Lung
cancer among young patients
in
Dharmais
Cancer
Center
Hospital,
Jakarta
(1994-1998)
Anwar Jusufx, Noorwati Sutandyo**, Sariasih Arumdatixx, Erlina Burhanx, Eddy Suratman*x, A. Mulawarman Jayusman x x
Abstrak
Kanker paru biasanya ditemukan pada usia trn dan usia pertengahan. Dari tahun 1994 sampai dengan tahun 1998, telah dirawat di RS Kanker Dharmais, 37 penderita yang berumur 40 tahun ke bawah, merupakan 5,9Vo dari seluruh penderita lunker paru yang dirawat selama masa tersebut. Penyakit ini ditemukan lebih banyak pada laki-laki (perbandingan kekerapan taki-taki dan perempuan adalah 3:l), kelompok umur 26-40 tahun. Sebagian terbesar pasien term.asuk stage IV (48,78ù, keluhan utama adalah sesak napas (58,IVo) dan nyei (32,5Vo). Kanker paru jenis karsinoma bukan sel keciL terbanyak ditemukan (91,98ù, karsinoma sel kecil sebanyak 2,7Vo dan pada 5,4Vo jenis histologis tidak dapat ditentukan. Pengobatan yang dipilih ialah pembedahan pada 9 lrasus, radioterapi pada 17 lcasus dan kemoterapi 5 kasus. Empat belas pasien (38Vo) meninggal di rumah sakit, sisanya tidak dapat diikuti. (Med
J
Indones 2001; 10:73-8)Abstract
Lung cancer is usually seen in patients of middle and old age. The disease is rarely seen in patients under 40 years. In Dharmais Cancer Center Hospital 37 patients of 40 years of age or younger were seen. The number was 5.9Vo of the total of lung cancer cases that was seen in this hospital in 1994
-
1998. The disease was more dominant among males (male to female ratio 3 :I),
age betvveen26-40years.Mostofthepatients were stagelV(45.78ù, chief complaints were dyspnea(58.IEo)and pain (32.5Vo). Nonsmall cell carcinoma was the moil frequent histologic type (91.9Vo), smaLl sell carcinoma was seen in 2.7Vo and in 5.4Vo the histologic type could not be determined. The treatment consisted of surgeryin
9 cases, radiotherapy in 17 cases and chemo-therapy in 5 cases. Fourteen patients (38Va) died in hospital, the rest were not followed further.(Med J Indones 2001; l0: 73-8)Keywords : Iung cancer, young age
As
in
other countriesin
the world,lung
cancer is increasingin Indonesia.
This
malignant disease is quitecommon among males of
the middle age and especially smokers, butis
not very frequent amongthose under
40 years
of
age. Previous studies havereported that
only
1 to
6
percents of patients with lung cancer are younger thanforty years
of
age.l-s Some have suggested that the clinical behavior oflung
cancerin
young patientsis
more aggressive comparedwith
bronchogenic cancer diagnosed inelder patients. r'2
MATERIAL
AND METHODS'We
reviewed all the cases
of
lung cancerin
patients of 40 years of age or younger who were hospitalizedin
Dharmais Cancer Center Hospitalfrom
January*)
Department of Respiratory Medicine, Faculty of Medicine, U niv e r s i ty of I ndone s ia/ P e r s ahab atan H o s p ital, J akar t a, Indonesia*x) Dharmais Cancer Çenter Hospital, Jalarta, Indonesia
1994
until
December 1998.The
Dharmais Cancer Center Hospitalin
Jakartais
oneof
the
teachinghospitals
for
the Facultyof
Medicine, University of Indonesia. There were 622 llung cancer patients seen during the periodof
1994-1998. They were managed according to the lung cancer protocol of the Faculty of Medicine, Universityof Indonesia.
The materials for this report were taken from the medical records of thehospital during the period. The inclusion criterias are:
-
Clinical and radiological diagnosis of lung cancer,with or without histological diagnosis
-
Age : 40 years or youngerThe items for analysis are :
.
sex, age.
chief complaints.
radiological abnormalitieso
histologic q?e according to WHO Classificationl98l
.
stage of disease accordingto
UICCI
AJCC 1997.
sites of metastasis.
treatment modalities.
outcome after treatment74
Jusuf etalRESULTS
During
1994-1998,37
lung
cancer patientsof 40
years or younger were seen. This number is 5.9Vo of 622fung cancer patients administered in the DharmaisHospital during the same period. There were 28 males (75,7Vo) and
9
females (24,3Vo) that makes male : female ratio approximately3:1.
Table 1 shows the distribution of the patients according to their age.Table
l.
The Distribution of Lung Cancer Patients Among Young Patients Accordingto
Ageat
DharmaisCancer Center Hospital 1994-1998
Age (years) I l-15 t6-20
2t-25 26-30 3 l-35 36-40 Not recorded
Cough
Cough and dyspnea
Dyspnea
Chest pain and dyspnea
Dyspnea, pain and nodule in chest wall
Severe dyspnea and nodule in the neck Chest pain
Discomfort in the back & chest pain Nodule in the neck
Bone pain
Headache
Stomach discomfort
Nausea
Unspecified
5
n
2 2 2I I
2.
I 4
2
1
I
2
13.5 29.8 5.4
5.4
5.4 2.7 2.7 5.4 2.7
r0.8
5.4 2.7 2.7 5.4
Med J Indones
Table 3 shows the chest X-ray abnormalities among the patients. The majority of them had a nodular mass
of
more than3
centimeters,with
or
without otherabnormalities
like
atelectasis, pleural
effusion,pneumothorax.
Table 3. Chest X-Ray Abnormalities of Lung Cancer in Young Patients, Dharmais Cancer Center Hospital, 1994-1998
Chest X-Ray Abnormality Vo
7o
> 3 cm Nodule
> 3 cm Nodule + Atelectasis > 3 cm Nodule + Pleural Effusion
> 3 cm Nodule + Atelectasis + Pleural Effusion > 3 cm Nodule + Pneumothorax + others
> 3 cm Nodule + others
< 3 cm Nodule + Pleural Efussion Atelectasis + Pleural Effusion Pleural Effusion
Others
Not recorded
9 2
I
2
I 2 3 2 5 8
2 24.3
5.4 2.7 5.4 2.7 5.4 8.1
5.4
13.5 21.6
5.4
1
6
11 l8 I
2.7
16.2
29.8
48.6
2.6
Total 100
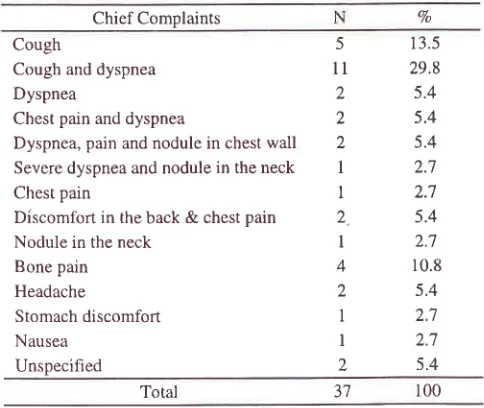
Table
2
shows the chief complaintsof
the patients.Dyspnea
alone
or in
combinationwith
othercomplaints was seen in 20 (54Vo) of patients, followed by pain alone or with
other
symptomsin
12 (32Vo),and cough alone or with dyspnea in 7 patients (l8,9Vo)
Table
2.
Chief Complaints of Lung Cancer Among Young Patients in Dharmais Cancer Center Hospital, 1994-1998Chief Complaints
Total
The histological diagnosis of the patients are shown in Table
4.
There wasonly
one caseof
small cell carcinoma (2,7Vo), 34 patients (97,9Vo) belonged tononsmall
cell
carcinoma andin
2
cases (5,4Va) Ihe histological diagnosis could not be determined.Table
4.
The Histological Diagnosis of Lung Cancer in Young Patients, Dharmais Cancer Center Hospital,1994-1998
Histological Diagnosis
100
.7 I
3t
ao N
7o
Squamous Carcinoma
Adenocarc'inoma
Large Cell Carcinoma
Adenosquamous Carcinoma Nonsmall Cell Carcinoma Small Cell Carcinoma Not Recorded
l0
18 2
3 I
1 2
27 48;7
5.4
8.1 2.7 2.7
5.4 Total
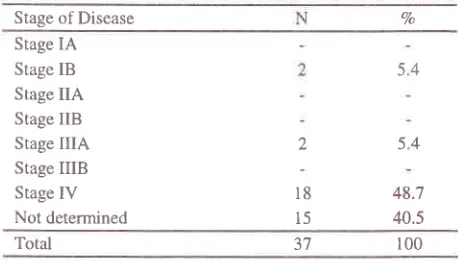
Table
5
shows the stageof
the disease among thepatients. Most
of
the patients (48,77o) were seen in stagefV;
5,4Vo were in stageIIIA.
In
4O,5Vo of casesthe
stageof disease
cannot be
determined. There were no stage IA, IIA,IIB
andIIIB
disease.100 37
[image:2.612.52.286.245.378.2] [image:2.612.48.290.511.715.2] [image:2.612.314.541.514.629.2]Table
5.
Stagingof
Lung Cancerin
Young Patients, Dharmais Cancer Center Hospit^\, 1994-1998Stage of Disease
[image:3.612.46.275.116.247.2]Brain Metastasis in Brain CT
Table 7. Bone Metastasis Shown in Bone Scanning in Lung Cancer Among Young Patients, Dharmais Cancer Center Hospital, 1994-1998
Metastasis in Bone Scanning
Vo
Stage IA Stage IB Stage IIA Stage IIB Stage IIIA Stage IIIB
Stage IV
Not determined
2
18 15
48.7 40.5
Table 6, 7 and 8 show the site of metastasis as shown by CT Scan of the brain, bone scanning and USG of
the abdomen. Brain CT Scanning was not performed
in 20
patients,in 9
patients there wasno
recordconceming this test. Among 8 patients who underwent
CT
of
the brain,4
patients show positive result ofbrain metastasis and in 4 patients, metastasis was not found.
Bone scanning showed metastasis
in
12 patients, in 4 patients the result was negative and8
patients therecord was not found. The test was not performed in
13 patients. Ultrasonography of the abdomen showed liver metastasis
in
5 patients,in
3 patients metastasiswere found in other organs. No metastasis were seen
in
the abdomenin
9
cases and the record was not found in 8 patients. The procedure was not performedin 72 patients.
Table
6. Brain
Metastasis Shown by Brain CT Scanning in Lung Cancer Among Young Patients, Dharmais Cancer Center Hospital ,1994-199832.4 10.8 35.2 21.6
Total r00
Table 8. Abdominal Metastasis Shown by Ultrasonography in
Lung Cancer Among Young Patients, Dharmais Cancer Center Hospital, 1994-1998
Seri Kemoterapi
Vo
54
54
Bone Metastasis Positive
Bone Metastasis Negative Not Performed
Not Recorded
t2
4
13 8 37
100 -tt
Total
Liver Metastasis Positive
Metastasis to Other Abdominal Organs No Abdominal Metastasis
Not Performed Not Recorded
Vo
100 37
Total
5 J 9
t2
8
1 3.5 8.1 24.3 32.4 21.7
Table 9 records the surgical treatment of the patients. Nine patients were treated with surgery. Six patients had lobectomy,
t
had superior vena cava by-pass surgery,2
patients had othertype
of
surgery. No record was availablein
4 patients andin
24 patients surgery was not performed.Table
9.
Surgeryin
Lung Cancer Among Young Patients, Dharmais Cancer Center Hospital, 1994-1998Type
ofSurgery
N
VoBrain Metastasis Positive Brain Metastasis Negative Not Performed
Not Recorded
Vo
N 4 4 20
9
10.8 10.8 54.1 24.3
lnbectomy
By-pass Surgery on Superior Vena Cava
Others
Not Performed Not Recorded
6
1 2 24
4
16.2 2.7 5.4 67.6
10.8 Total
[image:3.612.297.534.127.218.2] [image:3.612.302.535.548.652.2] [image:3.612.47.278.569.650.2]76
Jusuf etalEighteen patients were treated with radiotherapy. In 3
patients
the
records werenot
available andin
17patients
radiotherapywas
not
performed. Themajority of the inadiated patients had a total radiation
dose between 4000-6000 mcg (Table 10),
Table
10.
Total Doseof
Radiotherapyfor
Lung CancerAmong Young Patients Dharmais Cancer Center Hospital, 1994-1998
Radiation Dose
(cGy)
N < 20002000
-
3000 3000-
4000 4000-
50005000
-
6000 > 6000 Not PerformedNot Recorded
J
2
5
2 4
2
t7
2
8.1
5.4
13.5
5.4
10.8
5.4 45.9
5.4
CAP
II
*) Taxol-CarboplatinCAMP **)
Others
Not Administered
Not Recorded
1
1
I 2
5 )1
2.7
2.7
2.'7
5.4
13.5
73
Total 100
*) CAP II : Cyclophasphmide, doxorubicine, cisplatin
x*) CAMP: Cyclophasphamide, doxorubicine, methotrexate, procarbazine
After
treatment,14
patientsdied in
hospital, theremaining 23 patients were lost to follow up.
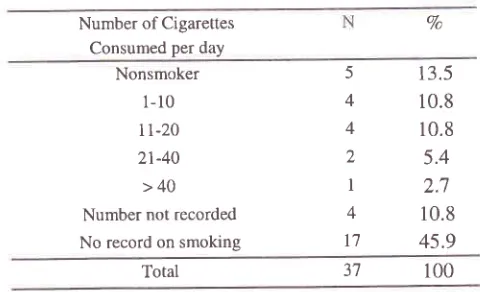
The smoking habit
of
the patients were recorded in only 20 patients. Five patients were nonsmokers, 15 rvvere smokers and there were no record concerningthis habit
in
17 cases. The daily cigarette consumption among the smokers were 1-10 cigarettes in 4 patients,Chemotherapy was administered
to
5
patients, no record was available in 2'7 patients, while in 5 patientschemotherapy was not indicated. Table 11 shows the
drug combinations that were used in the series
Table I
l.
Chemotherapyfor
Lung CancerIn
YoungPatients, Dharmais Cancer Center Hospital,
r994-1998
Drug Combination
Med J Indones
11-20 in 4 patients,
2l-40
cigarettes in 2 patients andmore than 60 cigarettes
in
1 patient. Noneof
them smoked 41-60 cigarettes per day and in 4 patients thedaily consumption was not recorded (Table 12).
Table
12.
Daily Consumption of Cigarettes in Young Patientswith
Lung Cancer Dharmais Cancer Center Hospital, 1994-1998Number of Cigarettes Consumed per day
13.5
10.8
10.8
5.4
2.7
10.8
45.9
Total
DISCUSSION
Our finding reveals 5.9Vo lung cancer among patients
of 40 years of age or younger. This figure was similar
to
those reported pievioristyby
several centers'1-5Other
had
higher
figuressuch
a
et.al.6 Earlier studY inPersah
that l5.2Vo of the lungcancer
cases
werein
young age group.Our
datacorroborate previous indication that adenocarcinoma are common among the young patients. Report from Persahabatan Hospital Jakarta gave
the figure
of 38.lVo of adenocarcinoma among the young patients'In
general, though squamous cell carcinoma has for many years been the most common histologic type, adenocarcinoma has been increasingin
incidence inrecent vears. a trend which has been demonstrated in
several repons.
Regardless
of
age, lung canceris
still
discovered assymptomatic disease as emphasized
by
the fact that94.6Vo of patients in our series were symptomatic. We
documented a
high
incidenceof dyspnea (29.8Vo)
asthe chief
complaint,and
combinationwith
othercomplaints were seen
in
58.lVo of patients. Chest pain aloneor
combinedwith
other complaint and coughwith or
without other complaints also. showed high incidence. These complaintsare,
as
reported byothers, are the symptoms of the late stage of disease.
Vo
r00
Nonsmoker
1-10
I 1-20 21-40
>40
Number not recorded
No record on smoking
5
4
4
2 I
4
t'l
100
3',1
[image:4.612.303.543.196.342.2]Kyriakous and Webberl0 reported weight loss as a chief complain, however
in
our study this complain was not recorded.Seventeen out
of
37 (67.6Vo) patients showed > 3 cm nodule in the chest X-rayfilm,
with or without other abnormalities such as atelectasis, pleural effusion, pneumothoraxand
others.Similar
condition was reportedby
De Caro et al showingthat2l
cases outof35 (6OVo) are considered as T2 and T3 cases.t
Metastasis
were
seenin
the
brain
(10.87o), bone (32.4Vo)and
liver
and
abdominal organs (2l.6Vo), although in 2l-24%o of patients no record was available. In accordance with the symptoms, most of our patients werein
the stageIY
(487o). The similar finding was reportedby
Green, who found out that 44of
out 48 (9l.7Vo) were first seen in stage fV.a The same finding was suggested by Bourke6 and GiriputroT which were 40-46Vo,and
66.6Vo respectively. These datas show that both public and professional awareness is limited since bronchogenic carcinomain
this
age group is uncofiImon. Young patients may not suspect serious illness. Moreover, physicians often may not suspect an underlying carcinoma despite persistent pulmonary symptoms, especiallyin
our setting where pulmonary tuberculosisis
still
the predominant causeof
many respiratory symptoms.Eighteen patients had radiotherapy,9 had surgery and 5 had chemotherapy as treatment. Radiotherapy was the most frequent modality chosen
for
the patients, while chemotherapy was administered onlyin
l4.5Vo of patients. This fact was controversial to the fact thatmost
of
the
caseswere
stage
IV, for
which chemotherapywas
more
indicated
while
the performance status allowed.The
reasonfor
thismaybe
due
to
financial
problem.
As
most
of Indonesians, most of the patients were not covered by insurance. They have to pay all the costs of diagnostic aswell
as the therapeutic procedures. Sincein
ourcountry
radiotherapycosts
less
expensive than chemotherapy, doctorsoften
haveto
choose this modality as palliative treatment, evenin
stage[V
cases, for example for bone pain, superior vena cava syndrome etc. Number
of
surgery performed in our study was relativelylow (6
lobectomy,1
bypass surgery for superior vena cava and 2 other equations). Mostof
patients were sincein
late state. This may explain why in 24 patients in this study, surgery was not performed. Since there were only 4 stageIB
andIIIA
patients, surgery were performedin
relativelylate stage patients as palliative treatment.
Cigarette smoking, is accepted as the important cause
of
lung
cancertt-tt
In
young
patie;ts
(95.2vo),however, many studies show different case. Giriputro
et al
showedthat
most young patientswith
lungcancer
or
95.27o werenon
smokers.T Greenet
al found 42Vo of never smokersin
theirstudy.a In
our series 13.5%of
our
cases were nonsmokers and 40.5Vowere
smokers,the
majority being
heavy smoker.In
spiteof
the lackof
data concerning this habitin
45.9Voof
the cases, the numberof
smokers are large enough to consider smoking as a risk factor. The high figure of smoking history was also reported in their study by Pemberton et al, Jubelier and Wilson, Bourke et al,and
Kyriakos and Webber which were87 Vo, 7 7 Vo, 8 I -9 \Va, and. 9 4. I Vo respectively. 2' 3'6' I 0
We found in our study 48.7Vo cases, the stage can not be determined. This high figure might due to the fact that many of our patients or the family decided to go home much early even before the diagnostic procedures were performed. Financial problem and
feeling
of hopeless are most likely to be the cause.This
early discharge by the patients or family wishes is perhaps responsible as wellfor
incomplete datain
metastasis and chemotherapy record.This study and others demonstrated that lung cancer is no longer a disease of old male patients with smoking histories
but
also
a
diseasesof
young
people, regardlessof
age and sex. Diagnostic test should be performed earlyto
exclude the possibilityof
lung cancer among young patientswho
have persistent symptomof
pulmonary diseases.It
is also important to look for other factors in our population such as air pollution, nutrition, education, social economic status and genetic abnormalities, which could be related to the early development and severityof
lung cancer. Further research, of course, need to be done.'']
78
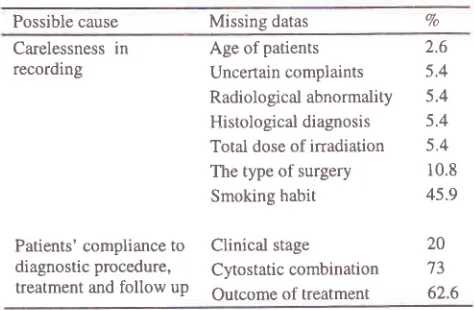
Jusuf et alTable 13. Missing datas and the possible cause
CONCLUSIONS
.
Lung
cancerin
young
patients (40 years oryounger) were seen in 5.97o of the total number of
case of lung cancer
in
Dharmais Cancer CenterHospital during the period 1994-1998
o
Mostof
lung cancer among young patients wereseen as advanced disease (stage
IV)
.
Adenocarcinoma was the most frequent histologictype in our study
.
Hôspital recording and reporting system need to tiedeveloped to ensure the complete and proper datas
are available for research
o
Both community and professional should be moreaware of lung cancer among young people, so the
disease could be found in the early stage
Acknowledgement
The authors wish
to
thankMrs.
Sunarti, S.Sos andMs.
Anggriani,SKM
for
typing and preparing thismanuscript
Med J Indones
REFERENCES
1. De Caro L, Berfreld JR. Lung Cancer in Young Persons. J Thorac Cardiovase Surg 1982 ;83 :372-6
Pemberton JH, Nagorney DM, Gilmore JC, Taylor WF,
Bernatz PE. Bronchogenic carcinoma in Patients Younger than 40 years. Annual of Thoracic Surgery 1983 ; 36 :
509-15
Jubelirer SJ, Wilson RA. Lung Cancer
in
PatientsYounger than 40 years of Age. Cancer l99l ;67 : 1436-8
Green LS, Fortoul TI, Panciano G, Robles C, Rivero O.
Bronchogenic Cancer
in
Patients under 40 years old.Chest 1993 ; 104: 1471-81
Rocha MP, Fraire AE, Guntupalli KK, Greenberg SD.
Lung Cancer in the young. Cancer-Detect-Prev 1994 ; 18 : 349-s5
Bourke W, Milstein D, Giura R, Donghi M, Luisetti M, Rubbin AHE, Smith LI. Lung Cancer in Young Adults.
Chest 1992 ;102:1723-9
Giriputro S, Rasmin
M,
JusufA.
Kanker paru padagolongan usia muda di RS Persahabatan Jakarta. Jumal Respirologi Indonesia 1988; 8 : 13-8.
El Torkey M, El Zeky F, Hall IC. Significant Changes in
the Distribution
of
Histologic Typesof
Lung Cancer.Cancer 1990 ;65:2361-7
Valaitis J, Warren S, Gamble D. Increasing Incidence of Adenocarcinoma of the Lung Cancer. Cancer
l98l
; 47 : 1042-6Possible cause Missing datas Vo Carelessness in
recording
Patients' compliance to diagnostic procedure,
treatment and follow up
Age of patients
Uncertain complaints Radiological abnormality Histological diagnosis
Total dose of irradiation The type of surgery
Smoking habit
Clinical stage
Cytostatic combination Outcome of treatment
2.6 5.4
5.4
5.4
5.4
10.8 45.9
20 73 62.6
2
5
6
7
8
9
10. Kyriakos M, Webber B, Path FF. J Thorac Cardiovasc Surg 1974 ;67 :634-47
I
1.
Jusuf A, Suryanto E, Hudoyo A. The relationship betweenSmoking and Lung Cancer
in
Persahabatan Hospital,Jakarta
in :
Cancerin
Asia and Pacific. IndonesianCancer Foundation, Jakarta 1998 : 655-62
12. Samet JM, Wiggins
CL,
Humble CG, Rathak DR.Cigarette smoking and Lung Cancer in Mexico. AM Rev
Respir Dis 1998 ; 137 :
lll0-3
13. Ernster VL. Trendy Smoking Cancer Risk and Cigarettes
Promotion. Cancer 1988 ;62: l7O2-12
14. Breslow L, Cumberland WG. Progress and Objectives in
Cancer Control. JAMA 1988 ; 259 : 16904
15. Trichopoulos D, Kalandidi A, Sparros L, Mac Mahon B. Lung Cancer and Passive Smoking. Int J Cancer 1998 ;
[image:6.612.47.284.100.255.2]