A number of papers have established the positive impact of the program on various socio-economic indicators of participants and the positive spillover to non-participants. Further discussion of the consequences of malnutrition is available in Isabel and Correla et al. However, the use of safe sanitary facilities such as with a running flush, pit latrine and composting toilet is limited to only a third of the rural population (National Institute of Population Research and Training (NIPORT) et al. 2013).
We first assess the impact of the CFPR on the nutritional status of participating household members and then investigate spillover effects to non-participants. Prevalence effect sizes for preventive care ranged between 12% and 80% of the main effect among outcomes.
CFPR PROGRAMME AND PATHWAYS OF SPILLOVER EFFECTS
All training sessions are conducted on a one-to-one basis, usually within the confines of the participant's home. The CFPR creates an inflow of agricultural assets in the treated communities, brings about a shift in the hours devoted from wage to self-employment among the poorest women in the community and increases self-employment output (eg milk, eggs) in the local markets. 2012) claim this causes spillover effects in local wages, output and livestock prices, leading to changes in the local market equilibrium. The spillover effects studied in this paper are more behavioral in nature and we hypothesize pathways through which they can occur. As the CFPR revolves around repeated dissemination of messages through in-depth and repeated training sessions on various topics to ensure information retention.
Social networks and “word of mouth” are quite fluid in rural communities and information is transmitted through households within similar socioeconomic strata (Banerjee et al. 2013; Scott, 2012). The importance of knowledge gained through interventions results in explicit or implicit signaling by participants, and its knock-on effects can induce “demonstration effects” among non-participating families (Handa et al. 2001; Miguel and Kremer 2004).
DATA AND METHODS
EVALUATION DESIGN AND DATA COLLECTION
VARIABLES
General household characteristics include whether the household has access to sanitary latrines and safe drinking water.
BASELINE CHARACTERISTICS
Using this framework as a guide, we assess the impact of CFPR on a number of intermediary outcomes hypothesized to influence the nutritional status of members in participating and non-participating households: initiation and duration of exclusive breastfeeding13, vitamin A supplementation (for children) between 6 and 59 months old) and disease incidence in the 15 days preceding the survey. The assessment tool collected detailed information related to demographic characteristics such as household composition, gender of the household head and household size. Socio-economic information detailing education and employment status of all household members, including sources of income with a 12-month recall period.
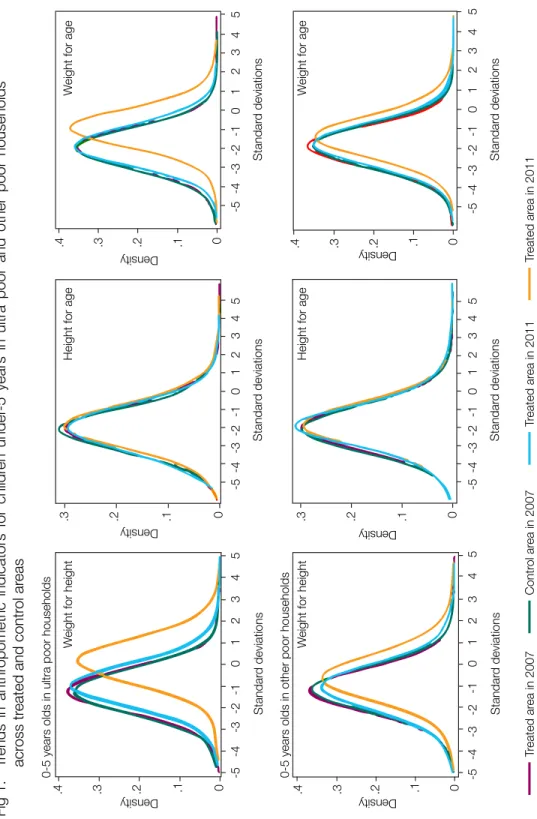
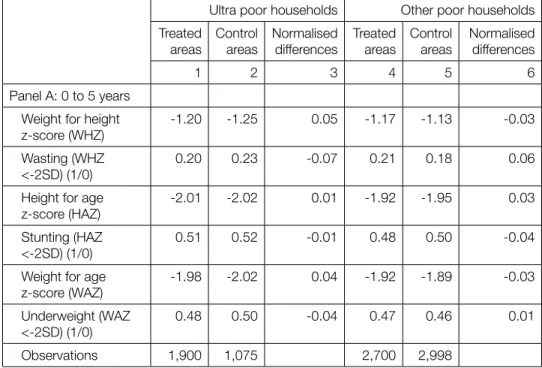
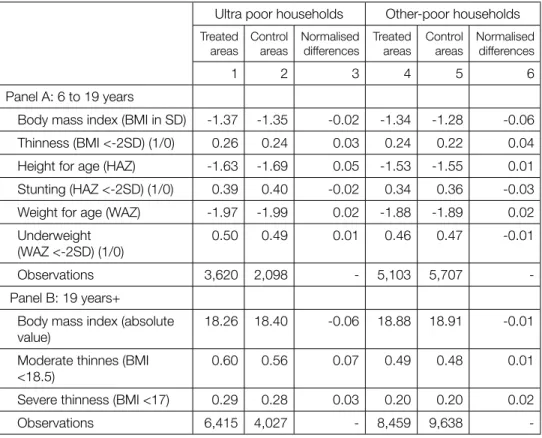
A comparison of the baseline means shows that a UP household head is more likely to work as a casual daily laborer in the treated areas than in the control group (46% vs. 30%). Similarly, for OP households, none of the differences in the covariates differed significantly between treated and control areas. Trends in anthropometric indicators for children under 5 years of age in ultra-poor and other poor households in treated and control areas.
EMPIRICAL STRATEGY
ANALYTICAL TECHNIQUE
In model (2), it gives the unique average effect of CFPR per female respondent in a female-headed household. The average effect in the treated areas is obtained by averaging the partial effect of the CFPR in the treated areas and subsequently combining with and. Similarly, the impact on individuals in female-headed households ( ) is given by averaging the partial effect of the CFPR in the treated areas for a specific subgroup.
Standard errors are estimated using the delta method and clustered at the branch level. To deal with type 1 error (α) due to multiple hypothesis testing, the critical value at which the null hypothesis is rejected is adjusted downward using the Bonferroni correction procedure (Gibson et al.
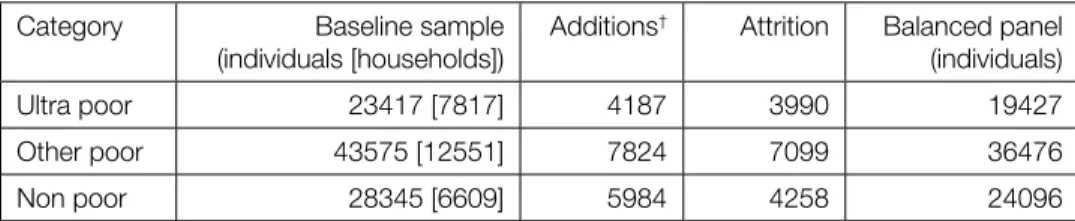
ATTRITION
Attrition could affect our effect estimates if it is associated with unobservable temporal variables that are also correlated with treatment. To test for attrition bias, we use the Verbeek and Neijman (1992) test, where we add the leading selection indicator (1) to the DiD model. and test the significance of this indicator (Jones et al. 2013). The results suggest that the dropout is random, as no or no effects were rejected for any of the outcomes (results available upon request).
RESULTS
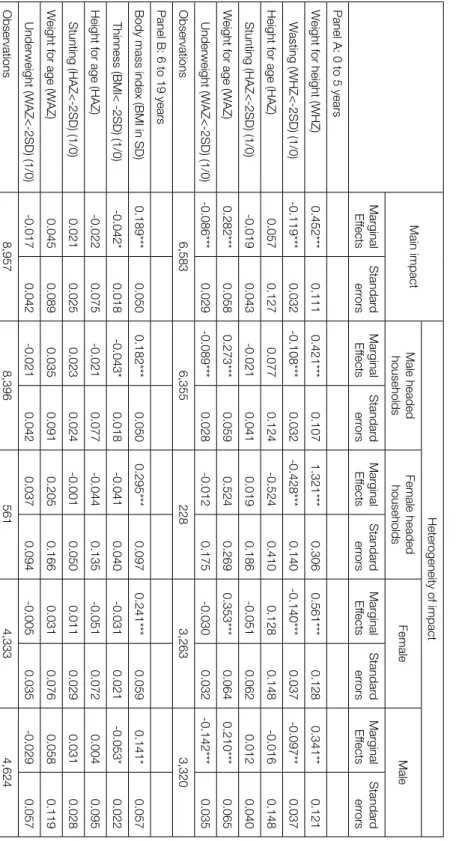
IMPACT OF CFPR ON PARTICIPANT HOUSEHOLDS
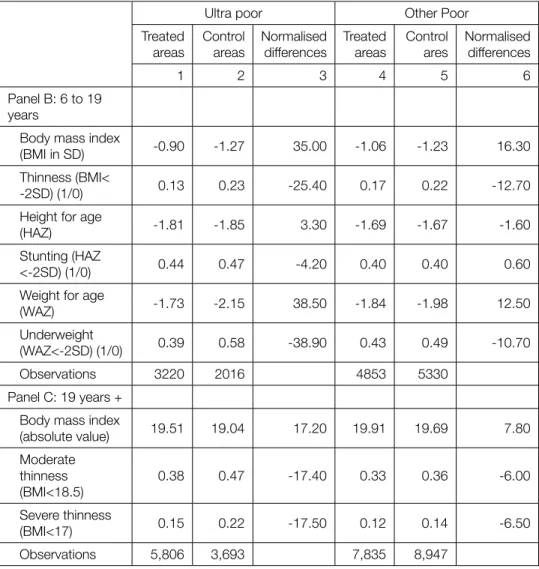
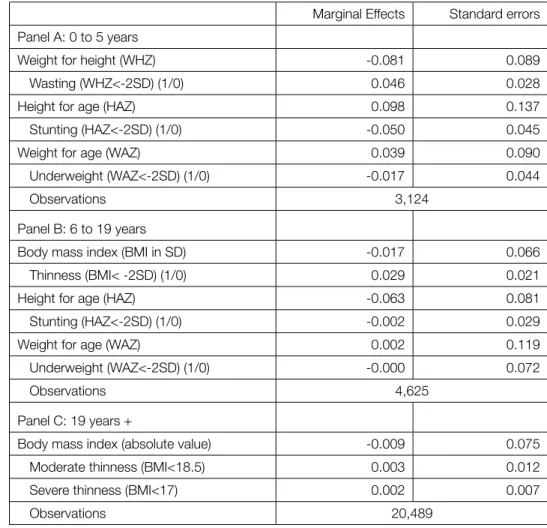
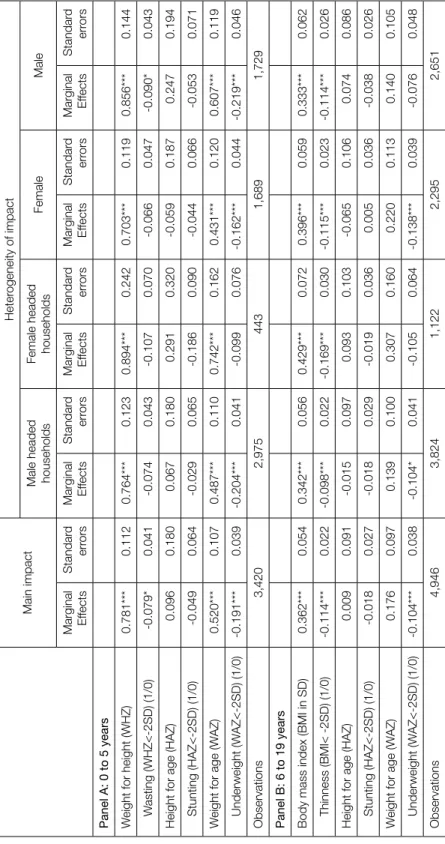
Results for the 20+ year group show absolute values of BMI and binary scores (BMI<18.5 and BMI<17.5) indicating moderate and severe frailty. The critical values at which the null hypothesis is rejected are adjusted using the Bonferroni correction. Bold type indicates significant differences between male-headed and female-headed households; and between male and female respondents at the 10% level.
SPILLOVER EFFECTS OF CFPR
Male headed households Female headed households Female Marginal effects Male Standard errors Marginal effects Standard errors Marginal effects Standard errors Marginal effects Standard errors Marginal effects Standard errors.
PATHWAYS OF SPILLOVER EFFECT IN NON-PARTICIPANT CHILDREN
If duration of breastfeeding is an important pathway for the dietary impact of CFPR, we should see greater effects of CFPR in children younger than 24 months. We investigate the heterogeneity of the impact between two age groups: 0–24 months and 25–60 months (see Appendix A7) and find that underweight for height and probability of being underweight are actually more strongly affected in the younger group (0 -24 months) between UP and OP households. Differences in the magnitude of impact for ultra-poor and other poor households are comparable to the main findings.
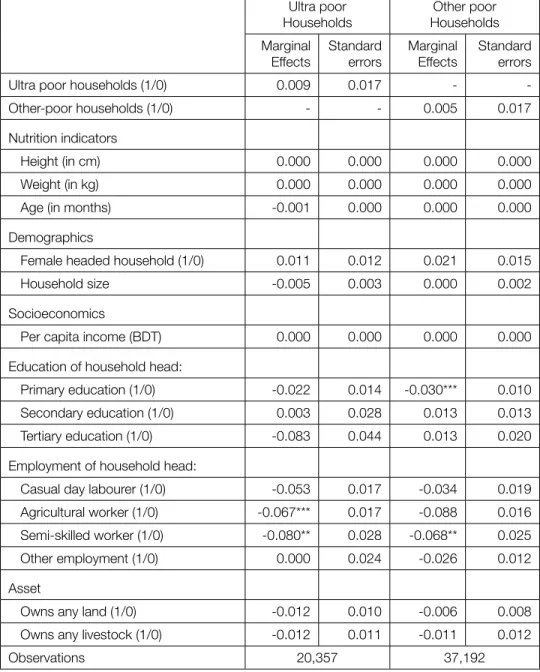
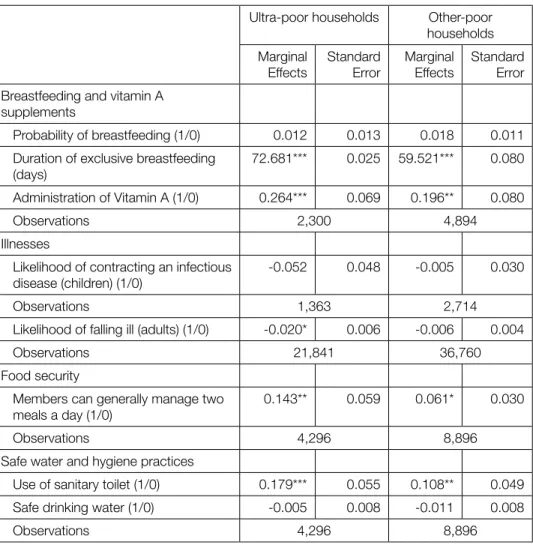
The results represent the impact of the CFPR on intermediate outcomes that may affect the nutritional status of ultra-poor and other poor households, and the sample is limited to households with children under 5 years of age. Adults in ultra-poor households are 2 percentage points less likely to get the disease, although no effect is seen among other poor adults. In terms of food security, however, both groups experience an increase in the probability that they will generally be able to secure at least two meals each day (by 14 percentage points and 6 percentage points for the ultra-poor and other poor, respectively).
Finally, the use of sanitary toilets increases by 18pp and 11pp for the ultra-poor and other-poor respectively.
DISCUSSION AND CONCLUDING REMARKS
The results indicate that the duration of exclusive breastfeeding and vitamin A supplementation is increasing among both the ultra-poor and other poor. For adolescents and adults in ultra-poor households, several factors contribute to improved nutritional status. In addition to the income increase noted by Bandiera et al. 2013), we find evidence of improved food security, lower risk of illness and improved hygiene practices.
Although the income increase for this group is small (Bandiera et al. 2013), Angelucci et al. 2006), studying the spillover effects of a cash transfer program (PROGRESA) on the nutritional status of non-participants, offer an alternative explanation for the way this takes place. They argue that despite the nominal income increase among non-participants, consumption among these households increases significantly more. We find that the CFPR not only has a significant impact on the nutritional status of participants, but also creates positive spillover effects among non-participants.
The size of the impact on the non-participants in treated areas is typically half of the impact on the participants. The results may be indicative of the success of a large number of social awareness programs, including CFPR, working to reverse these trends (Kabeer et al. 2013). Finally, impact and spillover effects, particularly among infants (through increased duration of exclusive breastfeeding), are driven by behavioral change without financial incentives.
An evaluation of a large-scale program found that the program was able to promote earlier breastfeeding, but the duration of exclusive feeding remained unchanged (Saha KK, Bamezai A, Khaled A, Subandoro A, Rawat R 2008). Many studies, on the other hand, report no or even negative effects of food subsidy programs on nutrition (Jensen and Miller Shankar Shaw and Telidevara, 2014). Overall, despite taking into account the actual impact and spillover effects, the long-term impact of the CFPR may be underestimated, especially for children.
Bobonis GJ and Finan FS (2002) Transfers to the poor increase the education of the non-poor: the case of Mexico's PROGRESA program. Construction of the World Health Organization child growth standards: selection of methods for achieved growth curves. Poverty, Inequality and Spillovers in the Mexican Education, Health and Nutrition Program, FCND Discussion Paper No.
The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated using a multivariate model analysis. Dhaka and Ottawa: BRAC and Aga Khan Foundation Canada, (CFPR-TUP Working Paper Series No. 10). Dhaka and Ottawa: BRAC and Aga Khan Foundation Canada, (CFPR-TUP Working Paper Series No. 12).
ANNEXURES
Normalized differences greater than 0.25 indicate statistically different means.¥ Analysis at the individual level.† Analysis at the household level. The dependent variable, attrition, equals 1 if the individual is not observed in 2011 and 0 otherwise. The models are analyzed using village-level fixed effects and the standard errors are clustered at the branch level.
The null hypothesis that covariates and attrition differ across treatment status was not rejected. Effects of CFPR diffusion on the nutritional status of non-poor households Marginal effects Standard errors Panel A: 0 to 5 years. For ages 0 to 19 years, the effect on continuous z-scores should be interpreted in terms of standard deviations from the WHO international reference group mean.
Effects on the continuous z-scores should be interpreted in terms of standard deviations from the median of the WHO international reference group. Bold indicates significant difference between the two age groups at the 10% level.