168
Hendarto and Gray MedI
IndonesSurgical and non-surgical intervention
for speech
rehabilitation
in
Parkinson
disease
Heru Hendarto*,
StevenGray'
Abstract
Parkinson disease is a common progressive neurological disorder with an unluown etiology.
It
hns a high incidence of speech, voice and laryngeal abnormalities which vary due to the severity of the disease. In addirtonb
temor and supraglottic hyperfinction, bowedvocal folds may result as part of the aging process. This condirton
will
cause an inadequate vocalfold
adduction or hypoadduction.The approaches
for
speech rehabilitation in Parkinson disease are speech therapy or vocal fold augmentation. One of the most studied approaches is thelze
Silvennan voice treatrnentfor
Parkinson disease. This program encourages maxirnum phonntory effort and improves voice quality, Vocal fold augmmtation by injecting under direct visualcontol
is one way to restore the focal fold function, The ultimate goal in the restoration of glottic insufficicncy is to mimic nature as closely as possible. Although many clinical stuliesshow promising results
for
the use of collagen injectionfor
bowed vocal foW ffeatment, no stady had shawn the efficacy of injectedvocal fold compared to voice teannent or the
fficacy
of combining both procedures.Abstrak
Penyakit Parkinson merupakan kelainan saraf yang progresif dan tidak diketahui penyebabnya. Kelainan
ini
mempunyai variasi kelainan wicara, suara, dan laring sangat tinggi yang sesuai beratnya penyakit. Keadaanini
seing dapat mempengaruhi produksi suara. Di samping tremor dan hiperfungsi supra-glotik, melengkungnya lipatan pita suara dapat terjadi larena proses penuaan. Halini
yang menyebabkan tidak sempurnanya adduksi atau hiperaddulcsi. Rehabilitasi suara pada penyakit Parkinson adalah terapi wicara atau augmentasi plika voknlis. Salah satu penelitian yang banyak dilakulan adalah terapi wicara cara Lee Silverman yangmemfokuskan kepada fonasi pada pengobatan kelainan suara pada penyakit Parkinson. Program ini mendapatlcan hasil maksimal dan memperbaiki kualitas suara. Swrtilan untuk menghasillan augmentasi pita suara adalah salah satu cara wûuk memperbaiki fungsi pita suara. Tujuqn utamanya adalah memperbaiki insufisiensi glotik dengan mendekati gLotik ke
fingsi
pita suara senormal mungkin.Walaupun banyak penelitian penyuntikan kolagen memberilcan hnsil yang menggembirakan, belum ada suatu penyelidil<an yang membandingkan hasil suntiknn pita suara tersebut dengan terapi suara atau kombinasi kedua cara.
Keywords: Parkinson disease, Lee Silverman, collagen injection, hypophonia
This condition
wasfirst
describedby
James Parkinsonin
1817, althoughits
symptoms andpotential
therapieswere
mentioned
in
the
Ayurveda,
the
system
of
medicine practicedin
krdia
asearly
as 5000BC,
andin
the first
Chinese
medical
text,
Nei
Jing,
which
appeared 2500 yearsago.'
The
etiology is still
unknown
or idiopathic, but
some researchershave mentioned
the
possibility
of
post
head trauma, post-encephalitis
or
prolonged use of
certain drugs. There are
degenerative changesin
theextra-pyramidal
system
especially
at the
substansianigra
and afew
cellsin
thestriatum.t*
This
will
cause adopamine deficiency,
andis
considered
responsiblefor
theprimary
disease symptoms.3'aPatients
aremost
often
aware
of.tremor, slowness
of
movement, andgait impairment.
In
most patientswith
Parkinson (also
known as
paralysis agitans),
is
acommon
progressiveneurological
disorderthat
resultsfrom
degenerationof
nervecells
(neurons)in
a regionof
the brain thatcontrols
movement.It
has anunknown
etiology due
to
deficiency
of
dopamine
(important
chemical transmitter
in
certain brain cells
goveming
movement, balance andwalking).
Parkinson disease isa
growing national problem,
with over
a
million
victims
in
the
United
States alone.There
are20
new casesof
Parkinson'sper
100,000 people per year.Most
victims
areover 40
yearsold
althoughthe
disease canappeff in
younger patients.l'z' Department of Communication Disorders, University
of
Utah at Salt Lake City, Saltlnke
City, Utaht
Vol 9, No 3, JuIy
-
September 2000early
stage, the diseaseis predominantly unilateral,
sothat
the
degree
of
functional
impairment
often
dependson which
handis
affected.Diagnosis
is basedon a
neurological examination
which
coversevaluation
of the
symptoms and
their
severity.
If
symptoms are serious enough,
a
trial
test
of
anti-Parkinson
drugs
may be
indicated.
Also
whenindicated,
brain
scansmay be
madeto rule out
other
diseaseswith similar
symptoms.l'3'aThe
earliest symptoms
of
Parkinson
diseasemay
benonspecific
and include
weakness, tiredness,
andfatigue. Other characteristic symptoms
for
diagnosingpurposes
can
be
divided
into
primary
symptoms:rigidity
(increased
tone in
the
muscles),
tremor
(smooth shakingof
thelimb
or
other partof
the body),difficulty with
balance, anddifficulty in walking
(due torigidity, tremor
&
balance incoordination). Secondary symptomswhich
may be presentsinclude:
depression,sleep
disturbances,
dementia
(senility),
speechproblems
the voice may
sound (breathy,
tremulous,high-pitched,
hoarse,
or
strident),
blepharospasm
(isthe inability
to
open
the
eyelids-or once
opened),bradykinesia
(slowness
and proverty
of
movement),difficulty
in
swallowing
(dysphagia),
drooling
(si alonhea), constipation, breathing problems,difficulty
voiding,
dizziness, stooped posture,
swelling
of
the feet. and sexual problems.-t'oThere
is no
cure
for
Parkinson
disease
but
somemedication such
aslepo
dova
(L-Dopa)
canbe given
to
minimize the
symptoms.
L-Dopa helps
replenish someof
the
lost
dopamine and when combined
with
other
drugs, helps
to
stimulate
the
dopamine
systemor
mimic
its
controlling effect
on other
nerve
cells,such
as
bromocriptine, pergolide, selegilene
and trihexyph em idy e.t'2'aSpeech therapy and collagen augmentationfor parkinsonian hypohonia
r69
Operative
procedures such astransplantation
of
tissueinto the
area
of
the
basal ganglia
that
acceptsdopamine
from
the brain-stem
is
another
treatmentpossibility.
This
area
is
called
the
striatum and
isdivided
into
the
caudate
nucleus and
the
putamen.Dopamine-producing
tissue has been transplantedinto
areasof
thestriatum
with
increasing
success.In 1950,
an ablative surgical
procedure
was
first
performed.Most
therapies
including tissue
trans-plantation
are aimed at increasing theproduction
and/or transmissionof
dopamine.This new
procedureis
doneby
placing
asmall leison (hole)
in
the circuit. The circuit
can
beintemrpted safely
in
human
in
the
globus
pallidus
(pallidotomy)
or
the
thalamus
(thalamotomy).
Thalamotomy
can
alleviate
tremor in
the
body
oppositeto
the
sideof
thebrain
that
is
operated uponwith up
to
98Voeffectiveness.
Problems
associatedwith
thalamotomy
include
loss
of
muscle
tone,balance
impairment, and
speech
impairment.
Theseoccur
with
greater frequency
in
patients
getting
bilateral (both
sidesof
thebrain)
surgery.Pallidotomy
helpsbradykinesia
(slownessof
movement)
more thantremor. Balance
and
speech
are
usually
improved
even
after only
one surgery
(unilateral pallidotomy).
Both
thalamotomy
and
pallidotomy reduce
theinvoluntary
movements
that occur
(dyskinesias) as
a sideeffect of anti-Parkinson
disease medicines.5PHYSICAL FINDINGS
One
of
the
characteristics
of
Parkinson
diseasefrom
the
laryngeal examination
in
addition
to
tremor
andsupra
glottic
hyperfunction,
are bowed vocal
folds
(see
figure l).6'r'tt
Bowed vocal
folds
are literally
folds
that
look
like two
bows
joined
at the
front
and170
Hendarto and Graypart
of
the vocal folds, and overtime, may results
in
a lossof
musclebulk in
the vocal folds that causes moredifficulty for
vocal
fold
closure.s'eBowing
at any age comesfrom
a subtlelack
of "nerve"
input to the vocal
folds. Typical
symptoms
are weak voice and
vocal
8.11.t2rangue.
This
condition which
IS theresult
of
Med J Indones
Vocal produetion
of
patient
with
Parkinson
diseaseare
characterized
by
low
vocal intensity,
monotone and hoarseness.t'ttThis
condition
may contribute
to
areduction
in
speech
intelligibility,tultt and
reducedvocal folds adduction
due
to
bowed vocal
fold.7'r2The
perceptual features
of
hypokinetic
dysarthtia
(including
reducedin ability to
sustain phonation and loudness)indicate
for
an impaired respiratoryfunction
(See
Table
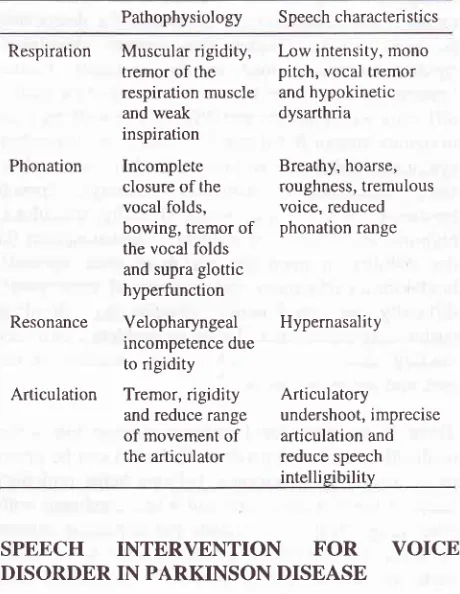
l).tt'tt
Table
l.
Speech characteristics of Parkinson diseaselhls
condltlon whtch rs the most colnmon result
orsenescence,
can
be
diagnosed
by
using
a
video-stroboscopy method.l3'la
Laryngolosits
suspectempirically
that this
condition
is due to the atrophy
of
the thyroarytenoid
muscles.
They
also indicated
thatthere
is
contribution
of
cricothyroid
muscleatrophy.s'r1
Physiological
changes
in
bowed
vocalfold
may
developed
from
muscular
weaknessdue to
lack
of
nerve innervation,
paralysis,
thinning
of
the connective tissue and disorganization of themyofibril.
This
may befurther
compoundedby
a decreasein
the tissueof
the superficial
and intermediate
layer of
thelamina propria.8'll'13
This condition
also can be relatedto
the extent
of
removal
of
the vocal
fold
tissue
in
laser surgery.
Bowing
of the
vocal
fold
as partof
the aging process appears as one of the two mostcommon
causes
for
hoarseness,
along
with
vocal
fold
paralysis.T'10'tt'tt
B"cause
of
this condition, the
vocal
fold
may
adduct
posteriorly
but not medially
which
will
cause
and
inadequate
vocal
fold
adduction
or
hypoadduction.to'tt
CHANGES
IN
VOICE PRODUCTION
There
is a
high
incidence
of
speech,
voice
andlaryngeal abnormality which varies due to the level
of
the disease
itself.
The
individuals
may have problems
with
phonation
(hoarseness,roughness,
breathiness,and tremulousness
due
to
laryngeal
dysfunction),
articulation
(articulatory undershoot,
rigidity
and reduce rangeof
movement),
resonance (co-occurrenceof
hypernasality;, and tongue
movement
(tremor of
the tongue).6'7Voice
disorders
common
in
Parkinson
disease
inwhich
many are
associated
with pitch,
loudness or
changes in
voice quality
in
which the bowed
vocalfold
may be the main culprit
for
this
condition.r0'rsThis condition which
also the most
common result
of
senescence
which
appear astwo of
the most commoncauses
for
hoarseness
along with vocal
fold
paralysis.T't
l't2
Direct
observation
of
the
larynx
indicated that there
is
a
direct relationship
between breathinessad reduced loudness
with
the gap
createdby the
bowed vocal folds.T'8'rl
Pathophysiology
SpeechcharacteristicsRespiration Muscular rigidity, tremor of the respiration muscle and weak inspiration
Phonation
Incompleteclosure of the vocal folds, bowing, tremor of the vocal folds and supra glottic hyperfunction
Resonance
Velopharyngeal incompetence due to rigidityArticulation
Tremor,rigidity and reduce range of movement of the articulatorLow intensity, mono pitch, vocal tremor and hypokinetic dysarthria
Breathy, hoarse, roughness, tremulous voice, reduced phonation range
Hypernasality
Articulatory
undershoot, imprecise articulation and
reduce speech intellieibilitv
SPEECH
INTERVENTION
FOR
VOICE
DISORDER
IN PARKINSON DISEASE
There
is a
long
history
of
research
attempting
todocument the effectiveness
of
speechintervention
in
Parkinson
disease.
Basically there
are
two
major
focuses
of
the
treatment.
The
first
one
is
a
broadbased speech improvement
program
designes
toimprove voice
loudness,
intonation and
articulation.
The
second one focusesonly on
single
aspectof
thevoice production such as improving
the
voice
andrespiration
such as the Lee Silverman voice treatmentfor
Parkinson disease (Ramig,
et all,
1995).re'20Although
the
ideal
candidate
for
intervention
is
apatient
with
idiopathic
Parkinson disease
andhypoadduction,
this
program
focuses
on
phonation,
and perhaps hasthe most encouraging results
for
the [image:3.595.345.575.229.526.2]Vol 9, No 3, July
-
September 2000effort
in
order
to
bring vocal folds
together
andimprove voice quality. This program
is
driven
by
anumber
of
perceptual
,features
of
phonation
in
Parkinson disease
such
as
reduced
in
pitch
and Ioudness, breathiness, and hoarseness.20'21The main goal
of
thel-ee Silverman
Voice
Treatmentfor
Parkinson disease
is to
increase
vocal
fold
adduction as
well
as respiratory volume.lT''o
This
isthe most studied treatment and the one
with
the
bestresults so
far
andis
doneby
encouraging the patient to"Think Loud!"
Increased
phonatory
effort
isaccomplished
in
a
seriesof
gradedtherapy
tasks thatfocus
on
increasing loudness, increasing intonation,
and reducing
hoarse
voice quality. Patient
receivesfour
treatment
sessions
per
week
for
four
weeks.Outcome
measuresincluded
a
comprehensive
rangeof
aerodynamic, acoustic,
and
perceptual
measures.Sessions
typically include both practice
on
simplephonatory
tasks (such as sustainingphonation
aslong
as possible)
and practice
in
maintaining
phonatoryeffort
in
speech activities, beginning
with
shortphrases
and progressing
to
longer
utterances.
Theclinician role
is to
give
patients
objective
feedbackabout
their
performance;
for
example,
length
of
maximum phonation or fundamental frequency
range.The
clinician
strongly
encourages
maximum
per-formance throughout
the
sessionand provides
homepractice
drills
to
elicit
maximal
levels
of
per-.
20.21IOrmance.
Ramig
et
a1,20 suggest that there are a numberof
keysto
the successof
thistype
of
treatment:1.
Simplicity
The
therapy
is
simple,
focusing
only on
thephonatory
aspectsof
speechproduction.
Becausepeople
with
Parkinson
disease areknown to
havedifficulty
simultaneously executing
two
move-ments,
simplifying
the focus
andinstructions
mayincrease the
probability
of
successful learning.2.
FocusFocus also
on
non-phonatory
aspects
of
speechproduction.
Speaking rates
may
be
slowed,
oral articulatory. gesturesmay
be extended, andoverall
speechintelligibility
may be
improved.
This
maybe related to an overall increase in physiologic effort.
3.
Intensive
treatmentThe intensive
treatmentwith
immediate
transferof
skills to
speechis
highly motivating.
Speakers andtheir
spousesreport immediate improvements,
thusencouraging
them
to
work
even
harder
to
bring
about more changes.Speech therapy and collagen augmentation for parkinsonian hypohonia
t71
4.
Calibration
Individuals with
Parkinson
disease appearto
havedifficulty
gauging
what is an
appropriate
level
of
phonatory
effort.
Patient testimonies
suggest thattheir
perceived
level
of
effort
must
be
"re-calibrated
to
insure
successful
carryover".
Speakersoften report that they do not realize their
voices aresoft
or
weakprior
to
treatment.Early in
treatment,
many
reported
feeling
as
if
they
wereshouting
in
order
to
produce
"normal"
voicing.
With
continuous feedback and other
techniquessuch as
review
of
audiotape recordings,
speakersare taught
to
become
comfortable
with
the
new
loudness
level.
Therefore,
a
focus
on
self-awarenessand
accuratecalibration
of
the
amountof effort
neededto
produce
acceptablevoice
also appear to becritical
treatment features.SURGICAL INTERVENTION
FOR
VOICE
DISORDER
IN PARKINSON DISEASE
Recent
advances
in
phonosurgery
have resulted in
several
new
approachesto
the managementof
bowed
vocal
folds. The ultimate goal
in
the restoration
of
bowed vocal folds
is to
mimic nature as closely
aspossible. Focal
fold
augmentation
by injection
underdirect visual control
is
possible
to
restore
the
focal
fold
augmentation
by
injection under direct
visual
control
is possible to
restore thefocal fold
function.22 Remacleet
al
(1990), Bless
et al
(1992),
andFord
etal
(1995)
usevocal
fold
injections
in
their
treatmentof
glottic
insufficiency. These
are
a
broad
studieswhich
include bowed vocal
folds
among the
subjectsand
show
a
promising result
for
the
injection
of
collagen
in
bowed vocal
folds.20'23'24The
studies also suggest thatin
patientswith relatively minimal glottic
insufficiency
who
are
bothered
by
weak,
breathy voice production, collageninjection
may be arelatively
safe and successful method
of
treatment.Many
patientswith
prebylaryngis,
with
bilateral
paresis
from
neurologic
diseaseor
trauma, andwith bowing
due tocricothyroid
muscle weaknessfit
in
this
g.oup.t'
In
anarticle
by
Burke,
etal
(1999), collagen injection
was
usedin their
study
of
35
Parkinson
patient with
hypophonia.
This
was
a
non
controlled study of
subjective
satisfactionwith
the procedures as reportedby
each patient.
This
suggestthat
the
augmentationmay
have arole
in
the
managementof
hypophonia
in
Parkinson disease
although
further
research
is172
Hendarto and GrayOne
of
the
issue
on injecting foreign materials.is
viscocity
andelasticity of
the vocal
tissuesis affected
by
theintroduction of
theforeign
biomaterial
becausethe
phonation threshold pressure
for
vocal fold
oscillation
is directly related
to
the viscosity
of the
vocal
fold
mucosa.
A
material
with
a
low
viscosity
flows
easily,
with little
internal
energy
being
dissipated
in the
shearing
process.A
highly
viscousmaterial
flows
more
slowly and dissipates
more -energyin
the
process.
At the
microscopic
level,
this
resistance depends
on
the
ease
of
relative
shear or
slippage between molecules
of
the material,
which
isdetermined
by
different
kinds of intramolecular
andintermolecular interactions
such
as
physical
entanglement, electrostatic
forces (e.g.,
hydrogenbond),
hydrophilic
and hydrophobic interactions,
andchemical interactions.
The stronger
the
molecular
interactions,
the more
resistant
the
molecules are to
slippage, and the
higher
the viscosity.22Numerous materials
have been used over the yearsfor
vocal
fold
augmentation. Synthetic polymer
Teflon
ismuch more
viscous
than
the
other
(biologic)
materials. Denatured
or partially
hydrolyzed collagen
and gelatin have
a
higher dynamic viscosity
thancollagen. The chemically cross-linked collagen
showsa
higher
dynamic
viscosity
than noncrosslinked
collagen, as
expected
from
the formation
of
many
covalent crosslinks
in
tropocollagen. Fat has
a lower
dynamic
viscocity
thancollagen, probably
becauseof
its very
different
molecular
composition.22The collagen implant consists
of
bovine
collagen
modified
by solubilization
andcross-linking to
reducecellular
and humoral host immune
response,but
it is
histologically
similar
to
the
deep lamina
propria
tissues
in the vocal
fold.
The
procedure requires
noextemal incisions
on theneck. Most important,
results appearto be long-lasting, which
hasbeen confirmed
objectively
and
subjectively.22'23Injected
collagen
closely
resembles host tissues at thevocal
fold
lamina
propria.
Like
other bioimplants,
it
promotes ingrowth
of
host tissues and eventual replacement
of
injectatewith
hostcollagen.
One
of
the unique
properties
of injected
collagen
isthe
apparent
tissue softening that occurs when
thecollagen is placed
in
scar tissue.The
eventsfollowing
collagen
injection
that
affect vocal
fold
function
specifically include
the gradual variable resorption
of
injected collagen, the
replacement
of
some
resorbedimplant
by
deposition
of
new
host collagen from
metabolically active invading
hostfibroblasts,
and theMed J Indones
softening
of
due
to
fibroblastic
Small
arnounts
(0.0
din
theplane
of
thevocal ligament
andthe intermediate layer
of
the lamina plgpria were
successful
at
producing
improved
voices."
Although bovine
collagen
is
widely
available,
autologous collagen
will
most
likely
have
evengreater
persistence
than bovine
collagen;
becauseautologus collagen molecules are preserved
in the
preparation process.2''According
to
Remacle
et
a1,23 collagen does have some disadvantages. 1)Its is not
cross-linked,
andits
sensitivity
to
fibroblast-secreted collagenase
could
lead
to
long-term resorption.
2)
The microfibrils
consolidate
in
situ after the injection.
3)
Water
-
avolume equivalent
of
at
least
60Vo
of
the
injected
volume
of
collagen
is eliminated,
requiring
overinjection.
Three percentto
4Voof
patientsinjected
with
collagen
are hypersensitiveto
it.
Resorption
is
reduced when collagen
is
injected
into
more superficial
vocal fold levels (superficial
lamina
propria)
and,in
many patients, asuperficially
injected
implant
could be
seeneasily
through the
transparentmucosa
years after injection.
Most
of
the
patientsreceives
immediate
relief
after injection, and
if
theimplants
is
properly placed
in
the
lamina
propria,
gradual resorption and
replacement
allow
the
vocal
mechanism
to
compensate
incrementally
for
small
changes.23
CONCLUSIONS
Parkinson
diseaseis
a
common
neurological
diseasewhich affects a large number
of elderly adults,
andoccasionally develops
in
young adults as
well.
Thedisease
is
caused
by
dopamine deficiency
which
effect many
movements
including walking
andhandwriting that
become
very small and weak
overtime.
For
most patients, voice and
speech
become weak and slurred aswell.
One
of
the characteristics
of
Parkinson
diseasefrom
the
laryngeal examination,
in addition
to
tremor
and supraglottic
hyperfunction is bowed vocal
fold
which
results
in
opening
of
the middle
part
of
the
vocal
Vol 9, No 3, July
-
September 2000indication
that
bowing might
be
the
result
of
senescence.
Voice disorders are common
in
Parkinson
disease.They
are associatedwith
pitch,
loudness or changesin
voice
quality.
The voice is characterizedby
low
vocal
intensity, monotone
and
hoarseness
which
maycontribute
to
a
reduction
in
speech
intelligibility,
reduced
in
ability
to
sustain phonation and
loudness dueto
animpaired respiratory function.
The most effective
treatments
for
speechand
voice
problems
associatedwith
Parkinson
disease appear tobe intensive
onesthat
involve daily
therapy
or
nearly
daily
therapy
for a
few
weeks.
The most
studiedtreatment and
the
one
with the
best results so
far
iscalled Iæe Silverman Voice
Treatment
which
focusonly
on single
aspectof
the voice production
such asimproving
the voice
andrespiration.
This
method hasthe most encouraging results
for
the treatment of
speech
disorders related to Parkinson
disease becauseit encourages
maximum
phonatory
effort
in
oder
tobring vocal
fold
together andimprove voice quality.
Recent
advances
in
phonosurgery
have resulted in
several
new
approachesto
the
managementof glottic
insufficiency. The ultimate goal in the
restoration
of
glottic insufficiency
is to mimic
nature
asclosely
aspossible.
Vocal
fold
augmentation
by
injecting
collagen under
direct visual control
is
one way
to restore thevocal
fold
function. Injected collagen is
anactive
bioimplant that closely
resembleshost
tissuesat
the vocal
fold
lamina propria. Although
manyclinical
studies show promising results
for
the
useof
collagen
injection for
bowed vocal
fold
treatment, nostudy
had
shown
the efficacy
of
injected vocal fold
compared
to
voice
treatment
or
combining
both procedures.Finally,
it
is apparently useful to study
theefficacy of
voice
treatmentwith
collagen
injection
or
theefficacy
of
combining
both
procedures especially
for
thetreatment
of
voice
disorders
for
patients with
Parkinson
disease.Future
research
should focus
onexamining
short and
long
term
effects
of
both treatments.REFERENCES
l.
YorkstonKM,
Miller RM,
StrandEA.
Management ofspeech and swallowing in degenerative diseases. Tucson, AZ: Communication skill builder, 1995.
Speech therapy and collagen augmehtationfor parkinsonian
hypohonia
17311.
Nusbaum
RL,
BieseckerLG,
PavanWJ,
SchwartzbergPL,
SuchyS, Boris
AW.
Background information on Parkinson disease. In National Institute of Health Divisionof
Intramural ResearchReport
[On
-
line],
1998.Available:
.hrml.
Berke GS, Genatt B, Kreiman J, Jackson K. Treatment of
Parkinson hypophonia
witb
percutaneous collagen augmentation. Ann Otol Rhinol Laryngol 1999;108:22'l-31.
Larsen
HR.
Parkinson disease:Is
Victory
in
sight? Intemational Joumalof
Alternative and complementary Medicine, 1997 ; 15: 22-4.Cosgrove
GR.
Surgery for
Parkinson
disease. InFunctional
and
stereotactic neurosurgery, HarvardMedical School [On-line], 1998.
Available:gMGH.
Netsel R. A neurobiologic view of speech production and the dysarthria's. San Diego, CA: College
Hill
Press, 1986. PerezKS,
RamigLO,
Smith
ME,
DromeyC.
The Parkinson larynx: termor and videostroboscopic hndings. Joumal of Voice 1996;l0:
354-61.Smith
ME,
RamigLO.
Neurological disorders and the voice. In Rubin JS, Staloff RT, Korovin GS, Gould WJ,Eds. Diagnosis and treatment
of
voice disorder. New York, NY: Igaku-
Shoin, 1995: 203-24.Ramig
LO,
Scherer RC. Speech therapyfor
neurologic disorder and the larynx. In Blitzer A, Brin MF, Sasaki CT,Fahn
S, Hanis
KS
(Eds.), Neurologic disorderof
the larynx. New York,NY:
Thieme Medical Publisher, Inc, 1992:163-82.Lundy DS, Silva
C,
CasianoRR, Xue JW.
Causeif
hoarsenessin
elderly patients. Otolaryngol-
Head Neck Surg, 1998; 1 18 : 481-85.Tanaka S, Hirano
M,
ChijiwaK.
Some aspectof
vocal folds bowing. Ann Otol Rhinol Laryngol 1994; 103:357-62.12.
Smith ME, Ramig LO, Dromey C, Perez KS, Samandari.Intensive voice
treatment
in
Parkinson
disease:Laryngostroboscopic findings. Joumal
of
Voice 1995; 9:453-9.
13.
Hirano M, Kurita S, Sakaguchi S. Aging of the vibratory tissueof
human vocal folds. Acta Otolaryngol (Stokh), 1989; 107: 428-33.14.
Woo P, Casper J, Colton R, Brewer D. Dysphonia in theaging: Physiology versus disease. Laryngoscope 1992;
102 139-44.
15.
CritchleyEMR.
Speech disordersof
Parkinsonism. A review journal of neurology. Neurosurgery and Psychiatryl98l:
M:751-58.16.
Ramig L, Bonitati C, Lemke J,Honi
Y. Voice treatmentfor
patients with Parkinson disease: Developmentof
an approachand
preliminaryefhcacy data. Journal
ofMedical Speech-Language Pathology 1994; 2'. 19 I -209.
17.
DromeyC,
RamigLO,
JohnsonAB.
Phonatory andarticulatory changes associated
with
increased vocal intensityin
Parkinson disease: a case study. Journal ofSpeech and Hearing Research 1995; 38: 751-64.
18.
Ramig
LO,
Dromey
C.
Aerodynamic mechanisms underlying treatment related changesin
vocal intensity in.,
3.
4
6
8
9
174 Hendarto and Gray
patients
with
Parkinson disease. Joumalof
Speech andHearing Research L996; 39: 798-807.
Ramig
L,
CountrymanS,
ThomsonL,
Horri
Y. Comparisonof
two formsof
intensive Speech.treatmentfor
Parkinson disease. Joumalof
Speech and HearingResearch 1995; 39: 1232-51.
Ford
CN,
BlessDM,
L,oftusJM.
Role
of
injectable collagenin
the treatment of glotic insufficiency:A
Studyof
119 Patients.Ann Otol
Rhinol Laryngol 1992;l0l:
237-47.
Ramig L, Countryman S, O'Brien C, Hoehn M, Thomson L. Intensive speech treatment for patients with Parkinson
disease: Short-and
long-term
comparison of
two techniques. Neurology 1996; 41 : 1496-1504.Med J Indones
Chan
RW,
'Ëtze
IR.
Viscosities
of
Implantable Biomaterialsin
Vocal Fold
Augmentation Surge.ry.Laryngoscope 1998; 108: 725-31.
Remacle M, Marbaix E, Bertrand B, Hamoir M, Eeckhaut
JVD.
Corectionof
glottic
insufficiencyby
collagen injection. Ann Otol Rhinol Laryngol 1990; 99:438-44. Ford CN, Staskowski PA, Bless DM. Autologous collagenvocal
fold
injection
A
preliminary
clinical
Study.Laryngoscope 1995; 105: 944-48.
Ford CN, Bless
DM.
A
Preliminary studyof
injectable collagen in human vocal fold augmentation. Otolaryngol-Head Neck Surg 1986; l:104-112.
22.
23.
24.
25
19.
20