Lisbon Congress, 1994).
INTERVENTION STRATEGIES TO OVERCOMEAND OR MINIMISE DRUG-RELATED
- Monitoring adverse drug reactions in elderly patients
- Maintaining patient records
- Educating elderly patients
- Communication regarding the discharge medicines of elderly patients
- Clinical Pharmacist Interventions
It is vital that ADRs occurring in the elderly are reported and the data shared with other clinicians. Through the collection and dissemination of ADR information related to elderly patients, advances in appropriate geriatric pharmacotherapy may be a more easily achieved outcome of drug therapy. Caregivers should also be involved in the discharge process and given information about discharge medications.
The clinical pharmacist in a regional hospital has a great opportunity to contribute significantly to an improvement in the quality of health care by providing advice on the appropriate and safe use of drugs.
STUDY DESIGN
IDENTIFICATION OF DRUG - RELATED PROBLEMS
STUDY POPULATION AND SAMPLlNG
- SITE OF THE STUDy
- THE STUDY POPULATION
- SAMPLE SELECTION AND SAMPLING TECHNlQUE
DATA COLLECTION AND MEASUREMENT
- RESEARCH INSTRUMENTS
- PILOT STUDY
- ETIIICAL CLEARANCE
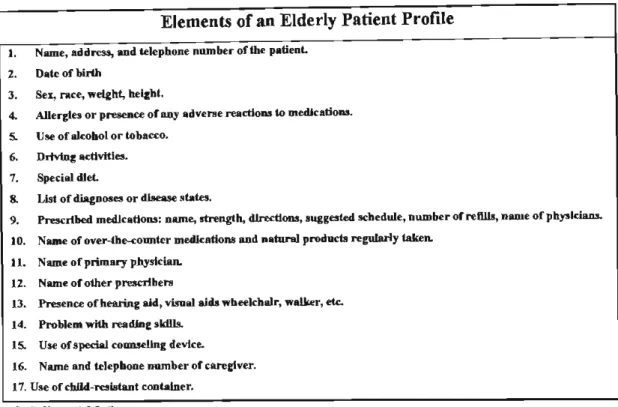
A detailed medication history was obtained from the patient's medical records and by interviewing the patient. The necessary data on the patient were classified into three groups: a) general characteristics of the patient (socio-demographic factors) (b) the patient's diseases, problems or symptoms and. A patient profile is outlined (Appendix I), which enables identification of inappropriate prescriptions (unnecessary drugs and drugs with absolute contraindications (Cl), interacting drugs of clinical importance) and side effects.
During the pilot study, problems were identified and the design and content of the patient profile were adjusted appropriately.
DATA PRESENTATION, ANALYSIS AND INTERPRETATION
- VARIABLES
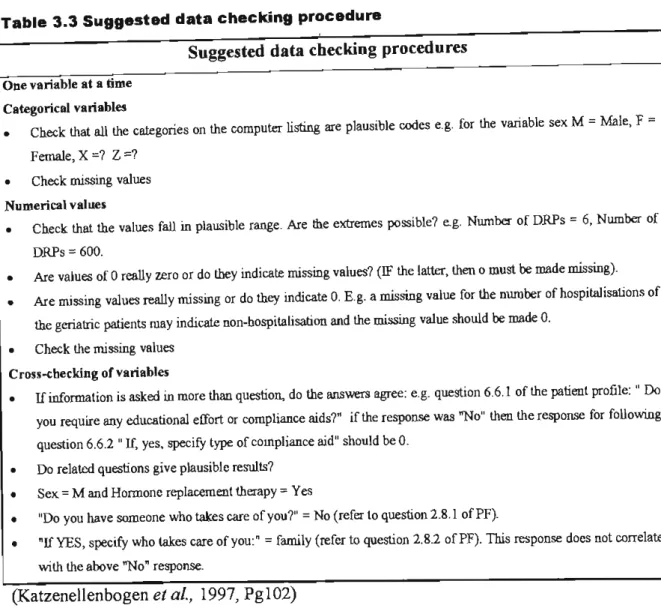
- DATA CHECKING BEFORE ANAL YSIS
- EXPLORATORY DATA ANAL YSIS
- SUMMARIZING THE SAMPLE DATA
- ESTIMATING THE POPULATION P ARAMETERS
- ANALYSIS OF PRESCRIPTION INTERVENTIONS
When any odd values were found, a list of the patient profile numbers of those cases was made. Graphical representations of categorical variables are primarily used to present geriatric study results. By examining the graphical representation of the data, the researcher decided which measures should be used to summarize the geriatric study data.
The most commonly used measure of centrality was the arithmetic mean or average (indicated by x).
INTERVENTION STRATEGIES
ASSESSMENT OF THE PATIENT COUNSELLING LEAFLET
The pilot study was conducted to allow for refinement of the research instruments, ie. Problems with the wording and clarity of the leaflet and the self-administered questionnaire were identified and these were modified. Unlike the geriatric patients in phase 1 of the study, it was not possible or necessary to apply the inclusion criteria listed in 3.2.3 to this sample population.
After explaining the purpose of the study to the selected patients, consent was obtained from them to participate in the study.
After completing the research instruments, they were distributed to geriatric outpatient clinics in the study itself. Ideally, one of the main intervention strategies would be to introduce routine counseling of all patients in the hospital about their medications. Therefore, it was decided to implement counseling of hospitalized patients in one of the medical departments as a pilot study.
One of the most common and potentially harmful or fatal ADRs is the adverse drug reaction.
PILOT STUDY
Determining the time it took to interview the patients helped establish an average of 15 patients interviewed by a single researcher per day. Drug-related problems were identified in twelve of the elderly patients (92%) interviewed in the pilot study. The pilot study DRPs will not be discussed in detail as this was not the purpose of the pilot study.
The results of the prevalence of DRPs in the pilot study assisted in the statistical determination of sample size.
GENERAL CHARACTERISTICS OF THE GERIATRIC PATIENTS
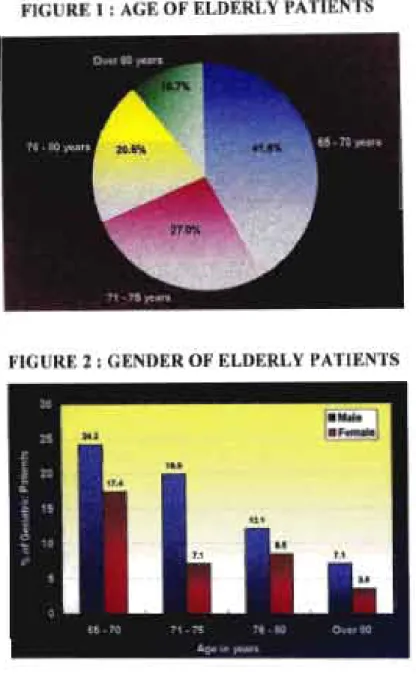
- PATIENT DEMOGRAPIllCS
- GERIA1RIC PATIENT'S BACKGROUND AND SOCIO-ECONOMlC
- ELDERLY PATIENTS LIFESTYLE OR ACTIVITIES
The education level of the older patients helped determine the literacy level of the population. The following table illustrates the results of older patients' ability to read, write and speak their first language. Healthcare providers play an important role in the supervision and administration of medications to older patients (section 4.7.2).
30.6% of the elderly patients consumed alcohol (Table 4.11), but very few admitted to consuming alcohol daily.
DISEASE PROCESS (ES) OF THE ELDERLY PATIENTS
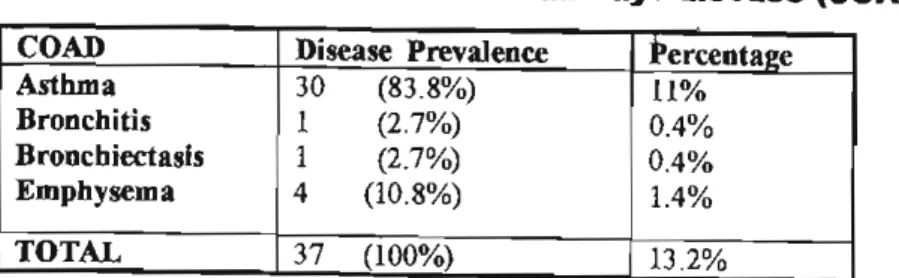
- PRESENT MEDICAL CONDmONS IN ELDERLY PATIENTS
- PHYSICAL IMPAIRMENTS OR DISABILITIES AND COGNmVE FUNCTION
- PAST MEDICAL msTORY
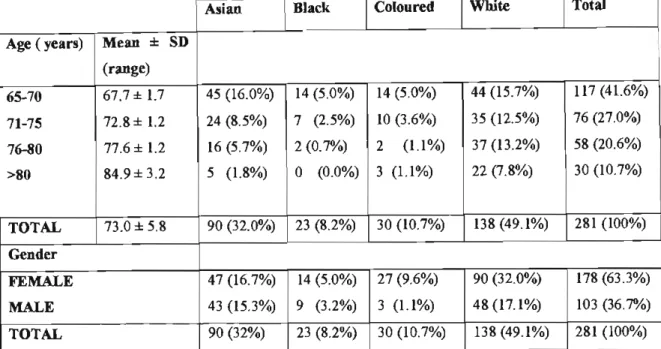
Prevalence of disease or symptom in elderly patients is a percentage of the total sample population (281). Impaired hearing (could not hear and needed hearing aids) was experienced by 50.5% of the elderly patients and impaired mobility (requiring the use of crutches or a wheelchair) by 59.1%. The majority of patients were female (63.3%) and 49.1% of patients were white in the total sample population.
30.6% and 12.5% of the elderly patients indicated that they had consumed alcohol and smoked cigarettes, respectively.
PHARMACOTHERAPY OF THE GERIATRIC PATIENTS
- OVERALL PRESCRIBING
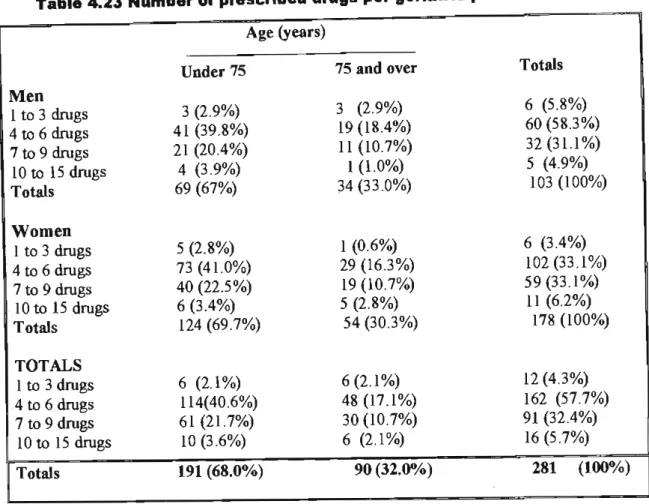
- NUMBER OF PRESCRIBED DRUGS PER ELDERLY PATIENT
- PRINCIPAL DRUG GROUPS PRESCRIBED
- USE OF MEDICATIONS OR SUPPLEMENTS OTHER THAN THOSE PRESCRIBED AT
- TOTAL NUMBER OF MEDICINES PER GERIA1RIC PATIENT
- TOTAL NUMBER OF OTC MEDICINES USED BY GERIA1RIC PATIENTS
- DISCUSSION OF DRUG THERAPY IN THE ELDERLY
157 blood and blood organ drugs were prescribed (9.1%) from the total number of drugs prescribed (Table 4.26). Anti-infectives were prescribed only in 8 cases (Table 4.30) and represented only a small percentage (0.5%) of the overall drugs prescribed (Figure 6). They accounted for 79.3% of the total number of drugs acting on the musculoskeletal system and 6.8% (Figure 6) of the total number of prescribed drugs.
Drugs acting on the sensory organs comprised only 2.5% of the total prescribed drugs (Figure 6).
DRUG RELATED PROBLEMS IN THE GERIATRIC PATIENTs
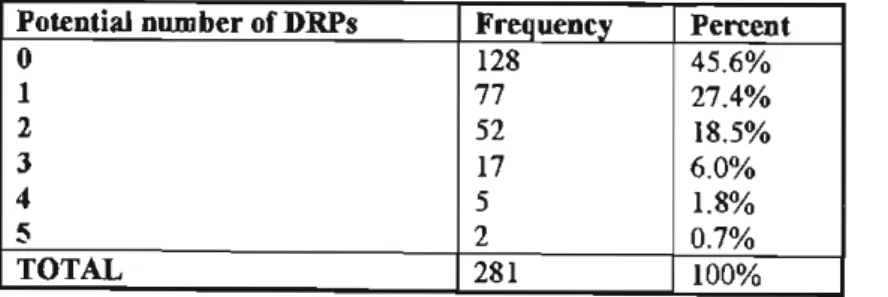
- INCIDENCE OF DRPs IN GERIA1RIC PATIENTS
- TYPES OF DRUG RELATED PROBLEMS
The patient had reported this to the prescribing physician at the consultation, and the dose was changed to Prednisone 10 mg daily for one month. A PIF was sent to the prescribing physician to review the patient's treatment and discontinue carbamazepine for reasons listed above. The prescriber taking a more careful medical and medical history of the patient could have prevented this.
In thirteen of the cases listed in Table 4.43, the patient was sent back to the prescriber and medication was prescribed to treat the necessary condition.
ADVERSE DRUG REACTIONS EXPERIENCED BY THE ELDERLY PATIENTS
- INCIDENCE OF ADRs FOR BOTH CURRENT AND PAST MEDICINES
- ACTUAL ADRs IN RELATION TO NUMBERS OF PRESCRIBED DRUGS
- TYPES OF ADRs
- RESPONSE TO ADVERSE SYMPTOMS
- DICUSSION OF ADVERSE DRUG REACTIONS
MEDICATION COMPLIANCE IN THE ELDERLY PATIENTS
PRESCRIPTION INTERVENTIONS
- NUMBER OF PRESCRIPTION INTERVENTIONS
- DRPs WARRANTING PRESCRIPTION INTERVENTIONS
- DISCUSSION OF PRESCRIPTION INTERVENTIONS
INTERVENTION STRATEGIES TO OVERCOME DRPs
- PATIENT INFORMATION LEAFLET
- PRESCRIBING GUIDELINES
- COUNSELLING OF DISCHARGE PATIENTS ON THEIR MEDICINES
DRUG-RELATED PROBLEMS SURVEILLANCE SySTEMS
GENERAL RECOMMENDATIONS ON STRATEGIES TO OVERCOME DRPs IN
RECOMMENDATIONS TO ADDINGTON HOSPIT AL AND THE PHARMACEUTIC AL
FUTURE RESEARCH