Differences were found between the types of workplace violence perpetrated by doctors, nurses and hospital managers. These were found to have influenced each of the participants in this study in relation to their experiences of workplace violence.
Background to the study
The experience of workplace violence appeared to be the same for the majority of study participants. The episodes of workplace violence ranged from verbal abuse and rudeness to malicious gossip, intimidation and physical violence.
Problem statement
King (2005a) argues that having a clearly localized picture of nursing staff's experiences in the workplace facilitates the development of interventions to maintain nursing staff's services. As nursing staff work in a variety of contexts, each with their own unique workplace dynamics and stressors, the researcher intends to delineate the field of study regarding the phenomenon of workplace violence and to study the phenomenon in a specific context (see below). .
Purpose of the study
Research objectives
Research questions
Significance of the study
Operational definitions
Workplace experience: in this study, 'workplace experience' refers to both the material and non-material aspects of being an employee within an organization.
Conclusion
Introduction
Definitional disputes
Lehane's (2005) views are further complemented by Gen-it Van Wyk's (2003) arguments in a South African study of workplace trauma. In addition to collegial acts of violence and aggression, Jackson et al. 2002) have further argued that violence in nursing does not occur in isolation, and that organizations play a central role in the perpetuation of workplace violence.
Psychological sequelae and support
Most respondents attributed the main cause of workplace violence to poor staffing conditions (lack of staff) (MNA, 2005b). A limitation of the study by Kwok et al. (2006) is that there are no clear recommendations regarding the management and limitation of workplace violence in nurses.
South African specificities
While this study demonstrates that workplace violence against nurses is a major problem in Hong Kong, it was further evident that a large proportion of study participants (42%) had a modus operandi when faced with an incident of workplace violence. ignored. King's (2005a) study also found that male registered nurses' experiences of workplace violence differed from those of their female colleagues.
Under-reporting of nursing workplace violence
When faced with verbal abuse from doctors and nursing colleagues – usually from senior colleagues, the majority of participants in King's (2005a) study reported feeling dissatisfied with the situation but feeling powerless to do anything about it. because if they reported to management they would either do nothing or they would be labeled as "troublemakers". In private hospitals, participants felt that nothing was done about these incidents because of the management's attitude that doctors are customers and nurses are just employees who have to keep working and go the 'extra mile'.
Financial implications of workplace violence
He notes that the consequences of workplace violence, and especially of workplace bullying, are too costly for employers to ignore. Considering the above and in relation to the specific domain in which this study is situated, Pieterse (2006) notes that in South Africa, although it is not difficult for healthcare organizations to find medical and surgical staff to utilize their facilities not, it is becoming increasingly difficult to find skilled perioperative practitioners (theatre nurses).
Strategies to prevent and manage workplace violence in healthcare settings Workplace violence in nursing does not occur in isolation - organisations have a central
However, Fisher (2005), in an article commenting on workplace violence prevention in the United States, notes that despite the fact that OSHA requires it. Fisher (2005) argues that these assumptions are incorrect, further noting that an incident of workplace violence is almost always premeditated; and is usually preceded by.
Limits of interventions
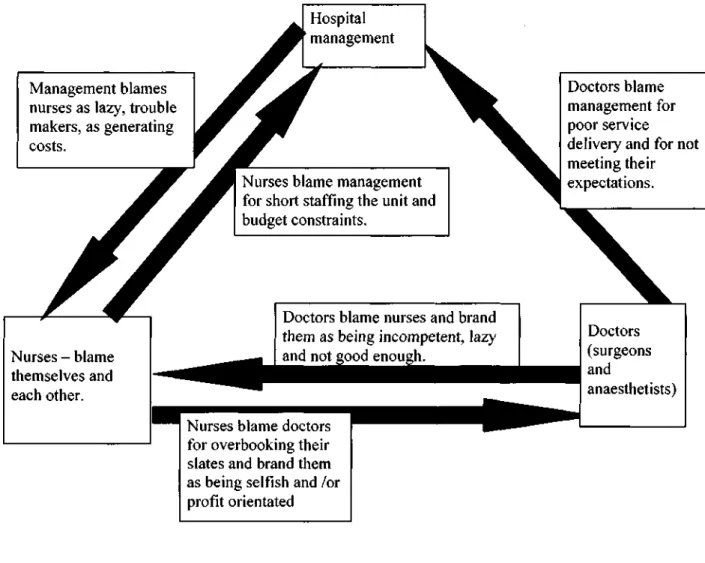
McKoy and Smith (2001) note that the situation is further exacerbated by the organizational dynamics of the 'blame triangle', in addition to facing an emotional dilemma regarding whether to report an incident of workplace violence. They argue that a radical (organizational) cultural shift is needed so that the drivers of the violence are recognized and corrected (Paterson et al., 2005).
Legal Aspects of Workplace Violence
While it is clear that a victim of nursing workplace violence may be able to invoke the doctrine of negligent employment in workplace violence situations involving fellow nurses, it is clear that the application of this doctrine to the sector Private healthcare in South Africa can be difficult. In terms of the doctrine of the voluntary assumption of the duty to protect, employers are obliged to provide adequate safety in the workplace (McKoy & Smith, 2001).
Conclusion
In reviewing the available literature regarding the context and type of incidents of workplace violence reported internationally and nationally, it appears that many of the factors associated with incidents of type II violence in the nursing workplace appear to are global in nature, e.g. Unlike Type II incidents of workplace violence, reported Type III incidents suggest that workplace violence is fueled and perpetuated by the environment in which nursing staff work (Pieterse, 2006).
Introduction
Research strategy and approach
Crotty (1996) also argues that the interpretive phenomenological method reveals the meaning of human experience in its situated context and that the approach enables the researcher to describe and interpret the meaning of the subjective experiences of each of the study participants in relation to their individual contexts. Thus, in this study, the researcher intended to make understandable the lived experiences of workplace violence among theater nursing staff.
Sampling design
This study was conducted in a private hospital in the DMA, which was purposefully selected as the research setting. Thus, this researcher stated that a private hospital was the preferred setting to investigate the phenomenon of workplace violence.
Selection of participants
- Participant demographics
All participants had obtained a Diploma in Operative Theater Nursing as a post-basic qualification. Regarding the nursing hierarchy, the participants represented the level of professional (registered) nurse.
Data collection process
- Setting and interview process
- Field notes
- Difficulties experienced in conducting the research
A synthesis of the field notes regarding the verbal and non-verbal communication of the participants proved that the majority of the participants were uncomfortable. The researcher and several of the participants decided that it would be easier to interview them at their place of work.
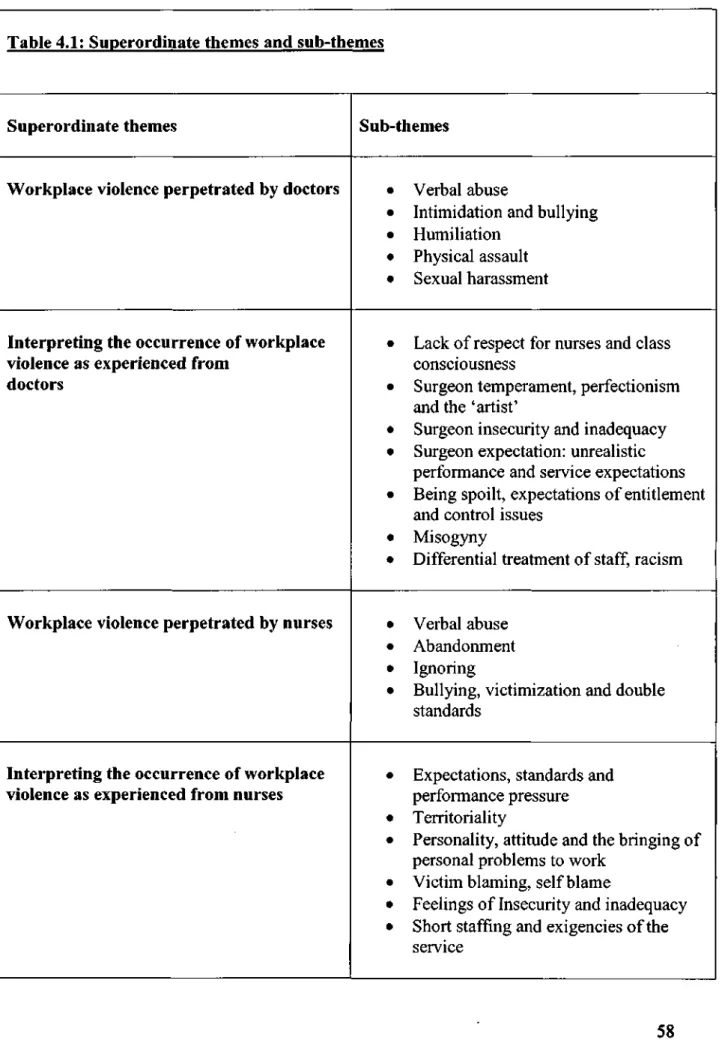
Data analysis
The researcher read and reread each transcript several times, using the left margin to record initial thoughts, observations, associations, and tentatives. interpretations in response to the text and the right margin to document new thematic titles and/or keywords that captured the "essential qualities" of the material. After reducing the data for each transcript in this way, the researcher produced a master list of themes which contained both overarching themes and sub-themes.
Ethical considerations .1 Negotiating consent
Via the theater manager and theater secretary who informed their staff of the research undertaking and thus formally established the researcher's credentials;. The cover letter from the participant (see Appendix Seven) explained the nature of the research study and emphasized that participation in the study was voluntary.
Trustworthiness of the research
Credibility was further enhanced by having the researcher present the data, data analysis and conclusions drawn for 'peer review'. Mutual debriefing' involved the researcher presenting the data (transcripts), data analysis and conclusions to the researcher.
Introduction
WORKPLACE VIOLENCE PERPETRATED BY DOCTORS
- Verbal abuse
- Intimidation and bullying
- Humiliation
- Physical assault
- Sexual harassment
And when she looked up, he stood in front of her and said to her "has anyone ever thrown a scalpel at you?" - because she was charging in his theater. Most of the participants had experienced intimidation and harassment from some of their medical colleagues.
INTERPRETING THE OCCURRENCE OF WORKPLACE VIOLENCE AS EXPERIENCED FROM DOCTORS
- Lack of respect for nurses and class consciousness
- Surgeon temperament, perfectionism and the 'artist'
- Surgeon insecurity and inadequacy
- Surgeon expectation: unrealistic performance and service expectations Additional explanations for surgeon behaviour related to their having unrealistic
- Being spoilt, expectations of entitlement and control issues
- Misogyny
- Differential treatment of staff, racism
It was noted by several participants that the staff working in the operating room were treated differently by the doctors. For one of the focus group participants it was clear that perceptions of hierarchy and.
WORKPLACE VIOLENCE PERPETRATED BY NURSES
- Verbal abuse
- Abandonment
- Ignoring
- Bullying, victimization and double standards
Abandonment and ignoring were process types of workplace violence evident in the accounts of a number of participants. Bullying behavior was evident in certain incidents described and especially in the stories of Sr B and Sr F.
INTERPRETING THE OCCURRENCE OF WORKPLACE VIOLENCE AS EXPERIENCED FROM NURSES
- Expectations, standards and performance pressure
- Territoriality
- Personality, attitude and the bringing of personal problems to work
- Victim blaming, self blame
- Short staffing and exigencies of the service
A large number of participants attributed their experiences of workplace violence to the territorial attitudes and behavior of certain nursing colleagues. A number of participants felt that their experiences in the workplace were mediated by the personalities and attitudes of their nursing colleagues, and had some understanding of incidents of workplace violence (verbal abuse) that were perceived to be caused by tensions and conflicts. tensions due to a colleague's circumstances, e.g.
HOSPITAL MANAGEMENT AND WORKPLACE VIOLENCE
- Victim blaming
- Lack of support and fobbing off of staff complaints
- Grievance procedure
For some participants, their stories revealed that they were typically blamed for workplace violence by management. Contrary to the above, the handling of the recent sexual harassment incident by the theater and hospital management appears to have been better managed.
INTERPRETING MANAGEMENT'S HANDLING OF WORKPLACE VIOLENCE INCIDENTS
- Fiscal considerations
- Social considerations and other vested interests
EFFECTS OF WORKPLACE VIOLENCE FOR THE SELF
- Doubt, loss of confidence and self esteem
- Loss of trust
- Avoidance, Resentment
- Stress, exhaustion, and being mentally drained
I come to work, I do my job - and it's not supposed to be a place where I get hurt. This is supposed to be a safe place - this is my workplace, where I was supposed to be protected, my rights were taken away and I was attacked.
STRATEGIES FOR COPING WITH WORKPLACE VIOLENCE
- Keeping the peace, keeping quiet, stoicism
- Prayer and professionalism
- Avoidance and withdrawal
- Intellectualization, rationalization, minimization
- Over-compensation and humour - the 'court jester'
- Venting to colleagues, support networks, crying and comfort eating
- Altruism, ethical conduct, and honesty
The prayer seemingly distanced the participant from the unpleasantness of the situation and thus made it more manageable. It was found that the participants concerned did not have a support network outside the workplace that they could rely on for support and understanding regarding the possibility of voicing their grievances and/or reporting an incident of workplace violence.
Introduction
What are the direct (personal) and indirect (witnessed) experiences of operating theater nursing staff regarding workplace violence. Third, the discussion focuses on participants' understanding of workplace violence in relation to participants' coping strategies.
Direct (personally experienced) and indirect (witnessed) experiences of operating theatre nursing personnel of workplace violence
As mentioned in chapter four, it was clear that particular surgeons were largely responsible for the verbal abuse and that this had significantly affected the working environment of the staff - so that no member of staff was comfortable working in those theaters with those surgeons, and. Where doctors are regarded by hospital management as customers, this study posits that this also fosters unrealistic expectations of service delivery and the entitlement of doctors, and that management in turn reinforces these notions to the detriment of their nursing staff. .
Meanings given by operating theatre personnel to their experiences of workplace violence
- Intrapersonal level
- Interpersonal level
- Institutional Level
On the interpersonal level, a number of the participants attributed their experiences of workplace violence to the territorial attitudes and behavior of particular nurses. Most of the participants also attributed the behavior of certain of their medical colleagues to the fact that they had been 'spoiled' by the nursing staff over the years.
Understandings of workplace violence
- Perceptions of workplace violence
- The blaming triangle
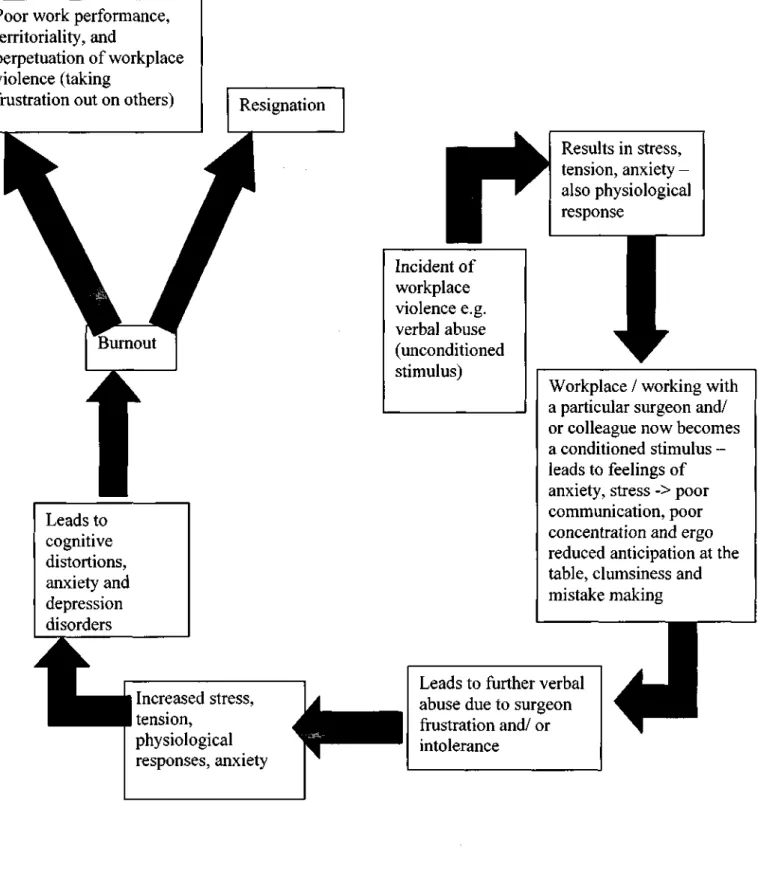
From the participants' narratives, it was further evident that incidents of workplace violence in the theater were underreported. The above findings suggest that theater nurses may experience workplace violence in the form of a cognitive-behavioural triad.
Coping strategies
The end results of the above can be poor job performance, territorial behavior and perpetuation of violence in the workplace by transferring frustrations to others and/or resignation of the nurse concerned (see diagram 5.5.2). As noted above, the potential consequences for theater nurses in the absence of theater workplace violence intervention are burnout, resignation or perpetuation of a cycle of workplace violence due to frustration, territoriality and/or poor job performance.
Introduction
Participant expectations and workplace violence prevention programmes In this study all of the participants emphasized the need for management to be proactive
However, the researcher believes that despite the complexity of organizational dynamics, the organization in this study must play a central role in eliminating, limiting and controlling workplace violence. First, there is an awareness phase that is used to sensitize role players to the prevention of workplace violence and the need and benefits of changing the status quo.
Recommendations for hospital management
Adopting policies that promote transparency regarding the management of workplace violence and ensure that stakeholders are given feedback. Implement programs that educate nursing staff about workplace violence and that promote self-confidence, anger and conflict management training.
Recommendations for the nursing profession
Ensure that all nurses and especially theater nurses are trained in complaints procedures and secure management support in relation to workplace violence and/or discriminatory practices. Provide a support structure for theater nurses to help contain and deal with workplace violence, e.g.
Recommendations for further research
Additional considerations, specific methodological critiques and strengths The broad limitations of this study are associated with the small scale of the study and to
The demographics of the participants further prove that each of the participants in this study had a tertiary education degree. The researcher states that all the above measures enabled the participants to convey the subtleties of their subjective experiences and the meanings associated with them and that the participant accounts derived in this study are suitable for IPA.
Conclusion
- Additional Readings
Integrative literature reviews and meta-analyses - nursing shortages in the United States: an integrative review of the literature. Workplace violence prevention and action: being assaulted is NOT part of the job, no matter where you work.
APPENDICES
- Appendix One: Focus group and interview schedule Setting the scene
How do operating theatre nursing personnel understand workplace violence?
What are the direct and indirect experiences of operating theatre nursing personnel in respect of workplace violence?
What meanings are given by operating theatre nursing personnel to experiences of workplace violence?
How do operating theatre nursing personnel manage experiences of workplace violence?
What are the direct and indirect experiences of medical staff in operating theaters regarding workplace violence.
How could workplace violence in the operating theatre be effectively contained and managed?
34; Exploring the experience of workplace violence against nursing staff in a private hospital in the Durban Metropolitan Area. RESEARCHER SHOULD ENSURE THAT THE QUESTIONNAIRE CONTAINS A SECTION AT THE END TO BE COMPLETED BY THE PARTICIPANT (PRIOR TO COMPLETING THE QUESTIONNAIRE) INDICATING THAT HE/SHE HAS BEEN INFORMED ABOUT THE NATURE AND PURPOSE OF THE PROJECT AND THAT THE INFORMATION PROVIDED WILL BE KEPT CONFIDENTIAL.
KWAZULU-NATAL
Appendix three: Letter requesting permission for the study to the Department Of Health
Exploring the experience of workplace violence against nursing staff in a private hospital in the Durban Metropolitan Area (DMA). EXPLORING THE EXPERIENCE OF WORKPLACE VIOLENCE ON CARE STAFF IN A PRIVATE HOSPITAL IN THE DURBAN METROPOLITAN AREA (DMA).
Appendix five: Letter requesting permission for the study to health care institution
The benefit for XXX Hospital will be mainly in terms of the results obtained - and how they can be applied by middle and senior hospital management to the recruitment and retention of nursing staff in the operating theatre. Please contact the unit manager, Sri bn extension 1 It to make reservations for the use of the room.
Appendix seven: covering letter to participants advising them about the study and inviting them to participate and consent form
The focus group will consist of 4-6 nursing colleagues who work with you in theatre. A copy of the dissertation will be given to the Ministry of Health and the hospital management.
RESEARCH STUDY CONSENT FORM
Appendix eight: workplace violence poster - calling for participants for the focus group
WORKPLACE VIOLENCE