The
outcome of
pregnancy
among
Graves'
\ilomen
treated
with
PTU
Ali Imran
Mukhsin*,
Sarwono Waspa-dji#,tmam
Subelci#, Sidartawan Soegondo#, Asman Boedisantoso Ranakusuma#, Slamet Suyono#258
Mukhsin et alImportant changes
occur
in
thyroid
physiologic
featuresduring
pregnancy.
The
basal metabolic
rate increases about 20oÂ.Estrogen stimulates the
hepaticproduction
of
thyroid-binding globulin
(TBG), the
i
Division of Endocrinologt and Metabolism, Facultyof
Medicine, University of Indonesia, Jakarta, Indonesiai
Department of Medicine, Faculty of Medicine, Universityof
Ind ones ia. Jakarta, I ndo nes ia
Med J Indones
primary
transport
protein
for thyroid
hormone. TBG
serum concentration doubles
early
in
pregnancy. BecauseTBG binds
morethyroxin
andtriiodothyronin
thannormal,
total
serumtriiodothyronin
andthyroxin
concentration
nearly
double,
rising
well
abovenormal.
However,
free
(unbound) serum
thyroid
hormone concentrations fall
because
of
increasedbinding
but
remain
within
the
normal range.
Thethyroid
gland becomesoveractive, showing histologic
features
of
stimulation,
and
radioiodine
uptakeAbstrak
Hipertiroidisme
ysng tidak terkendali
pada ke Sebalilorya pengobatanyang berlebihan dapa!
persalinan, gangguan pertumbuhan dan perkem kehamilan dan persalinanakan berlangsung
hipertiroidisme dengan PTIJ pada ibu hantil terhadap fungsi tiroic
FTa dan TSH ibu yàng diperiksa setiap bulan dari mulai iehamilan sampai melahirkan. Kadar TSH bayi dievaluasi dari
tali
pusar dan pada saat persalinan juga dievaluasi kadar TRabtanpa kelainan bawaan, di antaranl'a ada yang dilah janlung
,
TSH dan kadar TRab berturul-lurut adala sedangkan rerata dosis total PTU (a 50 mg pertableantara skor dosis PTU selama hamil dengan kadar TSH bayi, nam
melahirkan. Disimpulkan penggunaan
PlU
selama kehamilan dengan hipertiroidisme aman bagi bayi yang dilahirkan bila dilakukan pemantauan yang ketat terhadap fungsi tiroid ibu.Abstract
t1nconlrolled Graves' disease in pregnant women might result in abnormalities of the development and growth of the fetus- Once becoming eurhyT,ifl on anfithyroiâ drug, the pregnancy might ensue toward lerm and normal delivery. Overtreatment however, mighl caure piobleris to the baby iuch as hl,pothyroidism and goitre, resulting in dfficulties at the delivery and growth problems ldter in their life. Evaluation on the outcom"'ol pr"gnor"y and the delivered babies among pregnant Graves' women wcts conducled. All the pregnànt Graves, mother attended oru:
ihyioid
ilini" *rr"
treated withPTU, the
dose were tailored according to' lhe levels of Ta/
-FTtand TSH of
the pregnant mother. Laboratory evaluation was done every
ntonlhfrom
lhe slarl of pregnancy up to the timeof
delivery, during which thT.fetus TSHfrom
the umbilical cord blood and the mother's serum TRab were also measured. There were altogetherl2 pregnant Graves'
u,omen completed their pregtrcncy during the year 1997. Some pregnancy ended with low SC due togtnîcobgic
iiaiùnn.
All
the babies born in this series *,ere normal, without apparent congenital anomalies. The mean birthweight,iearl
raté, TSH and TRob levels were 3053!
279 grams, 14.5 + 8.4 beat/minute, 6.4 + 6.7 ug/L respeclively. The mean serum TRab of the mother were l8.7ok. The averageronl
dose of PTU during pregnancy was 200-300 tablets of 50 mg. There was signif;cant correiation between the amount of PTÙ tublets consumed during the pregnancy and the levels of the umbilical cord blood THS level, but there was no corelation between the TRab and TSH levels of the born babies.It
was concluded that the use of PTU among pregnonl Graves' women, in conjunction with meticulous moniloring of pregwncy and thyroid function resulted in sde outcomeof
pregnancy.increases.
However, during
this time,
serum
TSH
declines to thelower
limits
of normal.r
The
prevalence
of hyperthyroidism
in
pregnantwomen
has beenreported
to
be
in
the
rangeof
0.05-0.2oÂ.In
9,453 early pregnant women residing in
Japan 0.4% had
hyperthyroidism
(mainly
with
untreated Graves' disease).'
Mild
to moderately
thyrotoxic
\ryomen
remainsovulatory
and is not necessarily tobe
infertile.
Infants
of poorly
controlled hyperthyroid mothers
areat
risk
of
prematurity, intrauterine growth
retardation,
andneonatal
morbidity, such
as
fetal
or
neonatalhyperthyroidism
due
to
transplacental
passage
of
TRAB (TSH
receptor
antibody). On the
other
hand, overtreatmeirtmay
cause neonatal hypothyroidism.3The management
of
Graves' diseaseduring
pregnancyhas been
studied intensively. The
therapeutic
goalswere
to
maintain the mother
in
apregnant euthyroid
or
slightly
hyperthyroid
state and to keep the fetusin
aeuthyroid
state.
Thyroid dysfunction and goitre
aresometimes
found
in
neonates
bom
to
mothers
with
autoimmune
thyroid
disease,due
to
maternal
TSH-receptor antibody
and
antithyroid drugs,
both of
which
arereadily transfened
across the placenta. 3-5This
study was carried
out
to
seethe effect of
using
pncphylthiouracilin
contolling
matemalhlperthyroidism
to the newboms/infants'
thyroid
function
status.MATERIALS
AND METHODS
This
crosssectional study
wasperformed at
Division
of Endocrinology and Metabolism, Department
of
Medicine, University
of
Indonesia
/
Dr. Cipto
Mangunkusumo hospital during
theyear
1997.Subjects
Twelve
neonates
bom
in
1997 were
consecutively
studied.
They were bom
to lZ
women
with
treated
with prophylthiouracil
during
.
The
treatment
follow up for
their
Graves' disease
was done
at
the
Division of
Endocrinology
and Metabolism,
Department
of
Medicine
University
of
Indonesia.Laboratory
studies
Serum
thyroxin levels (Ta) and TSH were
assayedfrom the
mothers using
radioirnmunoassay
with
acommercial
kit
(Amerlex-
M
Tr RIA kits)
at the
first
visit
and Ta was subsequently measured every 4 week.TSH
receptor
antibody
(TRAB) level
was
measuredby
Radio
Receptor
Assay (RRA)
with
Kit
Bio
International
at thetime
of
delivery.
Neonatal
umbilical
cord's blood
TSH
was
assessed atdelivery.
Antithyroid
drug
(propylthiouracil-PTLl)
wasgiven
toall
the
patients,
to
maintain the
serum thyroid
hormone
level
at the
meanT+
-
15ugdL,
the total
Ta levels
of
normal
pregnancy
without any thyroid
problems
in
our
previous study. The
total
amount
of
PTU
administered
was
calculated using
the
score
of
PTU
dose expressed as :Siore 0
:PTU
wasgiven
lessthan
100 tablets (50mg/tablet).
Score
I
Score 2 Score 3 Score 4Score 5
PTU
wasgiven between
l0l-200
tablets.PTU
wasgiven
between 201-300 tablets.PTU
wasgiven
between 301-400 tablets. PTU wasgiven
between 401-500 tablets. PTU wasgiven
above 500 tablets.Data
processing
The
collected data
were included
in
the
case recordform,
tabulated according
to
the aims of the
study. Thereafter they were edited,
coded, and storedin
thehard disk using
IBM
compatible personal
computerwith
the help
of
software
SPSSfor
window
release6.0 and presented
in
table andgraphic form.
Multivariate
analysis
was
performed
to find
out
thecorrelation
betweenfetal TSH
andpTU total
dose, aswell
as mother'sTSH
receptorantibody
atdelivery.
RESULT
Table
I
lists the
characteristics
of the
12
subjects (mothers and neonates)included
in
this
study.260
Mukhsin et alTable
l.
Characteristics ofthe SubjectsMed J Indones
patients
and,6
(50%o)patients
had
TRAB
levels
of
more
than l5oÂ,
but
1 patient (8.3%)
did
not
haveTRAB
data.Table
3.
Total dose (TD), dose score (SD) mean daily doseMDD),
durationof
administration(D),
monthof
gestationat
which PTU was
withdrawn (withd), mother's TRAB and TSH as measuredin
umbilical cord's blood.D
(days) llaemoglobine
Albumin
Median dose PTU (score)
MedianTRAB
Maternal Ta during pregnancy Neonatal TSH
Birth weight
Heart beats
3050
t
279.1
C134.5
+
8.4 beaVmin12.6+
0.84.3
!
0.42.5
r8.7 %
14.4
+
4.1 6.4 + 6.7gdL
mC/dLltgldL
pIU/mL
Table 2. Clinical Features of Maternal Hyperthyroidism
Withd TSH
TRAB(month)
UIU/mL (n
TD SD
MDD(tablets)
(mg)28
38 59 24
Symptoms and Signs present Controlled (%) I 2 J 4 I 0 5 5 I 0 0 I 5 4 2 4
)
9 ##
6 3 2 7 8 8 9 9 160 80 600 1305 50 300 160 t4150
180200
240r00
66100
45100
30100
72275
200200
102200
6024
9.112.8
12.70.4
37.83.5
302.7
12.25.3
I4.9
18.75.9
I2.2
57 Uncontrolled (%) Palpitation Tremor Irritable Hyperhidrosis/excessive sweating Weakness Exophthalmos 75 83.3 58.3 100 66 83.3 0 16.7 8.3 t6.7 0 83.3Table
3
shows several parametersof thyroid
function
at
delivery
of
the neonates(umbilical
cord blood)
andtheir
mother's
(TRAB)
as well
as
data
on PTU
administered
to
the
mothers
(total
dose, dose
score, meandaily
dose,duration
of
administration,
andtime
i.e.
months
of
gestation
during
which
PTU
withdrew).
The
lowest
total
dose
of PTU
was
60tablets
(50
mg/tablet)
and
the
highest
was
1305 tablets.The lowest
daily
doseof
PTU was
50mg
and the highest was 300mg.
The longestadministration
of
PTU
was 240 days and the shortestwas
14 days.The neonatal
TSH
levels
lessthan
20ulU/ml
(normal
<
20 uIU/mL) were found
in
ll
(91.7%)
neonates,one (8.3%)
neonate
have TSH levels more than
20uIU/mL.
Fetal
heart beat andrespiratory
rate wasfound
within
normal
limit,
ranged
from
the lowest
120
beat
perminute
to
the highest
148 beat
per minute.
All
the neonates hadnormal Apgar
Score.The lowest mother's
TRAB
levels
at
delivery
werelYo
andthe highest
was 57Yo.Mother's TRAB
levels atdelivery
of
lessthan
l5%owere found
in
5 (41.7%)
#
PTU was givenat
the first
5
months, stopped and then readministered on the last month ofpregnancy##
PTU was givenat
thefirst
7
months, then stopped andreadministered in the last month of pregnancy nd : no data available
Table
4
shows
the
features
of
PTU's dose
score,number
of
patient and
neonates
TSH levels.
There was asignificant correlation
betweenPTU
dose scoreand
neonates
TSH levels
(r:0.668,
p=0.024)
asdepicted
in
figure
l.
Table 4. The Features of PTU's Score Dose, Number of Patient and Neonates TSH Levels
PTU dose score
N
Mean Neonates 'TSH5
133690
760
8
1449
lt0010
410lt
240 [image:3.595.84.319.92.413.2] [image:3.595.344.577.206.439.2]s
;1u*^"
" t,in"r' 6 I 10
[image:4.595.61.316.92.710.2] [image:4.595.338.568.95.333.2] [image:4.595.333.572.111.617.2]$lcrn Nconâlc's I'Sll
Figure
I. Relationship
Between PTU dose score and Mean Neonates'TSHMother's
TRAB
atdelivery
could influence
neonates'TSH levels. The higher mother's
TRAB
levels
thelower
the neonates'TSH
levels are (table 5).Table 5. Mother's TRAB at Delivery, andNeonates' TSH Levels
Mother's TRAB Neonates'TSH
Figure 2. Relationship Between Mother's
TMB
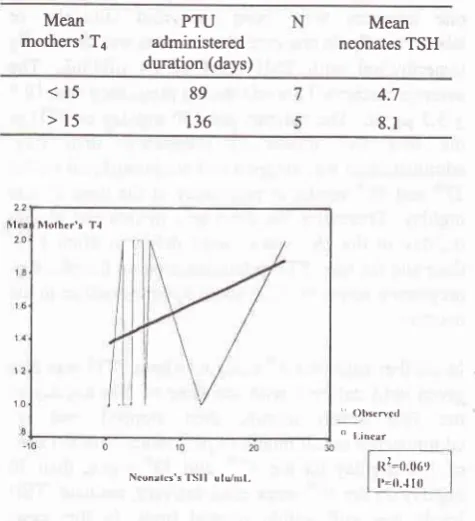
and Neonates'TSHTable 6. The Mothers' Ta, and Duration of PTU Administration
10
Ncoorlc's ti*tl uttj/r"t,
Mean
mothers'Ta administeredPTU duration (days)
Mean
neonates TSH
<15 >15
89
136
4.7
8.1 <15
>15
10.4
3.2
There was
no significant correlation
between mother'sTRAB
at delivery
with
neonates'
TSH.
(Pearsoncorrelation
t =
- 0.464,p:0.
150,figure
2).The
mothers'
Ta levelsduring
pregnancy and thepTU
administration duration
seemto
have aneffect on
theneonates'
TSH
levels.
The higher the mothers'
Talevels and
the
longer
the PTU
administration
tendedto
increase
the
neonates'
TSH
levels. There
wassignificant correlation
between themothers'
Ta levelsduring pregnancy
with
neonates
TSH
levels
(r
=
0.262\.The
mean
of
mothers'
Ta
levels during
treatment
in
this
studywas
14.4t
4.1
pgldL. During this
studywe
tried to
achieve
the
Talevel
-
15ug/dl,
sincein
our
previous study,
the
averageTa levels among normal
pregnantwomen was
15ug/dl.
Irlolhcr's T.l 22
12
'Otxrncrl " l-incar
0 10 20 s
Nconrtcs's'lSll ulu,/nrl,
Figure 3. Relationship Between Mother's Mean Ta Durtng Pregnancy and Mean Neonatal TSH
Higher
mothers'
Talevels
during
pregnancy
requiredlonger duration
of
PTU
administration and
increasedPTU
dosage score,
which
eventually
increased
the neonates'TSH
levels.20
10
[image:4.595.333.571.363.624.2]262
Mukhsin et alDISCUSSION
Previous studies
on
the
management
of
pregnancycomplicated
with
hyperthyroidism suggested
thatmothers'
thyroid
function during pregnancy
should bekept
in
pregnant euthyroid state
or
mild
hyper-thyroidism.a-'
This way, hyperthyroidism
causedby
PTU
overtreatment
in
neonates/infants
may
be prevented.8This
study showed
a significant
correlation
betweenPTU
dose score
with
neonates'
TSH
levels.
Theamount
of
PTU
dose during
pregnancy influenced
neonates'
TSH
levels. The
high
doseof
PTU
causedthe
increase
of
neonates
TSH
levels (table
4).However,
PTU
was
not the only
factors,
which
influence neonates'
TSH
levels.
Other
factors which
may influence
neonates'
TSH levels were
mothers"
TRAB.
However, in this study we failedto
demonstratesignificant correlation
betweenmothers'
TRAB
levelsat
delivery
and neonatesTSH.
In
this study,
from
12 examined patients,
all
exceptone
neonates
were born
euthyroid
clinically
or
laboratorically.
ln
one case, the neonates was chemicallyhyperthyroid
with
TSH level
of
24
pIU/mL.
The average mother's Talevels during
pregnancywas
19.5+
3.2 ltgldL.
The patients
got
150 mglday
of PTU
atthe
first five
month
of
pregnancy,
than
PTU
administration
was stopped and readministeredon
the37th
and
38thweeks
oilr"gnun.y
at
the
doseof
300mglday.
Thereafter
the
dose
was
maintained
at
200mg/day
in
the
39thweeks
until
delivery.
High
PTU
dose and the
long PTU administration
on the phaseof
pregnancy seems to
bring
abouthypothyroidism
to theneonate.
In
another case(the
4th case)to whom PTU
was
alsogiven
until
delivery
with
the
doseof
300 mg/day
in
the first
seven
month, then
stopped
and
re-administered
in
lastmonth
y with
the doseof
100 mglday on the
37
week, then
50mglday on the 39th week
u
,neonate' TSH
levels was
still within
normal
limit.
In this
case,perhaps
there
was an effect
of
extra
hypothalamic
TRH
andhigh
TRAB
levels.In
the
9s
casethe total PTU
dose
was high
(1100 tabs),the
daily
dosewas also
high
(275
mg),
and theperiod
of
PTU
administration'was also
long
(200days).
But
since
the TRAB
levels was
high,
theeàsuing
TSH level
was
not high.
It
seemsthat
high
Med J Indones
mothers' TRAB at delivery
(cases
1,2,5,6,9and
ll)
did not
determine
the
neonates'
thyroid
function
status, because
there
areother external factors
(PT[D
which
alsohave the influence on the
neonates' TSH.From
the
points
above,
routine
measurement
of
TRAB
is not recommended,but
still
useful
toperform
in
uncontrolled hyperthyroidism
with high dose
andlong
duration
of
PTU
administration.
In
that
case,if
mothers'
TRAB level
was high, the possibility
of
fetal/neonatal hypothyroidism
can
be
eliminated.Concomitant administration
of
PTU
was reported to
be able to prevent neonatal
hyperthyroidism.
Thefinal
result
of
neonates'
TSH
is
influenced
by both
PTU
and
mothers'
TRAB.
This
result
is in
agreementwith the
study
of
CheronRG et
alEwhich reported an
increase
in
neonates'TSH
levels
if
PTU
doseduring
pregnancy was
more than 400m{day.
Based on thatpoint,
theyperformed
further
study intendedto
determine thePTU
dose thatavoid
neonateshypothyroidism
by
giving
maximum
PTU
doseof
300
mglday.It
was reported thatfrom
ll
examined
patients,
all of
them delivered
euthyroid
neonates except
one
case (neonatal
TSH
>
20plU/ml),
who had PTU
in
the
first
8
months pregnancyof 100 - 150
mg/day
and 200 mg/dayin
thelast month
of
pregnancy.
Refetoff et
alEreported
thepresence
of
neonatal goitre
if
PTU
dose given
to
Graves' pregnancy mothers
was
more
than
200mglday. Momotani
et
ale
reported that there was
acorrelation between
PTU
doseduring pregrancy
andneonates'
TSH
levels. Those
studies
indicated
thatbeside
the amount
of
PTU dose during
pregnancy,there was also other factors influencing
neonates'TSH
level.
Mitsuda
et
ala proved
that
neonates'thyroid
function is influenced
by
both total
pTU
doseduring
pregnancy
and
mothers'
TRAB
levels
atdelivery.
This
study
yielded similar
conclusion
with
other studies stated above.In
real clinical
practice,
the
amount
of
pTU
administered
to
the pregnant Graves'
dependson
thelaboratory
thyroid function with monthly
monitoring
throughout pregnancy period.
To
the
uncontrolled
mother, PTU was given
in a
larger amount and
alonger
duration.
However,
considering
that the
total
dose
and duration
of
PTU
administration
influence
neonates'
TSH level,
it
is
advocatedthat
we
have to
be
aware and
careful
in
administering
high
dose andlong duration
ofPTU
in
pregnantGraves'
disease.receiving longer PTU
administration
ascompared
tothe
mothers
with
average
Ta
levels
<
15
pgldl,.
However, the
neonates'
TSH
level
of
both
groupswere
still within
normal limits. On further
analysis,however, there
were
significant
correlation
betweenmothers' Ta levels during
pregnancy
with
neonates'TSH
levels.
Similar result was also
reported
by
Momotani
et al.eNeonates'
TSH
levels are notonly
influenced by PTU
dose
during pregnancy
but
also
by
TRAB
level.Although there
were no
significant
correlation
between
Mothers'
TRAB with
neonates'
TSH in
this
study, there
is a
significant difference
in
neonates'TSH
level
in
different Mothers'
TRAB
group
atdelivery
(Wilcoxon
Rank-Sum Test).In
this
study
PTU administration
showed
a
positive
linear conelation
with
neonates'TSH level, but
on theother
hand
it
showed
a
negative/reverse correlation
with
mothers'
TRAB,
especially when
PTU
adminis-tation
wascontinued
upto delivery. Our result
is alsosimilar
to
that
obtained
by
Momotani
et
ale
andMatsuura
et
al.s They found that
pTU
and TRAB
influenced
the neonates'thyroid
function.
Folley
et al r0reported that
TRAB level
can
be
lowered Uy
ffU
administration
andit
was alsoproved in this
study.Tamaki et
al
rl
investigated
the
correlation
betweenneonates'
thyroid
dysfunction
and
neonates TSH
(umbilical
cord
blood).
They
reported
that
low
neonates'
TSH levels
and the presenceof
high
TRAB
could
predict
the
occrurence
of
neonates'
hyper-thyroidism.
Skuzaet
al
12reported
that
TRAB
level
of hyperthyroid patient
with
pregnancywill
be normalif
medication
isgiven during
pregnancy.TRAB
levelsare
going
to
increaseif
medication was
not given
atall.
Neonates'
TSH
level
in
thepatients
who
hadanti
thyroid
drugs wasreported to
bewithin
normal
limit.
On the other hand
neonates'
TSH level
of
patientswho
did
not
receive
any
medication
will
be
low,
concordance
with
hyperthyroidism
of
the
neonates.The result
of this
study is not
different from
the other studies mentioned above.The
meanbirthweight found
in
this
study was
3053grams, ranged
from
2500-3500 grams.
This result
issimilar
to
the result
reported
by
Mitsuda
et
ala whoreported
meanbirthweight of
3041
+
415
grams. Thelowest birthweight
in
this
study was 2500
g;
theneonate
was born
to
a
patient
with
uncontrolled
hyperthyroidism. Similar condition was
reported by
Mitsuda
et
al who
reported
that
patients with
uncontrolled hyperthyroidism,
treated or not,will
give
birth to
neonateswith lower birthweight
compared toneonates
of
patientswith
controlled hyperthyroidism.
In
this study,
no
congenital
anomalies
were
found,although
3(25%)
of
thepatients
sufferedfrom
hyper-thyroidism
in
early
pregnancy.
Neonatal
congenital anomalies as reportedby Momotani
etal
might
occurif
hyperthyroidism wasuncontolled
at early pregnancy,while Wing
et
alr3
did not find
any
longenital
anomalies
although
hyperthyroidism
occurredduring
embryogenesis
at
which
patient
was
treated with
antithyroid
agent.Milhama
reported the occunenceof
skin
aplasia
in
a
neonate
born
to a
hyperthyroid
mother
who got
methimazole therapy during
preg-nancy. Other studieshowever,
doubted thecorrelation
between
skin
aplasia andMethimazole
treatment sinceskin
aplasia can also occur
in
patients
with
otherthyroid dysfunction
without
methimazole treatment.It
is
concluded
that the conhol
of
hyperthyroidism
during
pregnancy
will
influence neonate
thyroid
function.
The
TSH level
of
neonatebom to
motherswith
hyperthyroidism
is
positively correlated with
PTU
administration,
while mothers'
TRAB
level
atdelivery is reversibly correlated
with
PTU administation.Optimal daily
dose
of
PTU that was not
resulted
in
neonate
hypothyroidism is less
than 300mg.
ThepTU
dose should be reducedto
100mglday
in
thelast four
weeks before
delivery
if
hyperthyroidism
persistsclinically
and laboratorically.Mean mothers' T4 level
of
14.4
+ a
p{dL
during
pregnancy
did not
causeany hypothyroidism
in
theneonates.
Meticulous monitoring of
pregnancy and thethyroid function
resultedin
safe outcomeof
pregnancy.Monthly
surveillance is considered to be adequate.The
measureof
the
neonates'
TSH level at birth
isadvocated
to
anticipate
thyroid
dysfunction
in
neonates
bom
to
hyperthyroid patients, as
well
asmothers'
TRAB
level in
pregnancyif
hyperthyroidism
is
uncontrolled
by high
dose
and long
period
administration of PTU.
REFERENCES
l.
Mazzaferri EL. Evaluation and management of common thyroid disorders in women. Am J Obstet Gynecol 1997;264
2.
3.
4.
5.
6.
10.
ll.
t2.
t3.
14.
7.
8.
Mukhsin et al
Roti E, Minelli R,
Salvi
R
Managementof
hyper-thyroidism and hypothyroidism in the pregnant woman. J Clin Endocrinol and Metab 1996 ;8l
:1679-82.Becks GP, Burrow GN. Thyroid disease and pregnancy. Med ClinNorth Am
I99l
; 75 :l2l-50.
Mitsuda
M,
Tamaki H, AminoN
et al. Risk factors fordevelopmental disorders
in
infants born to women withGraves' disease. Obstet Gynecol 1992;80 (3) : 359-64. Matsuura
N,
FujedaK, Iada Y,
et al.
TSH
receptor antibodies in mothers with graves disease and outcome in their offspring. Lancet 1998;I
: l4-7.Supran H, Suyono S, Supartondo. Free Ta, Tjuptake and
Free Thyroxin Index
of
normal healthy women in Dr.Cipto Mangunkusumo Hospital. National Congressof
the
Indonesian Intemal Medicine SocietyVI.
Jakarta 1984; 1050-60.Mestman
JG,
GoodwinMM,
MontoroMM.
Thyroid disordersof
pregnancy. Endocrinol MetabClin
NorthAm 1995
;24:41-71.
Cheron RG, Kaplan
MM,
Larsen PR, Selenkow HA,Crigler
JF.
Neonatalthyroid function after
propyl-thiouracil therapy for maternal Graves' disease. N Engl. JMed
l98l
;304.Med J Indones
Momotani
N,
Noh J,
OyanagiH,
IshikawaN, Ito
K.Antithyroid drugs therapy
for
Graves' disease during pregnancy. N Engl. J Med 1986 ; 315 : 24-8.Foley TP, White C, New
A.
Juvenile Graves' disease :usefulness
and
limitations
of
thyrotropin
receptor antibody determination. J Pediatric 1987 ;ll0
: 378-86. TamakiH,
AminoN,
TakeokaK,
etal.
Predictionof
later
developmentof
thyrotoxicosisor
fetal
hypo-thyroidism
from the
cord
serumthyroid
stimulating hormone level in neonates bom to mothers with Graves disease, J Pediatric 1989 ; I 15 : 318-21.Skuza
KA,
SillsIN,
SteneM,
Rapaport R. Predictionof
neonatal hyperthyroidism in infants born to mothers with Graves disease. J Pediatric 1996;128 :264-7.Wing DA, Millar LK, Koonings PP, et al. A Comparison
of propylthiouracil versus Methimazole in the heaftnent
ofhyperthyroidism in pregnancy. Am J Obstet Gynecol 1994 ; 170 :90-5.