Salmonella
typhi and applicability
of Etest
Yoshimi Matsumoto*,
Akiko Ikemoto, Akiko
Wakabayashi, John
Pitt,
Takashi
Hirano, Hitoshi Nishio,
Shuichi
Tawara
Abstrak
Aktivy'as in viÛo berbagai antibiotika termasuk sefiksim terhadap 73 isolat k/lnis Salmonella typhi dari berbagai srtmber telah dievaluasi menggunakan ,netoda dilusi agar konvensional dan Etest. I
I dari
73 galur tersebt$ resisten. terlndap klorantfenikol 4tn kotri-ntoksasol (sulfametoksrtsollrimetoprim), dan l2 dari I8 galur ini juga resisten terhadap amoksisil.in karenct nemprocluksi p-Iaktctnnse. sefiksim menunjukkan aktivitas yang baik untuk ke 73 galur tersebut dengan nilai MICgo 0,25 ltghnl. sefiksim menwtjukkan. aktit,itas )tang sangaî baik untuk galur yang resisten terhatlap kloratnfen.ikol, ternnsuk gaht penghasil $-laktamase yang resisten terhaclap amok-sisilin. HaI ini menuniukkan stabilitas p-laktamasenl'a yang tinggi. Aktivitas antibakteri sefiksim ternr-qta seban4ing dengan sefrriakson, ofloksttsin, dan siprofloksasin, yang saat ini sering digunakan untuk mengobati clemam tifoicl. Nitai MIC yang cliclapat clari Etest berko-relasi baik dengan hasil metoda dilusi agar konvensional. Hal ini menrulukknn bahwa Etest adalah stnttr metod4 baru yang mudah dilakukan tlan berguna untuk penentuan MIC. Sebagai kesimpulan, sefiksim oral merupakan obat altentatif lang aman dan efektif untuk penatalaksanaan demam tifoid, bahkan untuk kasus-knrus S. typhi yang resisten terhadap berbagai jenis obat.Abstract
The in vitro antibacterial activity of various antibiotics incfucling cefrxime against 73 clinical isolates o/Salmonella typhi from a vetriety of sources was evaluated by conventional agar-dih.uion metlod and Eîest.
lB
strains of these 73 strains were chloratnphenicol and cotrimoxazole (sulfcuttelhoxazole-trimetlnprtm) resistant arulI2 of these I8
strains were ttlso resistant to anroxicillin due top-Lttc-tamase protluction. Cefixitne slnwed excellent activity against
all
73 strains with the MICgI value of 0.25 1tg/nil. ReJlecting its high b-lactamase stabilily, CeJixime also lnd excellent activity against chloramplrcnicol-resistant strains inchrclirtg p-lactamase-proclucing amoxicillin-resistant strctitls. Antibacterial ctctivity of ceftxime was comparable to ceftriaxone, ofloxacin, antl ciprofloxacin, which are cl.rrently often useclfor
llæ trealment of typhoid fever The MIC values obtainetl front the Etest correlatecl well with th.e results of cotr-ventional agar-diltttion ntetlncl, suggesting the usefulness of the Etest as a new easy MIC detenninarion methocl.In
conclttsion, oral cefixinre can provicle a safe and effective allernativefor
nnnagement of tylthokl fetter even in cases of ntulticlrug-resistant S. typhi.Suppl
I
-
l99BAntibacterial
activity
of"€efTxime against
INTRODUCTION
Typhoid
fever continlles to be one
of
the majorpublic
health problems
in
developing countries.
Chloram-phenicol
was used
asthe
first
choice drug
for typhoid
fever
until
recently. However, causative
organism
Salmonella typhi
is developing
resistanceto
conven-tional
antibiotics
chloramphenicol, cotrimoxazole
and ampicillin
in
many
countries.
Consequently,
treatment of
typhoid fever with conventional
agentscan frequently cause clinical
treatment
failures
or
bacterial relapses. Frequencies
of
thesestrains called
MDR (Multi
Drug
Resistance)
are repofted
to
be 78.4Vo(1990) in Indiar, 75Vo
(1995) inEgyptz,77Vo
(1995)
in
Pakistan3
and 86Vo(1995)
in
Vietnama.
Re-Dept of Infections Diseases,
M edicinal Biology Research Laboratories, Ftlisewa Phannaceutical Co., Ltd., Osaka, Japan.
Therapy 189
T-1
flecting
this changing trends
of antibiotic
susceptibil-ity
of S. typhi, variolrs new
agents
having strong in
vitro activity
have been
tried clinically for the
treat-ment
of MDR
S. ryphr.MATERIALS
AND METHODS
Bacterial Strains
Clinically
isolated Salmonella
typhi
slrains were
pro-vided by Dr.
S. Matsushitaof
theTokyo Metropolitan
ResearchLaboratory of Public Health (37
strains
iso-lated in Philippines
in
1992-1994),
Dr.
K. Itoh of
the
National Institute
of
Infectious
Diseases
Japan
(15strains isolated
in
Japanin
1995-1997),
Dr.
Niimi of
the Osaka
City
General
Hospital
(9 strains isolated
in
Japanin
1994-1997).
The other
12 strains \ryerefrom
190
Typhoid Fever and other SalmonelLosisAntibiotics
Cefixime, cefdinir, ofloxacin, ciprofloxacin,
and
ni-trocefin
were synthesized
in
our laboratories.
Amoxi-cillin,
sulfamethoxâzble
andtrimethoprim
were
labo-ratory
standard. Ceftriaxone
and
chloramphenicol
were
commercially available.
Sulfamethox azole and
trimethoprim
were
mixed in
the
ratio
of
5:1
to
use ascotrimoxazole.
Susceptibility testing
Antibacterial
activity
of
test antibiotics was
deter-mined
by
agardilution
method using
Mueller-Hinton
agar
(Difco).
Inoculum
size was
approximately
103c.f.u./spot.
Etest
(AB
BIODISK,
Sweden)
was alSoused
for determination
of
susceptibility
of
S.ry-phi
to cehxime.
Detection
of
B-lactamase
B-lactamase
activity
was revealed
by
spotting
cells
onfilter
paper
containing
500
mg/ml of
chromogenic
cephalosporin nitrocefin
in
50
mM
potassium
phos-phate
buffer pH
7.0.Analytical
isoelectric focusing
Exponentially
growing cells
of
test strains
in
Trypti-case-soy
broth
(BBL)
were
harvested, washed
once, and resuspendedin
1/20volume of
50mM
potassium
phosphate
buffer pH
7.0. Crude extracts prepared
by
ultrasonic disruption were appiied on
an
Ampholine
PAG plate
(pH 3.5
-
10:
LKB).
Electrofocusing
wascarried out using
LKB
Multiphor
apparatus.
Severalkinds
of
known
B-lactamases
were also focused
onthe
same
gel. The
enzyme
activities were visualized
on
the gel
with overlaying filter
papercontaining
500mg/ml of nitrocefin.
RESULTS
Susceptibility
of
S.
typhi to various
antibiotics
The susceptibility
of
73 clinically
isolated
S. typhi
strains
was
evaluated
with
the conventional
agar-di-lution
method
for cefixime, cefdinir,
ceftriaxone,
amoxicillin, ofloxacin, ciprofloxacin,
chlorampheni-col
andcotrimoxazole.(Tâbie
1 andFigure
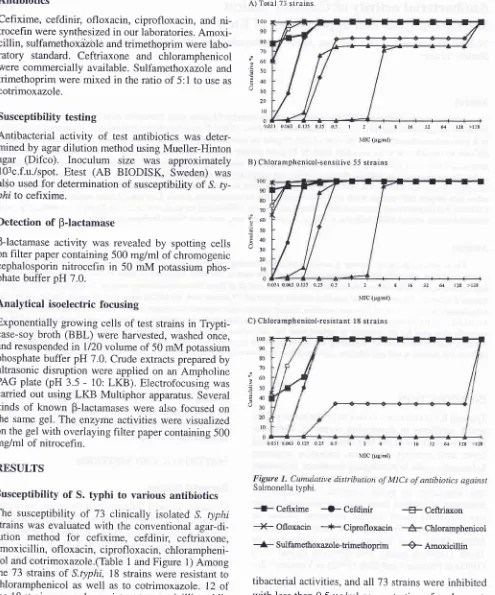
1)Among
the
73
strains
of
S.typhi,
18 strains were resistant to
chloramphenicol
as
well
as
to
cotrimoxazole. 12
of
the
18strains were
alsoresistant to
amoxicillin, while
the growth
of
the remaining
6
strains was inhibited
by amoxicillin
at
lessthan
0.5 pglml. The
other new
B-lactam and
quinolone antibiotics
showed good
an-A) Totâl 7:l strains
t00 90 80 70 60 50 40
l0
20
l0
0
,UlC (Ég/ml)
B) Chloramphenicol-sensitive 55 strains
0031 0,063 0t25 0.25 05 I 2 4
MIC (psiml)
C) Chloramphenicol-resistant I8 strains
0031 0063 0125 025 05 I 2 4 8 16 31 6 lzr >t:E Q
Med
J
Indonest 16 32 6t 128 >128 t00
m
8Cl
70
îuo
?so
?4 t3o 20
l0
0
100
90
80 70
=50Ê4 u30 20 l0 0
00it 063 0125 025 0._r I 2 4 I 16 32 64 t2E >t2E
\flC (Ég/ml)
Figure 1. Cumulative distribution of MtCs of antibiotics against Salmonella typhi.
*
Cefixime
{-
Cefdinir{F
Ceffriaxon--X-
Ofloxacin
--{-
Ciprofloxacin
-#
Chlorarnphenicotr*-
Sulfarnethoxazole-trimethoprimêAmoxicillin
[image:2.595.52.547.90.685.2]Suppl 1 - 1998
Ihble
L.
Antibacterial activity of cefixime against Salmonella typhiTherapy 191
SalmoneLla typhi (No. of strains)
Antibiotic MIC distribution (pgiml)
!.ffi
O.ffi 0.160.5 0.5
1 2 4 8
16 32
M
128 >1nMIC range
MICso
MICgoTotal (73) Cefixime Cefdinir Ceftriaxone
Amoxicillin
Ofloxacin Ciprofloxacin Chloramphenicol
Cotrimoxzole
91
1232281
1
[.0.031
0.250.125
0.258.0:031
0.0630.5
>1288.0.031
0.063!.0.031
t.0.0314
>1280.25
>12842
20
41236
57
44
11503
1 5
42
61
[.0.031-0.5
0.063-0.25 !.0.031 -0.125
12
0.25->128 !.0.031 "0.1 25r.0.031-0.25 1 g 1'>128
18
0.063->12844281
72
Chloramphenicol
- sensitive (55)
Cefixime Cefdinir Ceftriaxone Amoxicillin Ofloxacin Ciprofloxacin Chloramphenicol
Cotrimoxzole
50
4'l
2
21
20
32-
313
129251
36
18
154
111503
1 5
42
61
[.0.031-0.5 !.0.031
r.0.0310.063-0.25
0.125
0.125 0.0.031-0.125
!.0.031
0.0630.25-1 0.25
0.5 !.0.031-0.125
!.0.031
0.063r.0.031-0.25 r.0.031
!.0.0311-8
4
40.063-1
0.25
0.5Chloramphenicol - resistant (18)
CeTixime
Cefdinir Ceftriaxone Amoxicillin
0floxacin
Ciprofloxacin Chloramphenicol Cotrimoxazole
227
99
10
5!.0.031"0.25
0.063
0.250.125-0.25
0.125
0.25[.0.031-0.125
0.063
0.12512
0.25->128
>128
>128[.0.031"0.063
0.063
0.063[.0.031
D.0r031 u.0.0311g >128
>128
>12818 >128
>128
>128 .t .18
10 18Relation
between
BJactamase
production
and
susceptibility
to
cefixime
Amoxicillin-resistant strains
were
all
B-lactamase-positive by
easy
spotting
test.
However,
susceptibili-ties
of these
12
strains
to
cefixime, cefdinir
andceftriaxone
were
not different
from
other strains
(Ta-ble 2).
B-lactamasesproduced
by
thesestrains
hadpI
5.4
which
was
the same
as
TEM-I
type,
the
most
common
plasmid-mediated B-lactamase
in
gram-negative bacteria
world-wide.
Correlation
between
MICs from
conventional
agar-dilution method
and Etest
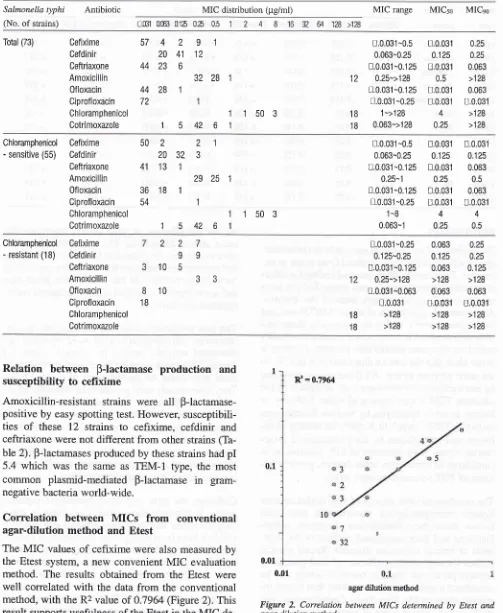
The
MIC
values
of
cefixime were
also
measuredby
the Etest
system,
a new convenient
MIC
evaluation
method.
The
results obtained
from
the Etest
were
well
correlated
with
the
data from
the conventional
method,
with
the
R2value
of
0.7964
(Figure
2).
This
result
supports usefulness
of
the Etest
in
theMIC
de-termination
of
S.typhi
to cefixime.
[image:3.595.43.546.104.717.2]agar dilution method
Figure
2.
Correlation between MICs determined by Etest and agar dilution method.xi
= 0.7964192
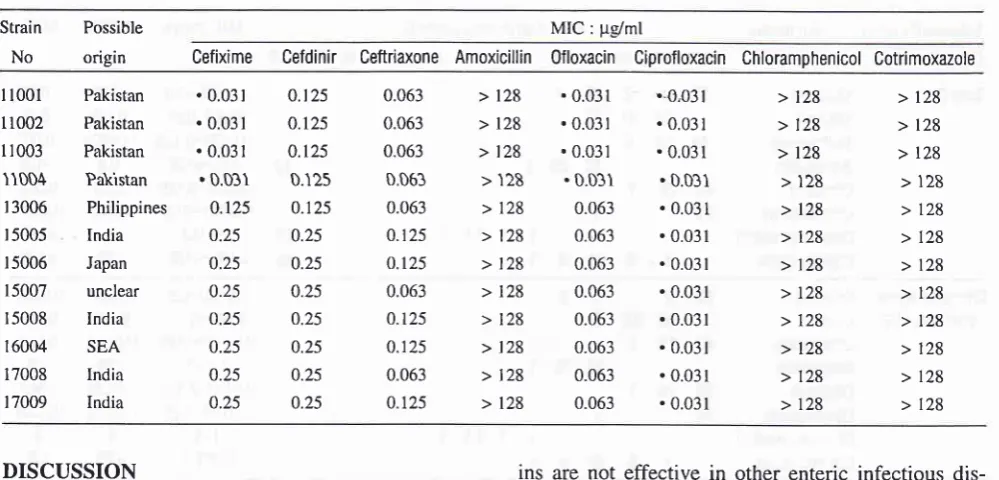
Tjphoid Fever and other SalmonellosisTable
2
List of p-lactamase producing Sahnonella rypâl strainsMed
J Indones
Strain
No
Possible
origin
MIC:
pg/mlCefixime Cefdinir
CeftriaxoneAmoxicillin 0floxacin
Ciprofloxacin Chloramphenicol CotrimoxazoleI
t00l
11002
r r003
ITDD4
r 3006
r 5005
r 5006
15007
r 5008
I 6004
17008 17009 Pakistan Pakistan Pakistan Pakistan Philippines India Japan unclear India SEA India India
.
0.03 r.
0.031.
0.03 r. 0.031
0.125 0.25 0.25 0.25 0.25 0.25 0.25 0.25 0.t25 0.125 0.t25 0.125 0.125 0.25 0.25 0.25 0.25 0.25 0.25 0.25 0.063 0.063 0.063 0.063 0.063 0.r25 0.125 0.063 0.t25 0.125 0.063 0.t25
> 128
> l2g > 128
>'t2g
>
l2g>
128>
t2g>
128> t28
>
l2g> I28
>
128. 0.031
. 0.03r .0.031 .0.031 0.063 0.063 0.063 0.063 0.063 0.063 0.063 0.063 ..0,031
.
0.031.
0.031.0.031
.
0.031.
0.031.
0.031.
0.031.0.03r
.
0.03 t.
0.031.0.031
>
128>
128>
t2g > 128>
128>
129>
128>
128>
129>
128>
128>
128>
l2g>
l2g>
128>
l2g>
128>
128>
128>
129>
128>
129>
128>
128DISCUSSION
The
problem of
resistance is
inevitable in
chemother-apy
of infectious
diseases.Typhoid
fever is not
anex-ception. Transferable
MDR plasmid
coding
for
chlor-amphenicol, cotrimoxazole,
and
ampicillin
has
beenspread
over S.
typh.i
in
many
areas
of
the
worldt-4.
Approximately one-fourth of
strains
(18/73)
we
usedin this study
were
found to
beresistant
to
thesecon-ventional
agents.These
resistance genes areprobably
coded
on the
same
transferable plasmid, although
it
is not
clear that
the amoxicillin
resistance
geneis
onthe
sameplasmid or not. All
B-lactamases prodlrced
by amoxicillin
resistant strains were thought to
be thecommon
TEM-1
type
from
a pI value.
Cefixime
isknown
to
resist hydrolysis
by
various
p-lactamasesincluding
TEM-1
types.
In S. typhi,
the
activity of
ce-fixime
was
not affected by the production
of
BJac-tamase either. Some
variation
of MIC
distribution is
considered
to
come
from
other factors, possibly
be-cause
of
PBP
variations
in
each strain.
The
excellent
in vitro activity of new
cephalosporins
against enteropathogenic
bacteria has been
well
known
since
their introduction. However,
cepha-losporins had
been
considered ineffective
for
treat-ment
of enteric infectious
diseases.
Recent clinical
studies showed
excellent efficacy
of third
generation
cephalosporins
for typhoid
fsys12,6-8which
can
beconsidered
asystemic
infection
rather than
a localin-testinal
infection
like
Shigellosis. Cephalosporins
canwork
against
certain types
of
enteric infectious
dis-eases such as typhoid
fever. Conversely,
cephalospor-ins are not effective in other enteric
infectious
dis-eases
such
asShigellosis. The
reason
for this
differ-ence
in activity
is presumed to
be dueto
the
infection
mechanisms
peculiar to
eachbacterial
species such asbacterial
distribution
in
the
body,
toxin
production
and so on.Further microbiological
andclinical
inves-tigations
arerequired.
The new antibiotics, cefixime, cefdinir, ceftriaxone,
ofloxacin, and ciprofloxacin, showed excellent
an-tibacterial activities against
the clinical
isolates
of
S.typhi.
This result
supports the
clinical
usefulness
of
these
new
agents
for
the treatment
of
typhoid
fever.
They have already
beenproven
to
beclinically
effec-tive2-4,6'12.
However,
new
quinolone
antibiotics
should not be
administered
to
pediatric patients
dueto possible
adversedrug
reactions.
p-lactam
antibiot-ics
can besafely
usedfor pediatric
patients, although
parenteral
onesare more
costly
in
terms
of
requiring
hospitalization,
anddrug
acquisition,
as well asbeing
less
convenient than
oral administration.
Cefixime, the
first
oral
third generation
cephalo-sporin,
is
currently commercially available
in
about
sixty
countries, and
its clinical efficacy
and safety
in
children
have
beenwell proven by
numerous
clinical
trials
and
large-scale
post marketing
surveillance13.Cefixime
can also
beadministered
in
aonce
or twice
daily
dosing regimen,
which can
enhance
patient
compliance,
especially
in
children
who
sometimes
refuse
oral administration.
Several
clinical trials
have [image:4.595.49.549.101.341.2]Suppl
I
-
1998It
is
recommended
that quinolones or
3rdgeneration
cephalosporins
should
be used
to
treat
suspectedty-phoid
fever
in
areaswhere
MDR
S.typhi
isprevalent,
until
culture
and
sensitivity
results
areavailable.
Ce-fixime provides
a safe,effective
and cheaperoral
op-tion
for
thetreatment
of typhoid fever in children,
es-pecially in
endemic
MDR
areas.REFERENCES
1.
Sugandhi Rao, P Rajashekar,V
Varghese, GK Shivananda,PG. Emergence of multidrug-resistant Salmonel.la 4,phi
inrl-ral southern India. Am J Trop Med Hyg 1993;
48(l):
I08-11.2.
Girgis NI, SultanY
Hammad O, Farid Z. Comparison of theefticacy, sat'ety and cost of cefixime, ceftriaxone, and
aztreo-nam in the treatment of multidrug-resistant Salntonella typhi
septicemia in children. Pediatr Infect Dis J 1995; l4(7):
603-5.
3.
Mirza SH, Beeching NJ, Hart CA. The prevalence andclini-cal features
of
multi-drug resistant Salntonel.latypli
infec-tions in Bauchistan, Pakistan. Ann Trop Med Parasitol 1995;
89(5):515-9.
4.
Vinh H, Wain J, Hanh VTN, Nga CN, Chinh MT. Bethell D,Hoa NTT, Diep TS, Dung NM, White NJ. Two or three days
of ofloxacin treatment fbr uncompJicated Multidrug-resistant
typhoid fevel in children. Antimicrobial Agent and
Chemo-therapy 1996; 4O: 958-61.
5.
Shigi
Y,
MatsumotoI
KaizuM,
FujishitaY, Kojo
H.Mechanism of action of the new orally active cephalosporin
Therap,- 193
FK027. The Journal of Antibiotics 1984;3'/(7): '190-6.
Cirgis
NI,
Kilpatrick ME, FaridZ,
Sultan Y, Podgore JK.Cefixime
in
treatmentof
enteric feverin
children. DrugsExptl Clin Res 1993; 19(l): 47-9.
Bhutta ZA, Khan JA, Molla AM. Therapy of
multidrug-resis-tant typhoid fever with oral cefixime vs intravenous
ceftriax-one. Pediatr Int'ect Dis J 1994; I3(11): 990-4.
Girgis NI, Tribble DR, Sultan
I
Farid Z. Short cou.rseche-motherapy with cefixime in children with multidrug-resistant
S a lrno ne I la ty p hi. Seplicaemi a. Journ al of Tropical Pedi atri cs
1995;41:364-5.
Alsoub H, Uwayadah AK, Mater l,Zebeib M, Elhag KM. A
clinical comparison
of
typhoid fever caused by susceptibleand multidrug-resistant strains of Salnonel.la typhi. Br J Clin
Pract 1997 ; 5l
(l):
8-l 0.Alam MN, Haq SA, Das KK, Baral PK, Mazid MN, Siddique
RU. Efficacy of ciprofioxacin in enteric fever: comparison of
treâtment duration
in
sensitive and multidrug-resistantSal-monelLa, Am J Trop med Hyg 1995; 53(3): 306-l1.
Wistrom J, Norrby SR. Fluoroquinolones and bacterial
en-teritis, when and tbr whom? J Antimicrob Chemother 1995;
36(1):23-39.
Seceer G, Kanra G, Figen G, Akan S, Ceyhan
M,EcevitZ,
Ofloxacin versus co-trimoxazole in the treatment of typhoid
fever
in
children. Acta Paediatrica Japonica 1997;39:218-21.
Nishio, H. An International Review of the Safety Profile of
Cefixime Curr Ther Res 19941 55 SuppA: 63-7.
l0
ll
12