Relationship between plasma lipid proile and the severity of diabetic
retinopathy in type 2 diabetes patients
Rianita1, Saptawati Bardosono1, Andi Arus Victor2
Abstrak
Penelitian ini bertujuan untuk mengetahui hubungan antara proil lipid darah dengan derajat retinopati diabetik penderita DM tipe-2. Penelitian potong-lintang pada 52 pasien retinopati diabetika dilaksanakan di Poliklinik Mata, Rumah Sakit Cipto Mangunkusumo, Jakarta. Data yang dikumpulkan meliputi data demograi, gaya hidup, lama menderita DM, pemeriksaan isik dan antropometrik, asupan lemak, asam lemak dan kolesterol data kadar gula darah puasa, A1C, kolesterol total, kolesterol-LDL, kolesterol-HDL and trigliserida, dan pemeriksaan fundus. Analisis statistik yang digunakan adalah uji chi-square untuk mengetahui hubungan antara proil lipid darah dengan derajat retinopati diabetik. Subyek terdiri dari 20 orang laki-laki dan 32 orang perempuan dengan rerata usia 53,8 ± 5,2 tahun. Sebanyak 53,8% telah didiagnosis DM selama >10 tahun, dengan rerata IMT adalah 24,1 ± 3,3 kg/m2 dan 38,5% diklasiikasikan sebagai obes I dan II. Rerata kadar gula darah puasa 157,5 ± 71,8 mg/dL, dan A1C 9,1 ± 2,4 %. Sebanyak 40,4% subyek mempunyai kadar kolesterol total darah tinggi, 34,6% kadar kolesterol-LDL darah sangat tinggi, dan 65,4% dengan kolesterol-HDL dan trigliserida darah normal. Derajat keparahan retinopati diabetika ditunjukkan dengan adanya 61,6% subyek dengan retinopati diabetika non-proliferasi berat (NPDR) and retinopati diabetika non-proliferasi (PDR). Kesimpulannya, belum dapat dibuktikan adanya hubungan yang bermakna antara proil lipid dengan derajat retinopati diabetika. (Med J Indones 2008; 17: 221-5)
Abstract
This study aimed to determine the relationship between plasma lipid proile and the severity of diabetic retinopathy in type 2 diabetes patients. A cross sectional study was done in Ophthalmologic Clinic, Cipto Mangunkusumo General Hospital, Jakarta for 52 diabetic retinopathy (DR) patients. Data collected were demographic, life style, duration of diabetes, physical and antropometric examinations, fat, fatty acid and cholesterol intake, fasting plasma glucose, A1C, total-, LDL-, HDL-cholesterol and triglyceride level, and fundus examination. Statistical analysis was done using chi-square test to see the associations between plasma lipid proile and DR in type 2 diabetes patients. Subjects comprised of 20 males and 32 females diabetes patients with mean age of 53.8 ± 5.2 years. As much as 53.8% had been diagnosed as DM for >10 years. The mean value of BMI was 24.1 ± 3.3 kg/m2 and 38.5% were classiied as obese I and II. The mean value of fasting plasma glucose was 157.5 ± 71.8 mg/dL, and A1C was 9.1 ± 2.4 %. For lipid proile, 40.4% had high total cholesterol level (>240 mg/dL), 34.6% had high and very high LDL-cholesterol level (≥160 mg/dL), and 65.4% had normal HDL-cholesterol (40-60 mg/dL) and triglyceride level (<150 mg/dL). For the severity of retinopathy, 61.6% had severe non-proliferative diabetic retinopahy (NPDR) and proliferative diabetic retinopahy (PDR). In conclusion, there were no signiicant associations between plasma lipid proile and the severity of diabetic retinopathy. (Med J Indones 2008; 17: 221-5)
Keywords: Fat intake, lipid proile, diabetic retinopathy
Diabetes mellitus is continuing to become a health problem because the prevalence of DM increases dramatically over the past two decades.1 Prevalence of diabetic retinopathy (DR), the ophthalmologic com
1 Department of Nutrition, Faculty of Medicine University of Indonesia, Jakarta, Indonesia
2 Department of Ophthalmology, Faculty of Medicine University of Indonesia/Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia
plication of DM, in Indonesia is 27.1%.2 Strategies to prevent the development and progression of DR is very crucial regarding its blindness end result. Risk factors of DR among others are hyperglycemia, hypertension, pregnancy, obesity and dyslipidemia.36 Dyslipidemia associated with DM are hyper triglyceride and decrease HDLcholesterol concentrations.1,7
Chen et al found that dyslipidemia, not hyperglycemia,
in microvascular human retinal vascular endothelial cells.8 High lipid levels are known to cause endothelial
dysfunction via a local inlammatory response resulting
in the release of cytokines and growth factors, activation
of oxygen-sensitive biological changes in vessel walls, increased low-density lipo protein (LDL) oxidation, and quenching of nitric oxide. Endothelial dysfunction
in diabetic vasculature results in bloodretinal barrier
breakdown that will lead to DR. Elevated level of LDL
and triglycerides in DM have been linked with higher levels of advanced glycation end products, which play an important role in the pathogenesis of diabetic complications.6,9,10
Previous studies found that high dietary fat intake among DM patients at Cipto Mangunkusumo General Hospital (27.3%33% total energy intake).11,12 High
intake of dietary fat will inluence plasma lipid proile and worsen the existing abnormal metabolism. This
research was aimed to investigate the associations
between dietary fat intake, plasma lipid proile and DR
in type 2 diabetes patients.
METHODS
Fifty two diabetic retinopathy patients were consecutively recruited from Ophthalmology Clinic at Dr Cipto
Mangunkusumo General Hospital, Jakarta. The inclusion criteria was age under 60 years while the exclusion
criteria were pregnant, lactating woman and/or taking antihyperlipidemic agent. All participants were given
written informed consent. The study protocol was approved by The Medical Research Ethics Committee of The Faculty of Medicine University of Indonesia. This was a cross sectional study to collect data by
interview, medical records, physical and laboratory
examination. Data collected were demographic
characteristics, life style, duration of diabetes, physical
and antropometri examinations, fat, fatty acid and
cholesterol intake by FFQ semiquantitative method, laboratory (fasting plasma glucose, A1C, total cholesterol, LDL, HDLcholesterol and triglyceride
level), and fundus examination.
Body weight was measured using a digital Seca scale with accuracy to the nearest 0.1 kg. Body height was measured using a microtoise with accuracy to the
nearest 0.1 cm. Both measures were used to classify nutritional status of the subjects based on body mass
index (BMI). Nutrients intake was analyzed using
data provided from the semiquantitavie foodfrquency
questionnaires. Blood samples were analyzed for
glycaemic control (blood glucose and A1C) and
classiied using local reference (PERKENI, 2006) and
lipid proile was analyzed by using high performance liquid chromatography and classiied using NCEP-ATP III 2001 reference. Classiication of retinopathy was
based Victor et al (1999) reference.
The data were analyzed using SPSS version 11.5. All
group data were presented as frequency distribution (proportion) and the average values was presented as means ± SD for the normal distribution data and
as median (minimum-maximum) for the non normal
distribution data. Data were analysed statistically using
chi-square or ischer exact test to see the associations
between plasma lipid proile and DR in type 2 diabetes patients. The minimal level of signiicance was set at p<0.05.
RESULTS
Subjects comprised of 20 (38.5%) males and 32 (61.5%) females, with mean age of 53.8 ± 5.2 years. Majority
of the subjects (80%) had low and moderate education
level, 94.2% were above the poverty line, 53.8% had been diagnosed DM for >10 years, 88.5% were non-smokers and 57.7% had low physical activity index.
The mean value of BMI was 24.1 ± 3.3 kg/m2, which
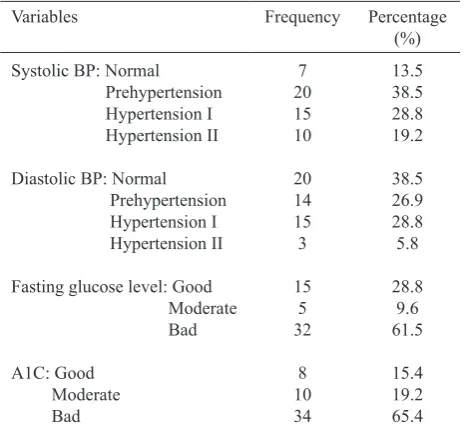
were within the risk range for obeisty and 38.5% of the subjects were classiied as obese I and II (Table 1). The mean value of systolic blood pressure was 137.4 ± 21.8 mmHg, diastolic blood pressure 81.5 ± 21.8 mmHg, fasting plasma glucose 157.5 ± 71.8 mg/
dL, A1C 9.1 ± 2.4 %. As much as 40.4% had high total cholesterol level, 34.6% had high and very high
LDL-cholesterol level, and 65.4% had normal HDL-cholesterol and triglyceride level (Table 2). The median of dietary fat intake was 39.5 (8-146) g/day and 78.8%
had high fat intake, 94,2% had high SAFA intake, all of
the subjects had enough PUFA and MUFA intake, and 94,2% had enough cholesterol intake (Table 3).
Table 1. Characteristics of the subjects (n=52)
BMI, body mass index
Table 2. Physical examination and laboratory data of the subjects (n=52)
Table 2. Physical examination and laboratory data of the subjects (n=52)
BP, blood pressure; A1C, glycosilated haemoglobin; LDL, low density lipoprotein; HDL, highdensity lipoprotein
Table 3. Fat, fatty acid and cholesterol intake of the subjects (n=52)
Intake Frequency Percentage (%)
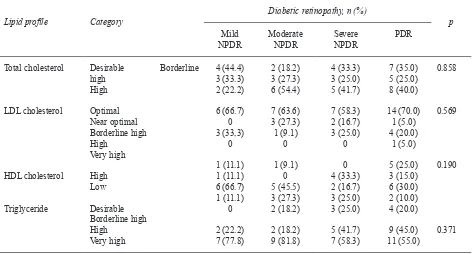
Table 4. Associations of lipid proile and diabetic retinopathy (n=52)
Lipid proile Category Diabetic retinopathy, n (%) p
Mild
NPDR Moderate NPDR Severe NPDR PDR
Total cholesterol
LDL, low-density lipoprotein; HDL, high-density lipoprotein; NPDR, non-proliferative diabetic retinopathy; PDR, proliferative
diabetic retinopathy
DISCUSSION
The present study showed that most of the subjects were diagnosed as having severe DR (severe NPDR and PDR). As much as 25% of the male subjects were
diagnosed as having PDR and most of the female subjects
had moderate NPDR. The Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) showed a
similar trend where male had more PDR than female.13
The mean age of the subjects was 53.8 ± 5.2 years. Epidemiologic studies showed an increased prevalence
of DR with increasing age in the youngeronset of DM. Increases in growth hormone, insulinlike growth
factor 1, sex hormone, poor glycemic control have been hypothesized to explain the higher risk of DR in the
youngeronset of DM.14
This study didn’t ind any trend on the increased of
PDR subjects when total cholesterol level increased.
This condition might be related to the fact that most
There were no signiicant associations between plasma lipid proile and DR by bivariate statistical analysis. This could be explained by the fact that most
of the subjects had normal plasma triglyceride and
total cholesterol level. Abnormalities in lipid proile
that could be associated with DR are high plasma triglyceride and total cholesterol. Beside that, most of the subjects had poor glycemic control in which glycemic control is known as the most important risk
factors for DR. This result was similar to the study by Lyons et al that showed no signiicant association
between plasma triglyceride, LDL and HDL cholesterol level with DR. Lyons et al found that DR
had a signiicant positive association with LDL small-dense and signiicant negative association with HDL.16
It is concluded that there was no association between
plasma lipid proile and the severity of DR.
REFERENCES
1. Powers AC. Diabetes Mellitus. In: Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, editors.
Harrison’s Principles of Internal Medicine. 16th ed. New
York: McGraw-Hill; 2005.p.2152-93
2. Suyono S. Kecenderungan peningkatan jumlah penyandang diabetes. In: Soegondo S, Soewondo P, Subekti I, editors. Penatalaksanaan Diabetes Melitus Terpadu. Jakarta: Balai Penerbit FKUI; 2005.p.1-5
3. Kanski JJ. Clinical Ophthalmology. 4th ed. Oxford:
Butterworth Heinemann; 2000. p.465-79
4. Rand LI. Diabetes and the eye. In: Becker KL, editor. Principles and Practice of Endocrinology and Metabolism.
3th ed. Philadelphia: Lippincott Williams and Wilkins; 2001.
p.141823.
5. Van Leiden H, Dekker JM, Moll AC, Nijpels G, Heine RJ,
Bouter LM, Stehouwer CDA, Polak BCP. Blood pressure, lipids and obesity are associated with retinopathy. Diabetes
Care. 2002; 25: 1320-25
6. Ciulla TA, Amador AG, Zinman B. Diabetic retinopathy and diabetic macular edema. Diabetes Care 2003; 26: 2653-63
7. Krauss RM, Siri PW. Dyslipidemia in type 2 diabetes. Med Clin N Am. 2004; 88: 897-909
8. Chen W, Jump DB, Grant MB, Esselman WJ, Busik JV. Dyslipidemia, not hyperglycemia, induces inlammatory
adhesion molecules in human retinal vascular endothelial cells. Invst Ophthalmol. Vis Sci. 2003; 44: 5016-22
9. Miljanovic B, Glynn RJ, Nathan DM, Manson JE,
Schaumberg DA. A prospective study of serum lipids and risk of diabetic macular edema in type 1 diabetes. Diabetes.
2004; 53: 2883-92
10. Leiter LA. The prevention of diabetic microvascular complications of diabetes: is there a role for lipid lowering?. Diabetes research and clinical practice 2005; 68S2:
S3-S14
11. Fitriyani S. Korelasi antara kadar vitamin E dengan
malondilaldehida dan creactive protein plasma penderita
diabetes melitus tipe 2. Tesis Magister Sains. Jakarta: Ilmu Gizi Klinik FKUI; 2006
12. Ambarwati FD. Indeks glikemik dan beban glikemik kue tradisional di pasaran dan kue sejenis buatan sendiri yang ditambah serat makanan pada kelompok DM tipe 2 dan non
DM. Tesis Magister Sains. Jakarta: Ilmu Gizi Klinik FKUI;
2006
13. Klein R, Klein BE. The epidemiology of diabetic
retinopathy. In: Ryan SJ, Schachat AP, editors. Retina. 4th
ed. Philadelphia: Elsevier Mosby; 2006. p.1503-21 14. Klein R. () Retinopathy and other ocular complications
in diabetes. In: Porte D, Sherwin RS, Baron A, editors.
Ellenberg & Rifkin’s Diabetes mellitus. 6th ed. New York:
McGrawHill; 2003.p.66394
15. Durrington PN. () Hyperlipidaemia diagnosis and
management. 1st ed. London: Wright; 1989.p.166-94
16. Lyons TJ, Jenkins AJ, Zheng D, Lackland DT, McGee D, Garvey WT, Klein RL, The DCCT/EDIC Research Group.
Diabetic retinopathy and serum lipoprotein subclasses in
the DCCT/EDIC cohort. Invest. Ophthalmol. Vis Sci. 2004; 45: 910-18
17. Klein BEK, Moss SE, Klein R, Surawicz TS. The Wisconsin epidemiologic study of diabetic retinopathy.
XIII. Relationship of serum cholesterol to retinopathy and
hard exudate. Ophthalmology. 1991; 98: 1261-65
18. Haddad OAW, Saad MK. Prevalence and risk factors
for diabetic retinopathy among Omani diabetics. Br J