254
StLstroast,rcro et al.Survival
Patterns of
Children
with
Rheumatic
Heart
Disease
Sudigdo
Sastroasmoro,Bambang Madiyono, Ismet N
Oesman, SukmanTulus
Putra,Najib Advani
Rheumatic fever
is
comnronly
considered
as 'social
disease'. The disease
has rarely been found
in
in-dustrial countrjes,
but_it is
still
prevalent
in
many
developing
countriesl-5 including
Indonesia. In
somesituations, however, rheumatic fever
may causeresur-gence
in
certain parts
of
some industrial
countries6indicating
thatthis
disease needscontinuous attention.
In the last
10years, admission
of children with
rheu-matic fever
andrheumatic
heart disease toour
Depart-ment
has been steady,
i.e.,
approximately
50-80
patients per year.
It
has beenour observation that
theaddition of
severalhospitals
in
Jakartawhich
carefor
pediatric cardiac
cases,
including
patients with
rheumatic
heart disease, has not reduced the numberof
Deparnnent of Child Health, Medical School lJniversity
of
Indonesia, JakartaMed J Indones
patients admitted
to the Department
of
Child Health,
Faculty
of
Medicine University
of
Indonesia Cipto
Mangunkusumo
Hospital,
Jakarta.It
is noted that the majority
of
rheumatic patients
in
developing counlries
do not
comply the
proposed secondaryprophylaxis, i.e., monthly administration
of
intramuscular
benzathinepenicillin.
This
would
place thepatients to
the dangerof recurrent
attacksof
acuterheumatic
fever, which may
result in further
damageof
the cardiac tissues, especially
in
those
who
havecardiac
involvement on the previous
attack.TIn
con-trast, many studies have indicated that the morbidity
and mortality
rates
of
patients
with
rheumatic
heartdisease, as a sequel
of
acute
rheumatic fever,
havedecreased
considerably
if
secondary
chemoprophy-laxis
isgiven regularly
and adequately. /To
the bestof
our knowledge there
has beenno study that
analyzesthe outcome
of patients
with
rheumatic heart
diseasein
the Indonesian
medical literature. This study
wasAbstrak
Makalah
ini
ntelaporkan hasil analisis kesintasan (sumival analyses) pasien penyakit jantung reunatik yang berobat di Bagian Iltnu Kesehatan Anak Fakultas Kedokteran Universitos Indonesia - Rumah Sakit Dr. Cipto Mangunkwuno, Jakarta, antara Januari l9B3 sanpai Desenber 1992. Dari 359 pasienyangdapatdianalisis, padaakhir penganatan,)'akni al<hir bulanke-120,69,1% pasiennasih hidup. Perbandingankuna
kesintasan berdasarkan beberapa larakteristik netnperlihatkan bahwa usia pada saat diagnosis dan junilahkatupyang terlibat berperan dalau prognosis, sedangl<anjenis kelanin, pendidil<an orangtua, dan status gizi tidak berhubungan dengan prognosis. Kesimpulanyang sana diperoleh bila dilakukan analisis univariat nnupun urultivariat terhadap 177 pasienyang telah diikuti selana 5 tahun atau lebih.
Abstract
We eranined the survival curves of patients v'ith established rheunatic heart disease treated at the Division of Cardiology, Departntent of Child Health, Faculty of Medicine University of Itrdonesia Cipto Mangunkusunto Hospital, Jakarta during the period of January 1983
until Decenber 1992. There were 359 patients availablefor analysis. At the end of the 120-nonth observation,6g,I % patients were still alive. Conparisons of several curves based on certain characteristics showed that age at the tine of tliagnosis and the nunùer of valves involved were associated wilh survival, while sex, parental education, or nutritional status were not. Closer exatnination of 177 patients t'ho had conpleted 5 )'ears of follov,-up, both using univariate and nultivariate analyses (logistic regression analysis) confirtned the results of sun'ival anab'ses. We conclude that age at the tine of diagnosis and the nuntber of valvar int'olvernent are sîrong detertuinants
for
the prognosis of children v'ith rheunntic heart disease.such
patients, and determine some factors
associatedwith
theoutcome.
METHODS
Records
of
all
cardiac
patientsadmitted
to the Depart-mentof Child
Health,
and attendantsof
theOutpatient
Clinic
of
the
Division
of
Cardiology,
Department
of
Child
Health, Cipto Mangunkusumo Hospital
were
available
in our database record. These served as a data basefor
our study. We collected
records
of
patients
with
the diagnosis
of
acute
rheumatic heart
disease treatedduring
thelast 10
years(from
January
l,
1983up to
December
31,
1992). Only patients
living
in
JakartaMunicipality
andits surrounding
area(Bogor,
Bekasi,
and TangerangDistricts)
wereincluded in this
study.
Patient diagnosis and
management
The diagnosis of acute
rheumatic
fever was establishedeither using
revised
or
modified
Jones criteria.8
Patients
with
the
diagnosis
of
acute rheumatic fever
were hospitalized
for
several weeks,
and then
were
followed
in
the
Outpatients
Clinic.
Monthly
ad-ministration
of benzathinepenicillin
were proposedfor
all
patients.
In
every visit they
were watched
for
thepossibility of
recurrent
attacksor
the development
or
progression
of
cardiac involvement.
Patients
who
had cardiovascular
sequelae,either
im-mediately following
acute attack
or evident
later
on,were
classified
as patients
with
rheumatic heart
dis-ease. Patientwho
werereferred
for
the managementof
establishedrheumatic
heart disease weregenerally
nothospitalized,
unlessthey are
severely
distressedor
thepossibility of
anew acute rheumatic attack
could
not
beexcluded.
They
were also
managedon OPD
basis,with
theadministration
of monthly (or
every
3 weeksfor
severe cases)benzathine
penicillin.
Patients
with
frank
or
subtle congestive heart
failure, as
usually
indicated
by
the
presence
of
decrease exercise
tolerance,
were given
anticongestants, mainly
digitalis,
diuretics,
andin
some cases,vasodilators.
The diagnosis
of
valvar abnornrality was
based
onclinical findingse'Io
and was subsequently
supportedby other non-invasive diagnostic
nrethods,i.e.,
chestX-ray,
electrocardiography, and
echocardiography;
the latter
has beenroutinely
performed
since
1986in
cardiovascular problem.
Criteria
for
clinical and
echocardiographic
andDoppler
study were
described.l."whe.e.lo-
12Data collection
For the purpose
of
thestudy
thefollowing information
from each
patient wascollected
: sex, date of diagnosis, age atdiagnosis, parental education, number
of
valvar
involvements, nutritional
status
at the time
of
diag-nosis, dateof
loss tofollow
up, and dateof
death.V/ith
regard
topatient's survival
status, thefollowing
steps wereperformed:
l.
From January
1993
to
April
1993,
all registered
patients who
madefollow
upvisit
to theOPD were
identified; they were included
in
the
survivor (or
eventfree) group.
2.
To
thosewho did
not
show
up
in
the OPD during
that 4-month period, a letter containing a
simple
questionnaire was
sent;only
important
information
was askedfor
(lastvisit
to thehospital, and
survival
status,including
dateof
death).
To
thosewho did
not
respond
to
the
first
letter,
asecond letter
was sent.If
both
letters were not responded in 2 rnonths,2
field workers
madea home
visit
asking
for
the necessaryinformation.
If the
patient's
address wasnot found,
then he
or
she
was
labelled as loss
tofollow-up.
Patients
with
rheumatic heart
disease
were
groupedaccording
to
their
age
at the time
of
diagnosis
into
thosewho
were
lessthan
8 years and thosewho
were8
years
or older. The
socio-economic status was
ar-bitrarily
groupedaccording
to the parentaleducational
level, i.e. by
averaging
mother's
and
father's formal
education,
into
those
with
9
years
or
more,
or
thosewith
less
than
9
years
of
formal
schooling.
The
patient's nutritional
status was assessed
by
using
thesimplified classification of Wellcome Trust
Party,
as-256
Sastroastnoro etal-Statistical
analyses
The
overall
survival
curve
was constructedusing
Cut-tler-Ederer method,
Similar survival
curves were
alsoconstructed
after grouping the
patients
according
to
sex (male or
female),
age group at thetime
ofdiagnosis
(8
years
or
older,
or
less
than
8
years),
number
of
valves
involved
(l
or more thanI
valvar
involvement),
nutritional status (well-nourished,
undernourished/
malnourished),
and parental educational status (9 yearsor
more,or
less than 9 yearsof formal
schooling). For
eachpair
of
grouping
ahypothesis testing
wascarried
out
by
using log-rank statistical test. The survival
analyses wereperformed by using True-Epistat
statis-tical
program.
Patients
who
had been
followed-up
for
5
years, i.e.,
those who had
been diagnosed between
January
l,
1983
through December
31,
1987,
were
analyzed
separately.
For
this
group
of
patients univariate
analyseswere performed using *2 fo. difference
be-tween 2 independent proportions,
and the Oddsratios
werecalculated.
We alsosupplied
95confidence
inter-vals wherever appropriate,
andused
p
<0.05 for
thelevel
ofsignificance. A logistic
regression analysisby
using
SPSS-PC was
perfornred
for
such patients, to
determine
therole
of
severalrisk
factors
onsurvival.
RESULTS
The
total
number of patientswith
the diagnosis of acuterheumatic fever
or
rheumatic
heart diseaseduring
theI O-year
period'(January
1, I 983 to December 31,1992)
was547. Details
of
thediagnosis
and managementof
the patients have been described elsewhere.
l3
For this
particular study 32 patients were excluded
becausethey
lived
outside
JakartaMunicipality
and surround-ings.Of
the remaining
5 15patients,
156 were freefrom
cardiac involvenrent; they were not
considered
for
further
analysis.Therefore
atotal
of
359patients were
left for survival
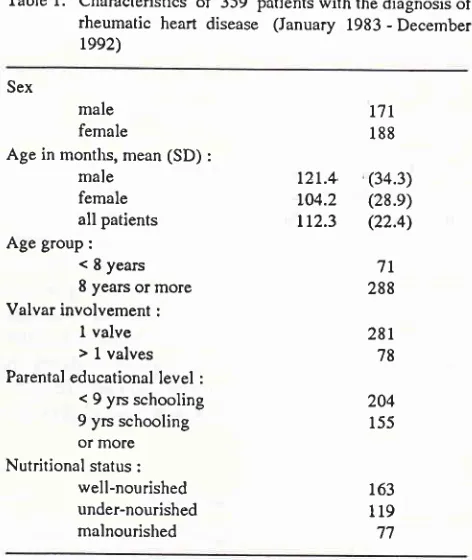
analysis.The clinical
and demographic
characteristics
of
the359 patients
at
the
time of
diagnosis are depicted
in
Table
l. The distribution
of
valvar involvement
is
depicted in Table
2which
shows thatmitral
valve
wasthe most
commonly valve involved,
followed
byaortic
valve.
Tricuspid
valve
wasonly affected
insmallnum-ber
of
patients; we
did not
diagnosepulmonic
abnor-mality in
any
of
our
patients.Med J Indones
Table
l.
Characteristicsof
359 patlents with the diagnosisof
rheumatic heart disease (January 1983 - December
ree2)
Sex
male female
Age in months, mean (SD) :
male female all patients Age group:
< 8 years 8 years or more Valvar involvement :
I
valve > 1 valvesParental educational level :
< 9 yrs schooling
9 yrs schooling or mole Nutritional status :
well-nourished under-nourished malnourished
t'll
188t2r.4.
(34.3)104.2
(28.e)tt2.3
(22.4)7t
28828t
78 204 155 163 119 77Table
2.
Valvar involvementin
359 patients with rheumatic heart diseaseDiagnosis No. of patients
Isolated mitral regurgitation Mitral regurgitation + mitral
stenosis
Mitral regurgitation + aortic regurgitation
Mitral regurgitation + tricuspid
regurgitation
Isolated mitral stenosis
Isolated aortic regurgitation
l8
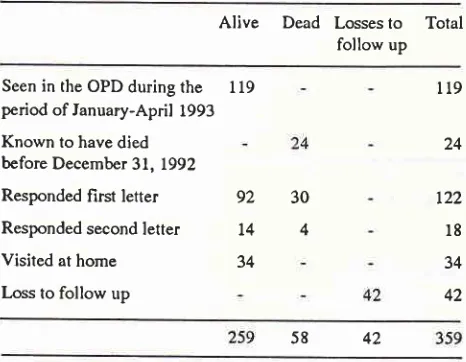
234 54 65.2 15.0 5.0 t.7 9.5 3.6 6 34 13Data
on
survival
status
[image:3.595.322.558.87.367.2] [image:3.595.325.560.441.591.2]Seen in the OPD during the period of lanuary-April 1993 Known to have died before December 31, 1992
Responded first letter
Responded second letter Visited at home Loss to follow up
of
the
first
letter
was reasonably
high,
i.e.,
122
(56.5%). When the second
letter was sent
to those who had not responded, 18 more responses were obtained.The remaining
76 patients whosesurvival status were
not available were visited by 2 field workers, and it wasfound that 42 were loss to follow
up. The final status
of patients' survival
dataon December
31, 1992 was
as
follows:
alive 259 patients, dead
58 patients,
and losses to follow up 42 patients. See Table 3.Table
3.
Survival statusof
patientswith
rheumatic heart diseaseAlive
Dead Losses
to
Total follow upThere were 202 patients with rheumatic
heart diseasediagnosed between January
l,
1983to
December 31,
1987.Of
those,
only
L77have complete
information
regarding survival. They
were selected to enable us to analyzerisk factors
for death
in rheumatic patientswho
were followed-up for the same periodof time (5 years).
During
the 5-year period 32 of them died. They
were analyzedby univariate
aswell as multivariate
techni-ques for the followingvariables: sex, valvar
involve-ment, age group
at
the
time
of
diagnosis,
parentaleducation, and
nutritional
status.Univariate
analyses
The results
of univariate
analysesof the survivors
andwho died are depicted in Table
3. The table providespvalue
of
each analysis
with its
corresponding
OddsRatio (OR) and its
957o confidenceinterval. It appears
that sex
did
not associate
with
survival, neither did
parental educational
level and
nutritional
status at thetinre
of
diagnosis.
However, when the patients were
groupedinto those with
I
or more
than
I
valvar
invol-vement, a significant difference
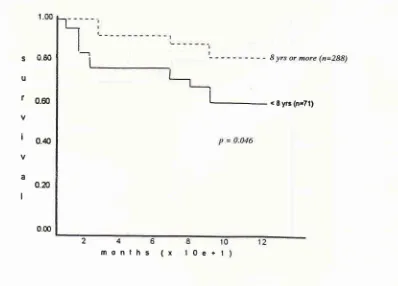
was obtained.Similar
results
were also obtained when the
.patients
werecompared according
to their age
group at the time
of
diagnosis.
Multivariate
analysis
Logistic
regression
wasapplied using
survival
as de-pendentvariable and sex, age group, valvular
involve-ment, parentaleducational level, and nutritional
status as independent variables. The resultsof
this analysis
aredepicted
in Table
4, which confirm
the results
of
multivariate
analyses, i.e., age group and valvar invol-vement were significant factors for survival, while sex,educational level, or nutritional
status were not.DISCUSSION
Our data confirmed previons reports and observations
that cardiac involvement
is
the most frequent
com-plication
in
rheunratic
fever
in
developing countries.
While in industrial countries
arthritis
is generally
the nrost common manifestationof acute rheumatic fever,
in
developing countries carditis is the most frequently
found manifestation.l0
Consequently patientswith
car-diac
sequelae
in
this
series outnunrbered patients
without cardiac involvement.
Table
I
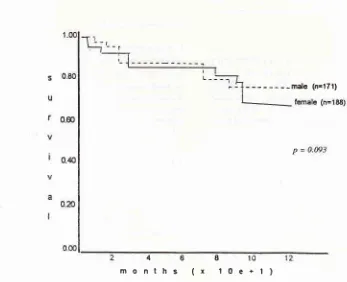
also shows that
there
was apparently
no
difference
between
sex
prevalence
in
rheumatic heart
disease,
but
patientsn9
lt9
92
t4 34
24
t22
l8
3442 30
4
42 58
SURVIVAL
ANALYSIS
[image:4.595.41.274.248.429.2]-Saçtroasnoro et al.
s
0.80u
r
0.60v
I
o.4o va 0.æ
I
0.00
[image:5.595.108.436.85.363.2] [image:5.595.113.460.416.698.2]months
(x 10e+1)
Figure
l.
Overall lo-year survival curve of 359 parients with rheunntic heart diseaseMed J Indones
- - male (n=171)
4681
months
(x 10e+l)
s
u
t
I
a
I 0.80
0.60
0.40
0.2)
9 yrs or morc(rrÎ55) < 9 yis (n=204)
P = 0.092
246
[image:6.595.113.511.416.702.2]months
(x
10e+t)
I
10Figure
j.
Contparison of l1-year survival cun'es ofpatients with rheunaric hart disease according to parental educational levels
o.EoU
r
o.æv
i
o.æv
a
0.æ
I
0.00
mont
hs
(x
0e+
< E yr3 (n'71,
260
sastroasnoro et aI.s
u
f
v
i
a
I
Med J Indones
0.60
o.4
0.æ
I
246
months (x
1- - - '1 valve (n=2El)
> 1 valve (n=78)
P = 0.02
[image:7.595.169.475.94.358.2]I
10e+
Figure 5. Conytarisott ofsurvival curveof palient v,ith rheurnaric heart disease according to the nunber ofvalves involved
10
121)
nen
S J.re
U
r
0.æv
I
o.€
Va
0.æ
I
0.00
well-nourosed (n=163)
undcr/rmlnourished (n=1 9Q
P = 0.144
I
010
e+1)
6ths
(x
[image:7.595.167.514.418.698.2]No
of
patients
Alive
Dead Pvalue
Or 95% ClSex
male female Age at diagnosis
< 8 years 8 years or more Valvar involvement
I
valve >I
valveParental education
< 9 years
9 years or mote Nutritional status
well-nourished undemutrition malnutrition
4t
r36 L4l8
t4
l8
7t
74 27ll8
85 92l9
l3
t2 t4 6 0.735 0.005 0.002 0.875 0.355 t.234 0.294 3.679 0.8690.535 ro 2.856
0.121 to 716
1.527 .o9.024
0.371to2.O2O LL2 65 101 76
8l
59 3797
l0
48
2282 63
69 45
3l
OR = Odds Ratio; Cl = Confidence Intervals
Table 5. Logistic regression ofseveral risk factors for survival
Variable
SE
Waldsig
df
Exp. BSex Valv Age &luc Nutr -.7236 -.0209 -.0422 -.8399 -.4212 .344t .0023 .0211 .o377 .t923 4.2323 32.4257 28.3265 6.298t 7.6690 .6672 .0287 .0334 .2367
.7t32
-.to12 -.33409 -.3079-. I 102
.232r
.36t2
.9971 .6759 .420t .3400I
I
I
I
I
valv
-
valvular involvement; Educ = parcntal education; Nutr-
nutritional statusaged less than 8 years were
definitely
fewer
than those aged 8 yearsor older.
series.
This
type
of
tesion usually
follows
acute
rheumatic
process, either at thefirst
attack orrecurrent
attacks.
When
sever
it
may
cause cardiac
failure with
pulmona
on; however,
massivepulmonary
edemais
untered.Mitral
lesionand other parts
of
the valve. Endocarditis
is
rarely
found
in
isolated
severemitral
regurgitation.
Mitral
stenosis,
either alone
or in
combination with
mitral
regurgitation
wasfound
in
many cases, someof
262
Sastroasnoro et al.literature
from
developing countries.
In
contrast,
in
industrial
countries stenosis
of
the
mitral
orifice
develop
fairly slowly,
yearsafter
the acute attack.The
underlying
mechanism
of
this phenomenon is not
un-derstood.
The development
of
established
organic
mitral stenosis
may further
increase
the
pulmonary
arterial
pressure
leading
to
pulmonary
hypertension
and increase
the
risk of right
heart
failure
and death.Moderate
mitral
stenosismay
betolerated
well
by
thepatient,
but
severe
mitral
stenosis
(mitral valve area
lessthan
257onormal)
is usually
associatedwith left
atrial hypertension
leading to severepulmonary
hyper-tension. This
will
eventually result
in
right cardiac
failure.
The next most common valve affected
is
the
aortic
valve, i.e.aortic insufficiency.
Patients
with nrild
tomoderate
rheumatic aortic regurgitation usually
cantolerate and
rarely
affects
their daily
activity.
Deterioration usually
is
causedby rheumatic
activity,
or
endocarditis.
Many
adolescentswith
severeaortic
regurgitation
may be
totally
asymptomatic and
can toleratewell untill
the 3rd or 4th decade. Nevertheless, more than 50% patientsdie
within
20 yearsafter
diag-nosis.
We found
only
a
small
number
of
patients with
tricuspid
abnorn-rality, andno patients
with pulmonic
disease.Tricuspid regurgitation
is usually
causedby
right
venticular
dilatation
secondary topulmonary
hy-pertension.
This
implies
left
cardiac involvement,
usually
a
combination
of
mitral
regurgitation
and stenosis.With
the availability
of
echocardiography and
Dop-pler, clinically
unrecognizable
murmur
rnay
bedetected. Echocardiography
haèan
important role in
the long-term
nranagementof
patients
with
rheumatic
heart
disesase;even a minimal regurgitation
can
be detected.The
degreeof
aortic or mitral
regurgitation
can be estimated
with
certain
accuracyby
usingecho-Doppler technique.
This
method has
increased
thebenefit
of
periodical assessment
of
patients with
rheumatic
heart disease.Although different valvar
lesions
may
lead
to a
dif-ferent
causeof
death,in
general the causeof
deathin
patients
with rheumatic
heart disease is associatedwith
cardiac
failure,
endocarditis, or dysrhythmias. We
did
not have data on
recurrence
or
the
development
of
endocarditis
in
this series; however endocarditis
isknown
to
affect lhe
prognosis
of
patients with
rheumatic heart disease.
It
is
understandable
thatpatients who
hasmore
than
I
valvar
lesion, usually
aMed J Indones
combination
of mitral
andaortic regurgitation,
have ahigher
mortality rate than those
with only a single
valvular
involvement.
The
managementof patients
with
chronic
rheumatic
heart disease must
include
aconsideration
of
invasive
treatment, eitherin
theform
ofballoon dilatation
of thestenotic
mitral
valve,
orby surgical
valvotomy.
Short-term results indicate that balloon
dilatation
give
com-parable results compared
to
surgical
valvotomy.
Obviously,
surgical
valve
replacement
is difficult,
or
even impossible to be performed
in
the
pediatric age
group,
since thepatient is
growing
anddeveloping.
With regard
to
survival,
in
general
our
data support
previous
evidence
that
rheumatic heart disease
decrease
the
life expectancy, and
many factors
con-tribute to
theoverall prognosis
of
patients
with
estab-lished rheumatic heart
disaese.The
generally known
most
important factor
for the development
of
severevalvar abnormalities
is inadequate
administration
of
antibiotics
(usually long-acting
penicillin), in
patientswith
existing valvar
damage.
This
encompliance
in-vites the
occurence
of
new
streptococcal
pharingitis
that may lead
to
another attack
of
acute rheumatic
fever.
18-
We
did
not include compliance
as
a risk
factor of
death,since
it
wasquite
difficult
to
classify
the
patients
into
groupsaccording to their compliance
to prophylaxis protocol,
since almost
all
patients
did
not comply.
The
severity of
cardiacinvolvement in
our parents wasalso
not
considered in
this
analysis
with
assumption
that
mild
valvar
abnormality
is
rarely
associatedwith
significant
other
valvar
abnormality.
We did not
have enough data to
validly classify
thepatients according
to
the
family's
sosio-economic
level. The
difficulties
arise when we
haveto consider
family
inconre, since
it
is notoriously known
that
es-timation
of family
income
is rarely reliable.
Further-more,
including nrother's or father's
occupation
into
the
independent
variable
with
also result
in
similar
situation, since many
of
our
parents
did not have a
permanentoccupation. For
those and other reasonswe
chose
to
average
parental
education as
a proxy for
family's
sosio-economic
status.Obviously
thisshould
have
affected our unusual result, i.e.
thatlhere
was noassosiation
between patient's prognosis and
sosio-economic level.
paren-Vol 4, No 4, October - Decetnber 1995
tal education, sex,
and
nutritional
status
were
not.Table
4
also
demonstrates
that
in
patiens who
hadfollow-up of
5 years, the casefatality
ratewas
321177(l8.l7o)"
The facts that significanr findings
in
univariate
analysesremained
soin logistic
regressionanalysis suggested that such associations 'were strong.
The major
weaknessof
this study
is that we do
not
know
the exacttime when
therheumatic
heart diseasestarted
in
mos(
of
our
patients.
This is
caused
by
atypical
phenomenon
in
patients
with
rheumatic
heartdisease
in
mostdeveloping countries,
i.e., that manyof
them
fail
to indicate
with certaintly when the first
symptoms
of
acute rheunratic
fever occurred.
Someauthors refers this phenomenon as to silent
carditis. We
are
of
the
opinion
that
it
will
take many
yearsbefore
we
could
get abetter
information
regarding
thebegin-ning
of
therheumatic
processin all
patients, i.e.,
until
everyone has an easy access to health services
offering
adequate
facilities
to diagnose acuterheumatic
fever.In
conclusion,
survival
analysesof our
patients
with
chronic
rheumatic heart
diseaseshow
that
ageat
thetime
of
diagnosis and the number
of
cardiac
valve
affected determined
the prognosisof
thepatient,
while
nutritional
status, sex, andparental education
did
not.Further study
involving
more independentvariables
isnecessary
for determining overall
factors
influencing
the
prognosis of children
with
rheumatic
heart disease.Acknowledgment
The
authors
wish to thank Mr,
Theo Stijnen,
Statis-tician, Department
of Epidemiology
andBiostatistics,
Erasmus
University,
Rotterdam,
for
his suggestionsin
managing
thesurvival
data.REFERENCES
l.
Agarwal BL. Rheumatic heart disease unabated indevelop-ing countries. Lancet 198 l;ii:910-1.
2. Ayoub EM. Acute rheumatic fever.
In:
Adams FH,Ern-manuillides GC, Riernenschneider TA, editors. Mos' Heart
disease in infants, children, and adolescents. 4th ed, London:
Williams & Wilkins, t989;692-7O4.
3. Taranta A, Markowitz M. Rheumatic fever. 2nd ed. Boston:
Kluwer Academic Publisher, 1989
4. Sievero
I,
Hall P. Incidenceol
acute rheumatic fever. BrHeart
I
1971;33:833-6.5. Majeed HA, Khan N, Dabbagh M, et al. Acure rlreurnatic
fever during childhood in Kuwait: the mild nature the initial
attack. Ann Trop Paediatr 198 l; l : l3-20.
Rheunatic Heart
Disease
2636. Veasy LG, Wiedrneier SE, Orsrnond GS, et al. Resurgence
of
acute rheumatic feverin
the intennountain area of theUnited States. N Engl J Med 1981;316:42I-7.
7. Markowitz M. The decline of rheumatic fever: role of
medi-cal intervention. Pediatrics 1966;106:545-50.
8. Committee on Rheumatic Fever and Infective Endocarditis
of
the Council on Cardiovascular Diseasein
the young,America Heart Association. Prevention of rheurnatic fever.
Circulation 1985;70: I I t 8A
-l
122L.9. Barlow JB, Pocock WA. The problems of nonejection
sys-tolic clicks and associated mitral systolic murmurs: empliasis
on the billowing mitral
leaflet syndrorne.Am
Heart J1975;90:636-9
10, Wahab AS. Penyakit jantung reumatik. In: Sastroasmoro S,
Madiyono
B,
editors. Buku ajar kardiologi anak. Jakarta:Ikatan Dokter Anak Indonesi a, L994.
ll.
Helmcke F, Nanda NC, Hsiung MC, et al. Color Dopplerassessment of mitral regurgitation with orthogonal planes.
Circulation 1987;75 : 175-83.
12. Putra
ST,
SastroasmoroS,
MadiyonoB,
Oesman IN.Echocardiographic diagnosis
of
acute rheumatic fever inchildren. Paediatr Indones 1993;33:227 -31.
13. Madiyono B. Diagnosis of rheumatic fever and rheurnatic
heart disease:
which modification?
Paediatr Indones1994;34:78-87.
14. Hudson REB. Cardiovascular pathology vol. 3. Baltimore:
Williams & Wilkins, 1970;549-81.
15. Markowitz
M,
GordisL.
Rheumaric fever. philadelphia:Saunders,1972.
16. Combined Rheumatic Fever Study Group.
A
cornparisonof the effect of prednisone and acetylsalicylic acid on the
incidence of residual rheumatic heart disease. N Engl
I
Med1960;262:895-902.
17. Cornbined Rheumatic Fever Study Group. A comparison
of
short-term, intensive prednisone and acetysalicylic acid
therapy in the treatment of acute rheumatic fever. N Engl
I
Med 1965;272:63-70.
18. Sastroasmoro S, Madiyono B, Oesrnan IN, putra ST.
Bac-terial endocarditis in children: Clinical and laboratory
find-ings, and the role of echocardiography in its diagnosis and
treatrnent. Paediatr Indones 1989;29: 188-98.
19. Gordis L. Changing risk of rheumatic fever. In: Shuhnan S,
Editor. Management
of
pharyngitisin
an era of decliningrheumatic fever:
fie
86th Ross Conference on pediatricResearch. Colonrbus, Ross Laboratories, 1983, pp7-13.
20. Tonrpkins DG, Boxebaum B, Liebrnan
I.
Long-terrnprog-nosis of rheurnatic fever patients receiving regular
intrarnus-cular benzathine penicilin. Circulation 1972;45.543-5l.
21. Gotsman MS, van der Horst RL. Surgical management
of
severe
mitral
valve
diseasein
childhold.
Am
Heart J1975;90:685-92.
22. Rachrnan OJ. Kardiologi intervensional. In: Sastroasmoro S,
Madiyono B, editors. Buku ajar kardiologi anak. Jakarta: