-\
Vol 10, No l, Jamnry
-
March 2001 Immunohistopathological featues of prurigo H ebraThe immunohistopathological features of
prurigo
Hebra
Siti Aisah
Boediardja,x Achmad
Tjarta,x*
SantosoComain,**
Unandar
Budimulja,*
Adhi Djuanda,
xEndang.S.Roostini,*x
Meny
Hartati**
Abstrak
Sampai saat ini meknnisme
pruigo Hebra (PH) belum diketahui
secara pasti. Namun, berdasarkan adanya riwayat dalam keluargayang menderita penyakit serupa serta riwayat alergi terhadap gigitan nyamuk, besar kemungkinan mekanismenya merupaknn mekanisme hipersensitivitas. Penelitian
ini
bertujuan mengevaluasi gambaran imunohistopatologik PH khususnya sebukan sel inflamasi umum dan spesifik pada lesi awal dan lesi kronik. Penelitian dilakuktn terhadap 50 spesimen yang berasal dari biopsi lesiawaL dan 50 lesi lanjut. Setelah diproses sediaan tersebut diwamaknn dengan HE dan imunoperoksidase (lP) menggunakan antibodi monoklonal terhadap sel inJlamasi spesifik, yaitu sel B, sel T, sel T-helper CD4+(sel CD4+), sel T-supresor CD8+ (sel CD9+), sel ktngerhans, dan sel penyaji antigen (SPA) yang mengel<spresikan HI,A-DR (SPA/HLA-DR). Pewamaan
HE pada
lesi
lanjut menunjukkan sebukan sel radang campuran yang lebih banyak dibandingkan dengan lesi awal. Pada lesi awaL jumlah sebukcn sel poLimorfonuklear hanya sedikit, sedangkan eosinofil sangat banyak tetapisel
mas tidak
ditemukm.Hasil
pewarnaan IP memperlihatkan sebukan sel radang terdiri atas sel T: CD4+ dan sel CD8+, sel lnngerhans, dan SPA/HLA-DR jumlahnya pada Iesi lanjut lebih banyak daripada lesi awal, tetapi perbedaanini
tidak bermakna (p>0.05), kecuali CD4+. Pada sediaan lesi awal maupun Lesi lanjut sebukan selCD4+
Lebih banyakjumlahnya daripada sel CD8+ dengan ratio 3:l dan 2:1. Sel B yang normalnya tidak dijumpaidi
kulit, ditemukan dalam jumlah sedikit, serta tidak berhubungan dengan banyaknya eosinofil dan sel T. JumLah seL I'angerhans (SL)di
epidermis pada lesi Lanjut Lebih banyak daipada awal. Secara statistik ditemukan korelasi kuat (0.39) antarajumlah sel T dan SPNHLADR. berdasarkan hal tersebut dapat disimpulkan bahwa pasien prurtgo selalu terpajan faktor ekstrinsik. Analsis menunjukkan pada pPH yang memiliki
HIA,-AI)
atau HLA-Al0-spIit, makin berat penyakitnya makin banyak jumlah sebukan eosinofil (X2for
trend <0.05). SeI radang yang didapatknn pada penelitian ini memperLihatkan bahwa mekanisme terjadinya prurigoHebra sesuai reaksi hipersensitivitas campuran tipe I dan tipe IV. (Med J Indones 2001;
l0:l-15)
Abstract
Until now the pathoLogic mechanisms of prurigo Hebra (PH)
is
still understood. Earlier study the genetic inheritance of PH showed the multifactorial pattern. Considering the genetic inheritance and the existence of allergic reaction to insects bitein all
patients, might be the mechanisms followed hypersensitivity reactions. The purpose of this study is to evaluate the general and specific local inflammatory featuresof
early and late lesions of prurigo Hebra (PH). Fifty biopsy specimens of early and Late lesions of prurigoHebra patients were processed
with
haematoxylin-eosin(HE)
and immunoperoryde(lP)
staining using monoclonaL antibodies against specific inflammatory ceLLs nameLy B cells, T ceLls, helper T (CD4+) cells, supressor T (CD8+) cells, Langerhans celLs, and antiqen presenting cells (APC) that expressed HIA,-DR antigen. HE-staineil specimens: In early lesions, PMN cells werefew,
while eosinophils were present in great quantity and independent of mast cells and plasma cells; this feature was similar to that of insect bite reaction. IP-stained specimens:In
Inte lesions, the amounts of lympho-histiocytic infiltration consisting of T cells, CD8+ cells, H['A-DR-expressing APCs were greater than those of early lesions, althoughit
was not statistically significant. An exception wasfor
the CD4+ celLs, whose number in early lesions was significantly higher. The ratio of CD4+ to CD8+ in early lesions was higher than in late lesions (3/1: 2/l). This suggested that CD4+ cells were predominant. B cells, which were normally absent, appeared in small quantity in both early and late Lesions. The presence of B cells was not statistically correlated with T cells or eosinophils. The number of Langerhans cells in late lesions was higher than in early lesions. There was a strong correlation (r=0.39) betyveenT cells and HLA-DR-expressing antigen-presenting cells (APCs|HLA-DR). Those cells foundin
greatqunntity
suggested that PH patients usually exPose to extrinsic factors. In some cases with severe condition, the presence of eosinophils was more profound and was statistically significant.It
is conclude that immunohistopathological mechanisms of PHfollow
the mixed types (one andIV)
hypersensitivity reaction. (Med J Indones 2001; l0:1-15)Keywords: Prurigo Hebra, eosinophils, CD4+cells, mixed (I and IV) types of hypersensitivity.
*
Department of Dermato-venereology, Faculty of Medicine, University of Indonesia, Jakarta, Indonesia** Department of Pathology, Faculty of Medicine, University of
Indonesia
Prurigo Hebra is
achronic,
inflammatory
skin
diseaseI
Boediardja et al
disease
in
Vienna,
Austria. Its clinical
manifestations,rtchrng,
prurigo
papules, hyperpigmentation
andhyperkeratotic
skin,
greatly inhibit
patient's rlcrivity
and
aesthetic
p.erformance.l-6In
Inclonesia. prurigo
Hebra
cases
are
very
common. even
in a
referralhospital
like
Dr.
Cipto
Mau_rnnkusumo
GeneralHospital,
Jakarta.T 8The diagnosis
is not especially
difficult;
the disease iseasily
recognized
by its
specific
locations:
theextensor surface
of
lower
and upper extremities, face,buttocks and abdomen. Patients
generally complain
of
severe
itching.
The
manifestation
is limited
to
theskin,
appearing as polymorphic lesions
such
aserythema and dome-shaped
papules
with tiny
vesicleon its top. The
vesicles are
immediately
ruptured
byscratching
then
the
lesions become eroded
andexcoriated.r-6
Agents
of
hypersensitivity, such
as bedbugs, ants, mosquitoes. and certain drugs and foods,
as
well
as bad hygiene and
poor
nutrition,
areclaimed as the factors that trigger
or
influence
thedevelopment
of the
disease. e'loUntil
now, the mechanism of the
disease hasnot
beenfully
understood.
Occampo
1975,
Australian,
fourld
that the histopathological
specimens stainedwith HE
of early infantile prurigo
Hebra lesions showed
acuteinflammatory
infiltration
consisting of
polymorpho-nuclearcells and eosinophils. This
feature was similarto
that
of insect bite
reaction.'o
On the other
hand,Boediardja,
1987, Indonesian,
found that the
histo-pathological examination
on
159
HE
biopsy
specimensof
chronic prurigo Hebra
lesions
showedchronic inflammatory
infiltration
predominated
bylymphocytes, histiocytes
and eosinophils.This
finding
could
not
be
concluded
wether
the
underlying
mechanism was
a
general
or
specific
immunological
reaction, even though the
presence
of
eosinophilssuggested
immediate (type
I)
hypersensitivity
reaction.Boediardja,
1987, alsofound
an increaseof
total IgE
levels
in
50Vo
of
159
patients.n
O""u-po,
1915,confirmed
the hypersensitivity to insect bite in prurigoHebra,
his
study
on
100infantile prurigo
casesfound
positive
prick
test reactionto insect allergens.l0
The airn of
this study
is to
identify
the
local
immunologic
mechanism
of
the
disease
using
histopathological examination
with
HE
and
IP stainings.Med J lndones
I\,IETHODS
A
descriptive-analytic study was designed
to compare
the intlammatory cellsinfiltration in
the early(A)
andlate (chronic) lesions
(B). Fifty
casesof
prurigo Hebra
were included in the study. Skin biopsy was
takenfrom
an early lesion (red papulethat appeared
within
48
hours)
and
a
late
lesion
(old
papule
onliyperpigmented area
or hyperkeratotic lesions)
oneirch subject.
All
skin biopsies
were sliced wrth a
microtome
to
3-4 pm thickness; 3 or
more slices
of
the
same lesion(A
or
B)
were prepared
on
an objective glass (slide).Fifty
slides
of
each
early and late
lesions
were
therrstained
with HE
and
IP
using
monoclonal
antibodies a-{ainstT
cells, T-helper (CD4+) cells,
T-supressor/cytotoxic
(CDS+)
cells, B cells,
Langerhans
cellsand antigen-presenting
cells which
expressedthe
q.-and
B-chain
of
HLA-DR
(APCs/HLA-DRu
or'APCs/HLA-DnB).
To identify
specific
cells
(T-cells,
CD4+
cells,
CDtj+
cells,
B
cells,
Langerhans
cells, and APCs),
themonoclonal antibodies
UCHL-
I(CD45RO),
antihuuranCD4+ cells,
antihuman
CD8+ cells, CD20
or
L26.protein
S-100. antihllman
HLA-DRa
and antilrunrarr
HLA-DRP
or CR3/213,
respectively were nsed.
Thesemonoclonal antibodies
were
made
by
Dako
Corporation.
The
substratefbr all lP
staining was
3'3'diaminoben-zidine (DAB),
')-r+except
fbr
epidermal
Langerhar.rscells (LCs)
was 3'amino-9'aethylcarbazone (AEC;. r5'r('From skin biopsy
100 wereeligible for
the study, eachlesion had
one HE-stained
slitle
and
seven
IP-stained sfides, onefor
eachtype
of
cells. The positive
control
specimens
were
taken
tl'om
the
tonsil/
appendix tissue
while
negative
(Lrnstained)contlol
specimens werefiom
the sarne lesions.Vol 10, No
I,
Janrcry-
March 2001average (mean
t
standard deviation) number of
infiltrating
cells was
calculated
from
the
total
number/l cm2
of
that particular
cell. The
averagenumber
of a particular
cell
in
the central part
of the
lesions
wasthe
total numberll cmz of
that
cells
in
three parts
of
each
slice divided by six (3x 2 slices).
Mann-Whitney
statistical method
(U
tesQ was used to comparethe
quantity of inflammatory cell infiltration
at the central part and the edgeofearly
and late lesions.The
immunogenetic
factors
of
human
leukocyte
antigen
(HLA)
were performed
in
4l
casesby using
HlA-class
I
Asian
dry
traylot
#
1A
based
onmicrolymphocytotoxic
reaction.RESULTS
The
histopathological
characteristics of
Ifi
staining
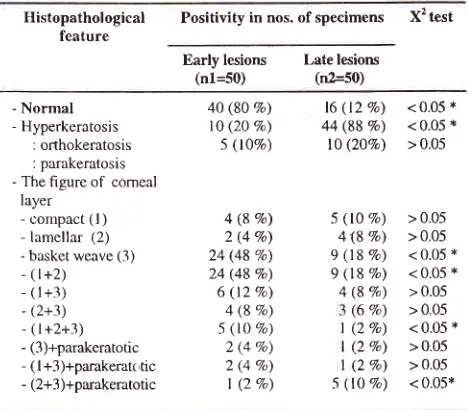
Histopathological examinations
revealed
thecharacteristics
of
corneal
layer
in
early and late
lesions and are presented in Table1.
Normal
corneallayer was seen
in
80% cases
of
early lesions
and l2%oof
late
lesions.
On the
contrary,
orthokeratosis
wasnoted
in
887o
cases oflate
lesions and
appearedin
only
2OVo casesof
early
lesions.
The
basket
weaveconfiguration
of
corneal layer was pronounced
in
early lesions
(48Vo).
All
findings were
statistically
significant (p<0.05).
Table t. The characteristics ofthe comeal layer ofearly and late prurigo Hebra lesions
Histopathological feature
Positivity in nos. of specimens X2 test
I mmuno hi s t op a tho lo g ic al fe atue s of p ruri go H e b ra
The characteristics
of
the epidermal layers (including
granulosum, spinosum and basal layers)
of early
andlate
lesionsof
prurigo Hebra
are presented in table 2.The thickening
of
the
granulosum
layer was more
frequently found
in the early
lesions than
in
the
latelesions;
the difference was
significant (p<0.05).
Onthe other
hand,the
thinning of
granulosum
layer
wasobserved
more frequently
in
the late
cases
than
in
early ones, statistically significant at p<0.05. Acanthosis,irregular papillomatosis,
andhyperpigmentation of
the basallayer were
morefrequently found
in
late
lesions thanin early
lesions,statistically significant
at p<0.05.In the
central
part
of
specimenspatchy
perivascular
infiltrates
were seen especially
in the
upper
andlower
dermis.
Lymphocytes, histiocytes and
eosinophils
were
abundant,
while
PMNs
were
few.
Forty-nine
(987o) specimens
of
early
lesions showed
vaso-dilatation and vascular
oedema
with protrusion
of
endothelial
cells
into the lumen.
Seven
(l4Vo)
specimensof
late lesions
showedcollagen thickening
and
a relative decreaseof fibrocytes.
Table 2. Epidermal characteristics of early and late prurigo Hebra lesions
Epidermal
layer
Positivity in nos. ofspecimens
X 2 testcharacteristics
Early
lesions
late lesions(nl=JQ)
(n2=50)- Normal - Hyperkeratosis
: orthokeratosis
: parakeratosis - The figure of comeal
layer - compact (l )
- lamellar (2)
- basket weave (3) - (l+2)
- (l+3) - (2+3) - (l+2+3) - (3)+parakeratotic
- (l+3)+parakerat( tic - (2+3)+parakeratotic
Early lesions
(n1=50)
Late lesions
(n2=s0)
Granulosum layer
Normal Abnormal: - thickening - thinning Spinosum layer Normal Abnormal: - sponglosrs
- acanthosis
- spongrosrs+ acanthosis
Basal layer
Normal Abnormal:
- papillomatosis - psoriasiform - irregular
papillomatosis
Basal pigmentation Normal Abnormal
12 (24Vo)
26 (52Vo)
4 (8Eo)
40 (80 Eo) t0 (20 Ea) 5 (tOVo)
4 (8 Vo) 2 (4 Vo) 24 (48 Vo) 24 (48 Eo) 6 (12 Vo) 4 (8 Vo) 5 (lO Vo) 2 (4 Vo) 2 (4 Vo) I (2 Vo)
16
(127o)
<0.05 * 44 (88Vo)
< 0.05 * l0 (207a) > 0.05L6 (32V.) 3l (62Vo)
3 (6Vo)
26 (52Vo) 13 (26Vo) 'l (147a)
4 (8Vo)
32 (64Vo) 12 (24 Vo) 5 (ljVo)
| (2Vo)
38 (76Vo) 12 (24Vo)
2O (40Vo) t5 (30Eo) 15 (3OVo)
8 (l6Vo)
>
0.05 < 0.05 *<
0.05 *0.05 *
0.05
0.05 * 0.05
lO
(20Vo)
< 0.05i
l7 (14Vo) > 0.053
(6Vo)
> 0.05 20(4OVo)
< 0.05 *23 (46Vo)
27
(54Vo)
< 0.05 * 5 (10 Vo)4\8 Vo) 9 (18 Va) 9 (18 Vo) 4 (8 Vo) (6 Eo) (2 Eo) (2 Eo) (2 Vo)
> 0.05 > 0.05 < 0.05 * < 0.05 * > 0.05 >005 < 0.05 x > 0.05 > 0.05 < 0.05x
Note
:
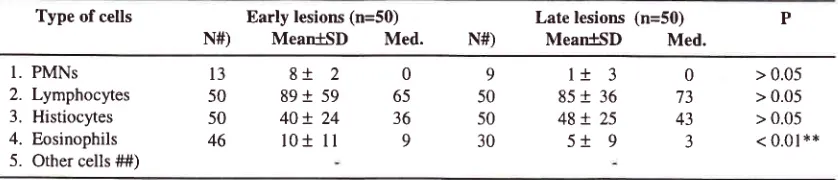
significant difference at p<0.05Table 3
displays
the average numbersof
non-specific
inflammatory cells found
in
the central part
of the
specimens.PMNs infiltrates were
seen
in
13
of
50 Note : The significant difference at p<0.05 [image:3.612.305.545.391.649.2] [image:3.612.47.281.506.711.2]Boediardja et aI
early-lesion and
9 of
50
late-lesion
specimens. Thenumber
of PMNs in
early lesions was greater
than in
the late
ones. Lymphocytes
and histiocytes
were abundant,their number
in
the late lesions were greater thanin
the early ones,statistically
thesefindings
werenot
significant (p>0.05).
[n
the
early
lesions,eosinophils
were morepronounced; their
number wasgreater
than that
in
the late lesions
with a
highly
significant difference (p<0.01).
In
5
early-lesion
specimens,the number
of
eosinophils found were
50-100cells/l
cm2; theyinfiltrated
uncommonly even in
the
interstitial
part of the
subdermis,
giving
theappearance
of
flame
figure.
Mast cells, basophils,
andplasma
cells
were not seen.Table 3. The non-specihc inflammatory cells in the central part of the lesions
Med J Indones
The
immunohistopathological findings
T, CD4+, CD8+,
andB
cellsThe
absolute numbersof
T,
CD4+ cells, CD8+
cells,and
B
cells
in
the central part of the
early
and
late lesions are showedin Table
4.
Statistical distribution
of
T, CD4+ cells
,
CD8+
cells,
B
cells, lymphocytes
and histiocytes
did not follow the
normal
curve,except for
the CD4+ cells
in
the
early
lesions,therefore
Mann
Whitney test
(U
test) was
used
for
analysis.The
absolutenumbers
of
T
and
CD4+
cellsin
the early lesionswere greater than
in
the late
ones,but
not
statistically
significant
(p>0.05). The
absoluteType of cells Early lesions (n=50)
N#) MeantSD
Med.Late lesions
(n=50)
PN#)
MeaniSD
Med.l.
PMNs2.
Lymphocytes3.
Histiocytes4.
Eosinophils5.
Other cells ##)8+ 2
089t
59
6540+
24
36l0+
ll
99
l+
350
85+
3650
48+
2530
5+
9l3
50 50 46 0 73 43 3> 0.05
> 0.05
> 0.05
< 0.01
**
Note:
N#) =nurn6st of positive specimens, Mean = average,'SD= standard deviation, Med. = median,##) Mast cells, basophils, plasma cells were not found.
Significant different at p <
0.05, **
highly signihcant difference at p< 0.01Table
4.
The absolute numbers of T,CD4+ cells ,CD8+ cells, and B cells in the central part of prurigo Hebra lesionsThe absolute number of
cells
/l
cm2Early lesions (n1=59; Mean
t SD
MedianLate lesions (n2=50) Mean
t SD
MedianU test
1. T cells Lymphocyes Histiocytes+lymphocytes
2. CD4+ cells Lymphocytes Hi sti ocytes+lymphocytes
3. CD8+ cells Lymphocytes Histiocytes+lymphocytes
4. B cells Lymphocytes Hi stiocytes+lymphocytes
5. Ratio CD4+ cells: CD8+ cells
72.68 X44.22
55.06
t
28.38 91.94 + 4t .4341.40 + 35.44
60.18+31.01
97.79
t
45.3820.84
t
15.86 68.52t35.32
105.68 + 48.884.57
+
3.83 93.73 + 43.62 37.00r 57.00
2.90
I
1.8957.24 + 33.59 51.66 + 25.96 87.30 + 41.78
27.70 + 18.00 62.04 + 27.02 102.94 + 41.7',1 20.00
I
16.00 67.96 + 28.O4108.98 + 46.56
5.76
r
3.00 '73.43!33.88
119.81!43.52I
.847+ l.l8
58.50 53.50 86.50 28.00 60.00 94.00 17.50 70.50 108.00 4.00 92.00 130.003. t0
5t.50 50.55 86.50 22.29 65.50 99.00 17.00 70.50 107.50
5.7 | 74.00 t24.00
1.58
p > 0.05 p > 0.05 p > 0.05
p > 0.05
p > 0.05 p > 0.05
p > 0.05
p > 0.05
p > 0.05
p > 0.05
p > 0.05
p > 0.05
p < 0.05*
[image:4.612.52.471.297.387.2] [image:4.612.51.478.468.699.2]Vol 10, No
I,
Jawnry-
March 2001number
of CD8+
cells
in
the early lesions was similarto the late ones.
No
specific
arrangementdistributions
of
CD4+ and CD8+ cells were
seen
in
the
patchyinfiltrates.
The
CD4+: CD8+ ratio in
the early lesionswas higher than
that
in
late
lesions,
statistically
significant
at p<0.05. Data
showed
that CD4+
cellswere predominant
both
in
the early
and
late
lesions.Surprisingly,
B
cells
were
few
in
number;
their
number
in
the late lesions was
greater
than
that
in
early lesions, and
were not
statistically
significant
(p>0.05). The
absolutenumbers
of
lymphocytes
andhistiocytes
in
the early lesions were greater than thosein
late lesions, but not statisticallysignificant
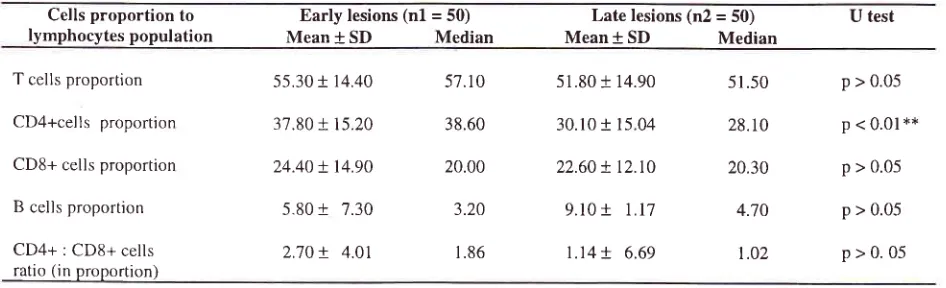
(p > 0.05).The
proportion
meaning
the
percentage
of
theabsolute
number
of
T,
CD4+, CD8+
cells
and
Bcells
in
the central
part
of
the
specimensto
the total
number
of
lymphoèytes
in
each
slides/l
cm2. The
proportions were
presented
in
Table 5. The
CD4+
cell
proportion
in
the early
lesions
was
statistically
Immunohistopathological featues of prurigo Hebra
greater than that
in the
late Iesions (p<0.01).
Theproportion of T
cells
wasfound in
great number
(51-57Vo),
while
B
cellsjust
in
a
few
(3-5Vo). Other cells showeddifference
betweenearly and
late lesions,
but
were
not
statistically significant.
In
spite
of
statistical
calculations, the CD4+
cells
seemedto
predominate (over CD8+ cells) in both the early and late lesions.Langerhans and
HlA-DR-expressing
APCs
The
absolutenumbers
of
LCs/l
crrf
are presentedin
Table
6.
The absolute
number
of
epidermal LCs
thatstained
with
protein 5-100
in the
late lesions
wasstatistically
greater thanthat
in
early lesions (p=0.05).
LCs expressed
the
HLA-DRcI and
B
monoclonal
antibody. The
numbers
of
both
LCs/HLA-DRa
andLCs/HLA-DRp
in
late
lesions were also
greater thanthat
in
early lesions
and
were
statistically
significant
(p=0.01).Table 5. T, CD4+, CD8+, B cells proportion at central part
of
early and late lesions of prurigo HebraCells proportion to
lyrnphocytes population Mean + SDEarly lesions
(nl
= Median50) Late lesions (n2 =50)
Mean + SD Median
U test
T cells proportion
CD4+cells proportion
CD8+ cells proportion
B cells proportion
CD4+ : CDS+ cells ratio (in proportion)
55.30 + 14.40
37.80
r
15.2024.40
t
14.905.80
t
7.302.70
+
4.0157.1 0
38.60
20.00
3.20
1.86
51.80
i 14.90
51.5028.1 0
20.30
4.70
1.02
p > 0.05
p < 0.01't*
p > 0.05
p > 0.05
p>0.05
30.10
t
15.0422.60
!
t2.t0
9.10
+
1.171.14+
6.69Note: SD = standard deviation, significant difference
at p
<0.05, highly significant difference at p<0.01Table 6. The numbers of epidermal Langerhans cells in the central part of the lesions
Epidermal Langerhans
Cells Mean + Early
SD
lesions (n=50)Median Mean + Late lesions (n=50)SD
Median U testLCs /S- 100
LCs/HLA-DRa
LCs/HLA-DRp
3.58
+ 2.11
3.96!
2.444.75
+
2.544.00
4.00
5.00
4.50
r
5.30
r
6.t4
!
2.91
2.69 3.03
5.00
6.00 6.50
P = 0.05* p = 0.01** P = 0.01**
[image:5.612.47.520.372.516.2] [image:5.612.46.517.581.666.2]Boediardja et al
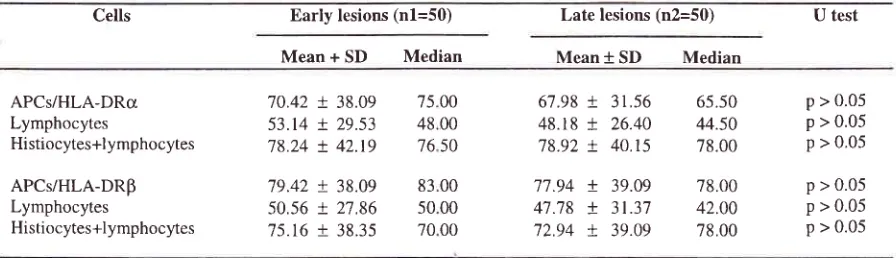
The
absolute numbers
of
HlA-DR-expressing
APCsare showed
in
Table
7.
The
absolute numbers
of
HLA-DR
(o
and B
chains)-expressing
APCs
in the
early
lesions
were
greater
than
those
in
late
lesions,but
werenot statistically significant (p>
0.05).The
expression
of
HLA-DR-o
and
HLA-DR-B
onAPCs in
thecentral part
of
early
lesionswere
as seenin
the part
of
early lesions were as
seen
in
theScatter-diagram 1. There
was a
positive
correlation
between the expressions
of
HLA-DRcI
and Bin
APCs,Med J Indones
the
coefficient correlation
(r)
was0.618
with
95VoC.I.=
0.410-0.765.
This correlation was
calculated
by
statistics
with
confidence/C.I.A. program.
HLA-DR
expressedthe
Bchain more
stronger
than theo
chainin
dermalAPCs, but
in
epidermal LCS,
the expressionof
Bchain
was asgood
asu
chain.The
proportion
of
HLA-DR-cI-
and
HLA-DR-p-expressing
APCs were
the
ratio
of
the
absolutenumbers
of
eachAPCs
to the total number
(sum)
of
lymphocytes
+
histiocytes
+
APC/I
" .'
TheTable
7.
The absolute numbers of HlA-DR-expressing APCsin
the central part of early and late lesions of prurigo HebraCells Early lesions (n1=50) Late lesions (n2=50) U test
Mean +
SD
Median Mean*
SD
MedianAPCs/HLA-DRcr Lymphocytes
Histiocytes+l ymphocytes
APCs/HLA-DRp Lymphocytes
Histiocytes+lymphocytes
70.42
!
38.09 53.14!
29.53 78.24!
42.t979.42
t
38.09 50.56t
27.86 75.16+
38.3567.98
r
31,56 48.18t
26.40 78.92t
40.1577.94
+
39.09 41.78
+
3l.37 72.94X
39.09p > 0.05 p > 0.05 p > 0.05
p > 0.05 p > 0.05 p > 0.05 75 00
48 00 76 50
83 00 50 00 70 00
65.50 44.50 78.00
78.00 42.00 78.00
Note:
SD = standard deviation, APCs = antigen-presenting cellsU test with signihcant difference at p<0.05, highly significant diftèrence p < 0.01.
HLA.DRaIfa and
HLA.DRbEtha
EXPRESSING
ANTIGEN PRESENTING
CELLS
IN PRURIGO HEBRA
G
c
o)
o
at Jo
(U (U
É,
o
3
I
HLA-DRbetha, Acute, Central
Scatter diagram-
I.
The expressionof HU-DRa
and HLA-DR| on APCs^
a^-^ tA
^^^^^:^
^^Àlrât^
a-ara
^
l^
[image:6.612.47.495.269.398.2]Vol 10, No 1, January
-
March 2001proportion
of of
HLA-DR-a- and
HLA-DR-P-e4pressingAPCs
in
the
central
part
of
the
lesions
is presentedin Table
8.
The
proportion of both
HLA-DR-cr- and HlA-DR-B-expressing APCs
in
the late
lesions were
greaterthan that
in
early
lesions,but not
statistically significant (p>0.05).
The
correlation
between
inflammatory
cells,severity,
and
human leukocyte antigen
In
order
to
improve
the
correlation
betweeninflammatory cells
in
early
lesions, theseverity
of
the disease and immunogenetic factorsof
human leukocyteantigen
(HLA),
were performed
in
4l
of
50
subjectsImmuno hist op atho Lo gic a L featue s of pruri go H e b ra
with
prurigo Hebra. Forty one prurigo Hebra
casesconsisting
of 17 mild
and 24
severe
condition.
Female was the majority (28 cases).The
amounts of cell infiltrate inearly
andlate
lesionsof
41 prurigo Hebra
is shown
in Table 9.
Statistically
the
distributions
of
non-specific
and specific cells
were notnormal, Mann
Whitney
method
was used forstatistical
analysis.There
is no significant
difference
between
the
specific inflammatory and
nonspecific
cells
in
early
andlate lesions. Correlation
between B and Tcells,
B and
eosinophil,
LCs and
T, CD4+,
andCD8+ cells
were
weak
and were
not
statistically
significant.
Table 8. The proportions of HLA-DR-o and HLA-DR-B expressing APCs in the central part of prurigo Hebra lesions
Antigen- presenting
cells
early lesions (n=50) late lesions (n=50)
Mean +
SD
Median Mean +SD
MedianU
test
APCs/HLA-DRcr
APCs /HLADRp
47.20 + 15.60
50.10+ 16.80
45.40
-54.1 0
46.30 +
t3.70
48.30.
52.00 +18.10
54.60p > 0.05
p > 0.05
[image:7.612.43.476.327.413.2]Note:
SD = standard deviation, U test with significant difference p<0.05, highly significant difference p <0.01.
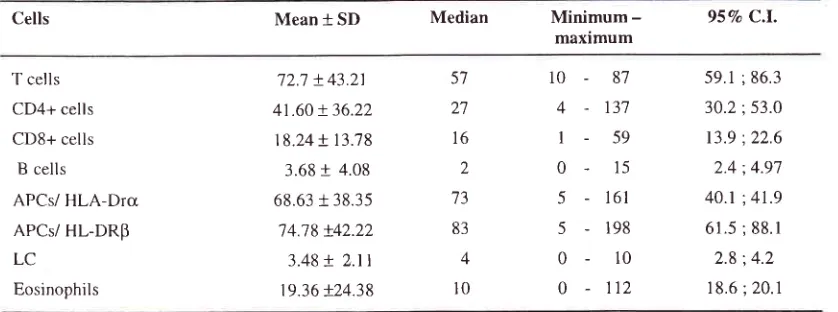
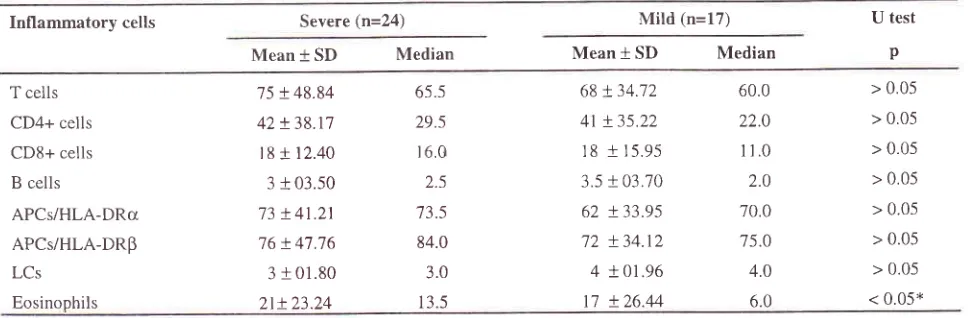
APC = antigen-presenting cellsTable 9. Inflammatory cells
in
early lesionsof
prurigo Hebra cases (n=41)Cells Mean + SD Median
Minimum-maximum 957o C.l.
T cells CD4+ cells CD8+ cells
B cells
APCs/ HLA-Drcr APCs/ HL-DRp LC
Eosinophils
72.'7 + 43.21
41.60 + 36.22 18.24
t
13.783.68
+
4.08 68.63i
38.35'74.78 t42.22
3.48
+ 2.tl
19.36 +24.385't
2'7 16 2
73
83
4
l0
10-
874 -
13'7l-
590 -
155 -
16l5-198
0-
100
-112
59.1 ; 86.3
3Q.2;53.0
13.9 :22.6 2.4 ;4.97
40.1 ;41.9
61.5 ; 88.1 2.8 ;4.2
18.6;20.1
[image:7.612.47.466.492.648.2]-t
Boediardia et al
Correlation between
T,
CD4+, CD8+
cells,
APCsand eosinophils
Table
10.
shows that correlation
betweenAPCs
andT
cells
and
subsetswere
strong
(r =
0.32-0.49),
andsignificant
with
95VoC.
I,
save
for
the
correlation
between
APCs/HLA-DRB and CDS+ cells
(r=0.24).
The strong correlation
betweenAPCs
andT
cells
andtheir
subsets suggestingthat this condition
might
leadto
chronic
inflammation
of
prurigo Hebra.
The abundanceof
APCs
meantthat
a personwith
prurigo
Hebra
was exposed to antigens
or
triggering
factorsfor
a long
time
and thus the
interaction with
T
cells andtheir
subsetsdid
follow.
The correlation
betweenT
cells
andAPCs/HLA-DRP
waspositive
as shown inScatter diagram
2.In
this
analysis, the
correlation between
eosinophils andT
cells
(r=-
0.05,
95VoC.I.=-
0.385;0.255), CD4+
cells (r=-
0.09,95Vo
C.I.=-
9.399
;0.221),
andCD8+
cells
(r=-0.19
with
95VoC.I.
-
0.469
;
0.126)
wereweak.
It
was
doubted whether
the
presence of
eosinophils was due
to
a collaboration between
type-lV
and
type-I hypersensitivity,
or to
insect
bite
reaction
itself.
Statistical
analysis
also
showed
thatthe
correlation between eosinophils and
APCs/HLÀ-DRcr
(r=0.16 with
95VoC.I.
- 0.367
;0.246)
and
thecorrelation between eosinophils
andAPCs/HLA-DRP
(r=0.14
with
95VoC.L
=
-0.180
;0.425)
were
borhweak.
Med J Indones
Table 10. The correlations between APCs and T, CD4+, and
CDS+ cells
Correlationbetween
Correlation"'r;i:#,!:'
correlation
95Vo C.L
APCs/HLA-DRa and
T cells
APsC/HLA-DRcI and
CD4+ cells
APCs/HLA-DRq and
CD8+ cells
APCs/HLA-DRB and
T cells
APCs/HLA-DRp and
CD4+ cells
APCs/HLA-DRp and
CDS+ cells
0.39
0.32
0.49
0.49
0.46
o.24
0.090
0.010
0.188
0.217
0.179
-0.06
0.624
"
0.578 *
0.678 *
0.694
"
0.674 *
0.523
Note: APC= ântigen-presenting
cells,
95VaC.l.
=
95Vo confidence intervalCorrelation
betweensevertty
of
prurigo
Hebra
and
inflnmmatory
cellsTable
11
shows
the
quantity
of
non-specific
andspecific
inflammatory cells in
24
severe casesand
17mild
casesof prurigo
Hebra.
There wasno significant
difference between
the
amount
of
non-specific
andspecific
cell
infiltration in
severe
and
mild
cases,except
for
the
eosinophils.
In
severe
cases,eosinophlis were
predominant (p<
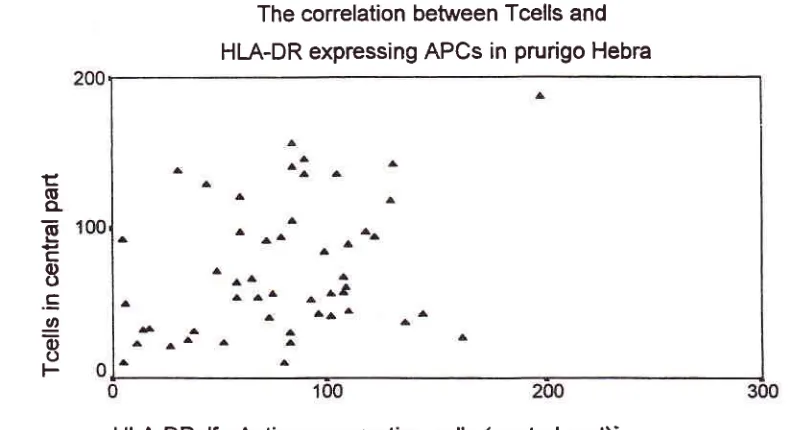
0.05).The
correlation between Tcells
and
Ëo
CL
6
c
c)
o
.s
o
E
o
HLA-DRalfa-Antigen presenting cells (central
part)'
Scatter diagram -2. The correlation between T ceLls and APC/HI-A-DRP
[image:8.612.304.539.118.305.2] [image:8.612.85.479.466.681.2]VoL 10, No 1, January
-
March 2001The
analysis showedthat correlation
between severityof prurigo
Hebra
and
the quantities
of
T cells (r=
0.18),
CD4+ cells
(r= 0.19), CDS+ cells (r=
0.20), andLCs (r=
- 0.22)
were
not statistically
significant.
However,
the
correlation between severity
of
prurigo
Hebra and eosinophils
(r= 0.25) was strong.
It
isassumed
that the
more the number
of
eosinophilspresent,
the more severe thecondition would
be.Correlation
between severity
of
prurigo
Hebra,
eosinophils and
HLA
Eosinophils
in
severe cases
was more
pronounced than thatin mild
ones, and wasstatistically significant
(p<0.05). Further
analysiswith
X2trend
(Table
12)in
Table I
l.
Inflammatory cells in severe and mild cases of prurigo HebraImmunohistopathological featues of
pwigo
Hebra3
groups
of prurigo Hebra
with
severe
condition
showed that 9
caseshad
eosinophils
0-51lcnf;
9 cases had6-10,
and
6
caseshad
2
Il,
the
increastnqrelative risk (RR)
was
not significant
(score
test X'
for
trend=
7.729, p> 0.05).The
sameanalysis
in 17 mild
casesshowed
that
11mild
cases
had 0-5 eosinophils,
4
cases
had
6-15eosinophils, and 2
cases
had 216
eosinophils,
thedecreaiing
RR
wasnot significant (score
testX2 for
trend
=
1.595, p>0.05).
Although it
was
not
significant,
it
suggested
that
prurigo Hebra
with
severe
condition
had eosinophils
>5/1 cm' for
thosewith
mild condition
<5/l cm'.
Inflammatory cells Severe (n=24)
Mild
(n=17) U testp
Mean + SD Median Mean
*
SD MedianT cells CD4+ cells CD8+ cells B cells
APCs/HLA-DRct APCs/HLA-DRp LCs
Eosinophils
75
!48.84
65.542X38.17
29.sl8 + 12.40 r6.0
3
t
03.50
2.573 + 41
.21
73.5 76 +47.76
84.03
r
01.80
3.0 2t+23.24
13.568 !34.'.72 41 + 35,22 18 + 15.95
3.5
t
03.70 62!33.95
72 + 34.12
4
!01.96
17 + 26.44
> 0.05 > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 > 0.05 < 0.05* 60.0
22.0 11.0 2.0 70.0 75.0 4.0 6.0
Note: APCs = antigen-presenting cells. LCs= Langerhans cells. Significant difference
at
p < 0.05 U test = Mann Whitney testTable I 2. The amount of eosinophils in severe cases of prurigo Hebra (n=24)
Groups
(eosinophils/cm2)
Nos.
of
Expected specimensTotal
PH RR
959n C.I. Score test
X2
for
trendr. (0-s)
il.
(6-rs)III.
>
I69
1t.7 20t3 '7.60
4.68
0.745
1.1'7
1.21
0.383
;
1.4500.614
:
2.2400.597
:
2.470Note: Significant difference at p <
0.05
95Vo C. I. = confidence interval [image:9.612.52.537.319.478.2] [image:9.612.53.541.559.668.2]Vol 10, No
l,
January-
March 2001The Immunohistopthalogical
features showedthat
thenumbers
of
cells
in
early and late
lesions
were
not
significant difference,
except
for
CD4+ cells,
which
were
found
significantly greater number
in
early
lesions.
In
both the early
and
late
lesions, the
T,
CD4+, CDS+ cells and APCs were found
in
greatquantities.
This finding
was
compatible
with
thefèature
of type-IV hypeËensitivity.
'/''t
The
abundance of
APCs
and
T
cells and
its
strongcorrelation
probably
indicates
that the
prurigo_lebra
patients
alwaysexposure
toextrinsic
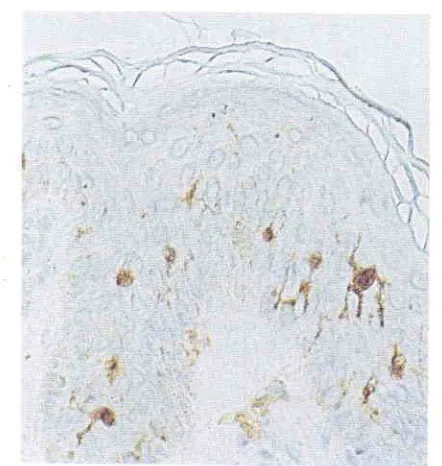
factors.lT'18Protein
5-100 and monoclonal antibodies
of
HLA-DR-cr
andp
wereboth
potential to
usefor
epidermal
LC identification.
Langerhansepidermal
cells
stainedwith
monoclonal
antibodies
of
HLA-DRcr
or
p
andprotein 5-100
with
AEC
substratewas
seenin good
configuration
with
its
dendrite
processus.
Thenumber
rn
late
lesions
was
significantly
moreprofound than
in
early
lesion,
but
the
number
waswithrn normal
limits
(2-87o).B
cells, which normally were not found
in
normal
skin,'?'18were surprisingly
found in few number
Thetàct, that eosinophils were found
in
large
amountsmight
have been related
to
CD4+
cells'
domination,
although statistically
thecorrelation
betweenT
helper(Th) or
CD4+
andeosinophils
wasnot
sigificant.
As
it
is
beenknown
that
T
helper
(CDa+)
cells consist
2subsets,
T
helper
-l
(Th-l)
and
Th-2.
Theoretically
Th-2 cells
collaborate
with
type-I
hypersensitivity
reactions.Th-2 cells
produceIL-3
andIL-5,
cytokines
that act as
attracting mediator
to
eosinophils
andpotentially
stimulate eosinophil
migration
to
theinflammatory site.rT'r8
In
this study
Th-l
and Th-2
werenot
examined.In
this
study
the
severity
of prurigo
Hebra
wassignificantly
correlated
with
hypereosinophils
rn
skinlesions
of prurigo
Hebra patients
with
HLA-410
andits
splits.CONCLUSIONS
The
immunohistopathological
feature
revealednumerous inf'lammatory
cells
consisting
T
cells,CD4+
cells,
CD8+
cells,
T suppressor
cells,
LC
cellsand
HlA-DR-expressing
APCs.
However
thenumbers
of
cells
in
early and late lesions were
notstatistically different, except
for
CD4+ cells,
which
were found
in
significantly
greater
number
in early
Immunohistopathological featues of
pruigo
Hebra
I Ilesions. CD4+ cells were significantly
predominant
than CD8+ cells.
The
eosinophils
were
found
in
abundance, independent
on
the
presence
of
mast cells, plasmacells, basiphils
andB
cells.
The presencemight
be correlatêdwith
CD4+
cells'
domination. The
numbers
of
LC
were
within
normal
limits.
The
correlation
betweenT
cells
andAPCs were
strong,
it
is
indicated
that
prurigo
Hebra
patients
alwaysexposure
to
the
extemal factors, especially
insectsbite. The
severe casesmay
correlate
with HLA-AIO
andhypereosinophils
in skin
lesions. Considering
theimmunohistopathological
findings
it
is
assurned thatthe
mechanisms
of
prurigo
Hebra
was
a mixture
betweentype-IV
andtype-I hypersensitivity
reactions.Acknowledgement
We
would
like to
thank the
head
of
the
Pathology
Department
for
the
possibility
of
the
study
in
immunohistochemistry.
We
aredebtfull
to Ms.
Nunuk
Kurniati
and
Ms.
Neneng Komariah
analysts,
for
their keen
work
in
staining
the
immunoperoxydase
specimens.
Personally,
I
would
like
to
thank
Dra.
Corry
Wawolumaya,
PhD,
MPH
for
statistical
consultations.
REFERENCES
1.
von
HebraF.
Erythema multiforme,lichen
simplex, prurigo, pityriasis rosea, rhinosklerosis.In:
Shelley WB,Crissey
JT,
StokesJH,
Eds.
Classicsin
clinicaldermatology
with
biographical
scketches. Oxford: Blackwell Scientific Publication; 1953. p.ll0-2.
2.
McKenna RW, Mc Kenna MW. Diseasesof
the skin. 6th ed. London: Billairelndall
andCox;
1952. p.331-52.3.
Ormsby DS, Montgomery H. Diseases of the skin. 6th ed.Philadelphia: Lea & Febriger;1954. p. 191-203.
4.
Rook
A, Wilkinson
DS,
Ebling FJG. Eczema, lichen simplex and prurigo. In: Rook A, Ed. Rook's Textbookof
Dermatology. London: Blackwell Scientific Publication;
1972. p.84-9,291-8
5.
Arnold HL, Odomm RB, James WD. Andrew's diseasesof the skin: clinical dermatology, 8'h ed. Philadelphia: WB
Sauders Company; 1 990. p. 1 57-8.
6.
Kocsard E. The problem of prurigo. Austr J Derm 1962; 6:156-66.7.
Boediardja SA. lncidenceof
skin diseasesin
Indonesianchildren
fiom
l98l-1985.
In: Urabe H,
Kimura
M, YamamotoK,
OgawaH,
Eds.Proceeding
of the
4thlnternational Congress of Pediatric Dermatology. Tokyo: University Press ofTokyo; 1986. p. 371-82.
8.
Medical record liom Sub-Dept. of Pediatric Dermatology, Department of Dermato-Venereology, Dr. Cipto Mangun-kusumo Hospital, Jakarta (1990-1997, in press.).9.
BoediardjaSA,
SoelarsitoSA,
Wisnu
IM.
Gambarant2
Boediardja et alKumpulan makalah Ilmiah, Kongres PADVI ke-4. Ujung
Pandang: 1986. h. ll58-65.
Occampo
FA,
ColladeCM.
Acute infantile
prurigo.Clinico
pathological correlationin 100
cases. Austr JDerm 1975; 16:169-73.
Jasani B, Schmid Kw. Immunocytochemistry in diagrostic
histopathology. London:
Churchill
Livingstone; 1993.p.l-27.
Yaoita H. Enzyme labelled antibody method. In: Ueki H,
Yaoita
H,
Eds.A
colour atlasof
dermatohistocytology.Tokyo: Wolfe Medical Publications Ltd; 1989. p. 8-10.
Takezaki
S,
NishiyamaS.
Applicationof monoclonal
antibodies. In: Ueki H, Yaoita H,
Eds. A
colour atlas ofdermatohistocytology. Tokyo: Wolfe Medical Publications
Lrd.; 1989. p.18-23
Hsu S-M, Raine
L
The useof
avidin-biotin-peroxidasecomplex (ABC)
in
diagnostic and research pathology. In:Med J Indones
Ueki H,
Yaoita
H,
Eds.A
colour
atlasof
dermato-histocytology. Tokyo: Wolfe Medical Publications Ltd;
1989. p. 3l-42.
Boenish
T.
Staining methods.In:
NaishSj.
Handbook:immunological
staining
methods.
Califomia:
Dako cooperation; 1989. p. l3-23.Farmilo AJ. Stead RH. Fixation in immunocytochemistry.
In: Naish Sj. Handbook: immunological staining methods.
California: Dako cooperation; 1989. p.24-9.
Bos JD, Das PK, Kapsenberg
ML.
Skin immune system.In: Bos JD, Ed. Skin immune systenl
l't
ed. Boca Raton:CRP Press; 1990. p. 4-7.
Bos
JD
and
KapsenbergML.
Skin
immune system:progress
in
cutaneous biology. Immunology to day 1993;l4:75-8.
Boediardja
SA.
Therole
of immunogenetic factors
ofHLA in Prurigo Hebra. Disertation, Jakarta 1999.
15
1.6
77.
18
1.9
10
11
L2
13
Vol 10, No
l,
January-
March 2001Figure
l.
Prurigo Hebra ih a chiW with severe condition,the skin lesions were seen on the extensor part of the
el<stremities,
but
the body was spare.Figure 3. A mixed cells
infiltration
in early lesion of prurigoHebra eosinophils were predominant than lymphocytes and
hystiocytes (HE, I 20x).
Immunohis topatholo gical featues of prurt go H ebra
l3
Figure 2. The characteristic of
pruigo
papules (dome shapedpapules) were seen on the extensor part of the extremities
Figure 4. The expression of protein S-l@ with DAB
chromogenic substrate, in the epiderma! Langerhans cells
t4
Boediardja etal
[image:13.612.43.255.92.336.2] [image:13.612.298.494.141.335.2] [image:13.612.301.504.425.638.2] [image:13.612.49.276.438.635.2]Figure 5. The expression
of
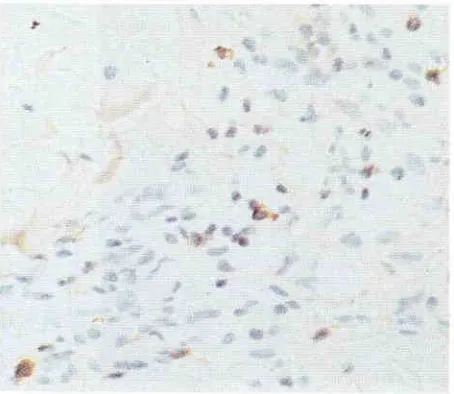
UHCL in T cells in an early lesion of cases No 19. , were clearly seen (brownish in colour), within lymphocytes and histiocytes (lP, I20x).Figure 7. The expression of CD8+ monoclonal antibody in CD8+ cells of an early lesion of cases No. 19., were less
amowt than CD4+ cells (lP, l20x).
Figure 6. The expression ofCD4+ monoclonal antibody in CD4+ cells of an early lesion of cases No.l9., were seen less amount than T cells (lP, 120x).
Med J Indones
Figure 8. The expression of L-26/CD20 monoclonal antibody in B cells of an early lesion of cases No.27., only one B cell
Vol 10, No
l,
Janunry-
March 2001Figure 9. The expression qf
HU-DRa
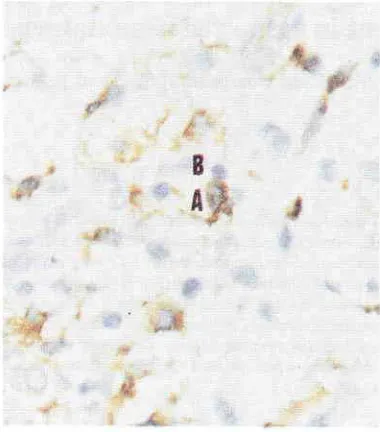
monoclonal antibody in dermal antigen presenting cells (APC) (brownish in colour)ofan early Lesion ofprurigo Hebra. The interaction betvveen lymphocytes and APC was seen (lP, 240x)
[image:14.612.58.251.92.310.2] [image:14.612.302.492.96.312.2]Immunohistopathological featues of prurigo Hebra
l5
Figure 10. The expression of Hl,A-DRp monoclonal antibody in dermal antigen presenting cells (APC) (brownish in colour)
of an earLy lesion of prurigo Hebra. The interaction between