Vol 6, No 3, July - September l99V Vitanin A Level in Hydatidiform MoIe
r53
A
Case-control Study of
Vitamin
A
r,evel
in Hydatidiform
Mole
Andrijono*, Kukung Kurnia*, Nur
Asikin**
Abstrak
Mola hidatilosa merupalan kehamilan abnormal yang masih merupal<an masalah dalam usaha meninglcatlcan derajat l<esehatan reproduksiwanin' larena kciadiannyayang cukup tinggi serta lcarmakomplikasiyang dapat ditimbultun. pencegahandapat
dilaladcan bila faktor etiologi atau faloor
isiko
wanita penderita moln hidartdosa t"tonaUnnttii.
iujuan penelitian ini adatan unntk mengetahuifaktor
isiko
tersebut yang diduga salah satunya adalah kadar vitamin A yang rendah- Penelirian ini merupalcan l<asus kontrol. Kasusadalah30orangpenderitotnolahidartdosadenganlantroladatahwaniiahamildengan padanan
umui sela4
nhun
dan parttassela I ' Dilakukan
pengukuran
Pearson. Kadar rata-rata retinol darahpendein
molahidatidosaadalah
10,52
89ytg/dl. Keduanilaitersebut berbedabermalnasecara statistik. R.isiko teriadinya mola hidatidosa pada wanita hamil berusia
3
24 tahun dan mendertta defisicnsi berat vitan in A adalah 6'29 l(ali lebih rtnggi dan pada wanita berusia 3 24 tahun, berparitas nol dan menderita defisiensi berat vitamin A adalah 7 kali lebih ting gi dibandinglcan dengan kontrol.Abstract
Hydatidifurm mole is an abnormal pregnancy which constitutes a problem in the effort to improve the reproductive health level of women because of its high incidence rate and complicartons that ntoy;rise. Preventioimay be perfomed if eiotogicatfactors
or
risk factors of thewomenwith hydatidiform mole have beenidmtified. The aim of this sndywasti ide)ttyy
tt
or" riskfactors. One of the rtskfactor was susPected to be a vitamin A level. This
stufi
was a case,ortroi
sndy.Tie
,or", -rr"'30
patients with hydartdifurm mole and the control were Pre?nant women of equivalent age of 4 years interval and partty interval ofl.
Th"^"^ur"^ent
of fasrtng blaod retinol level was done using Neeld and Pearson's method. The average level of blootl retinol of the patients with hydatiform mole was 10'52 1tg/dl' and the average blood retinol of the control patien* wàs 12,89]ts/dl;
startsticaliy itias
significantlydffirent.
The riskfo
ceofhy
thepregnantwomenofl
24yearsofagewithr"r"rid"Sri*"y
2gtimeshi
riskfor
in the women of < 24 years with nit parity and severed"trciency
rnany as7
than inKeywords
:
Vitamin A, hydatifurm moleINTRODUCTION
Hydatidiform
mole
is oneof
theproblems
in
women's
reproductive health. This
is because
this
diseaseis
suffered
mostly by
women
of
young
age andwithout
children who
still
need
their reproductive
functions,
andits
incidence
is high
enough, i.e.
oneof
60
preg-nancies
or
16Vo.1,2One
of
the most
dangerous
hydatidiform
mole complications is the occurrence
of
malignancy degeneration
which
results
in
the
failure
of
reproductive functions, or
even death.3'aOne
of
the
efforts
to
promote
women's
reproductive
health
is
through the prevention
of
the occurrence
of
hydatidiform mole by
undertaking
the
studies
on
theetiology
of
this
disease and
its risk
factors.
The
decreaseof
hydatidiform mole incidence
will
be
agreat significance
in
the
efforts to
promote women's
reproductive health.
Hydatidiform mole
is
an abnormal
pregnancy
indi-cated by degenerationofhydropic
chorionic
villi,
avas-cular chorionic
villi and
proliferation
of
trophoblast
*
Departmentof
Obstetics and Gynecology, Facultyof
Medicine, University
of
Indonesia/
Dr. Cipto Mangunkusutno General Hospital, Jakarta, Indonesia**
Department of Biochemistry, Facuhy154
Andrijonoetal.cells.5'6
The causeof
these changes hasnot yet
beenidentified. However,
it
hasbeen understood
that
thechanges
in
cell
differentiation and
cell
prolifera-tion
are causedby
the disorderof intracellular
metabo-lism.
One of the metabolism
chainsis
thefunction of
vitamin
A.7'8'9Therefore, it will
beinteresting
tostudy
whether there is
acorrelation between vitamin
A
andthe incidence
of
hydatidiform mole. This study
isperformed
with
thepurpose of attempting
to give
thetentative
answerto
thatproblem.
MATERIALS
AND METHODS
The study was designed
as a casecontrol
study.
The cases were the patientswith hydatidiform mole
and thecontrols were the pregnant women.
Two determining
factors were
ageand parity.
Thesetwo factors
were used as matchedparity
with
aninterval
of one and ageswith interval
offour.
All
the patientswith
hydatidiform
mole which
met thecriteria of
the study wereincluded
in the study,
and thesematched factors
served as thecontrol.
Thepatients with hydatidiform
mole included
in this
studywere
thoseevacuated
at Dr. Cipto
Man-gunkusumo
Hospital, neither receiving blood
trans-fusion
yetnor
thetreatment with vitamin A
>5000IU.
The measurement
of
vitamin
A
performed was
thelevel
of
fasting retinol,
andit
was
carried out at
theLaboratory
Research Center
for
Immunoendocrinol-ogy
Jakarta, according
to
Neeld
and Pearson's
method.lo
RESULTS
During the period
of
a year study (June 1990-May
l99I),
a number of 30 cases ofhydatidiform
mole werequalified for the
study.The
average caseswere 25
years( + SD: 5,73
)
with
the youngest age being 18 years and the oldest
40 years.The
average ageof
thecontrol
group was 26,43years ( +
SD: 4,28 ), the youngest
agebeing
14 years and theoldest
38 years.Forparity,
70Voofthe
cases and 76Voofcontrol
group
had parity
of
1or 0, the rest
hadparity
more
than
1.The
averageeducation length
of
casegroup
was 7,96 years ( +SD:
3,64 )while
thecontrol
groupbeing
10,7 years( + SD:
3,78). Statistically, all
thesefactors did
not differ significantly.
Med J Indones
The Level
of
vitamin
A
Table 1. The average level of vitamin A in
both
groupsGroup x SD
Mole Result
30 30
r0.52
12.89
3.94
3.93
Z = 2,33 p < 0,05
The results
of
the study revealed
a
significant
dif-ferencein vitamin
A
level between the
casegroup
of
hydatidiform mole
andthe control group. The lowest
vitamin A level found
in
the casegroup
was 5,0pg/dl,
the highest level was 17,5
ltgldl, while
the
lowest
vitamin
A level in
thecontrol
group was6,7
ltgldl,
and
thehighest level
was2l,81tgldl.
These
results showed
a
significant
difference
in
vitamin
A
between the patients
with
hydatidiform
mole
andnormal pregnant women.
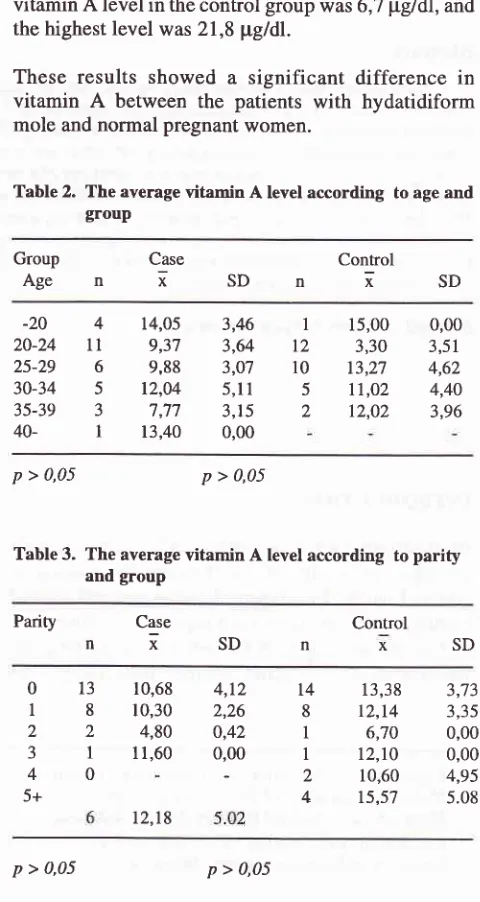
Table
2.
The average vitamin A level according to age and groupGroup
Case
ControlAgeniSDniSD
-20
420-24
1l25-29
630-34
535-39
340-
115,00
0,003,30
3,51t3,27
4,62tt,o2
4,4012,02
3,9614,05
9,37 9,88
12,04
7,77
13,40
3,46 3,64 3,07 5,1I 3,15 0,00
I
t210 5 2
p
> 0,05p
> 0,05Table
3.
The average vitamin A level according toparity
and groupParity Control
x
Case
nx-SDn
SD4,12
142,26
80,42
10,00
I
-2
4
013
t8
22
3l
40
5+
10,68 10,30
4,80 I1,60
12,18
13,38
3,7312,14
3,356,70
0,00t2,10
0,0010,60
4,95t5,57
5.08 [image:2.595.307.547.293.744.2]Education
Case(year) n
i
SDControl
nxSD
Vol 6, No 3, Jaly - September 1997Table
4.
The average vitamin A level according to the level of education in both groupsVitamin A Level in Hydatidifurm
MoIe
155Analysis
of the women
in
the
agegroup
lessthan
24years.
Table
6.
Yitamin A deficiency in the case and control group with age less thanZ
years oldGroup Vit.
ADef.
(+)
Vit. A Def. (-)Case (mole)
Control (pregnant)
P
=
0'038 OR = 6,29These data suggest
high risks, i.e. 6,29 times
in the
women group
of
<
24
years
of
agewith vitamin
A
deficiency
for
developing
hydatiform
mole.
Table
7.
Vitamin A deliciency in the case and control group withparity
of 1 or lessGroup Vit. A
Def.
(+) Vit. A Def. (-) TotalCase (mole)
Control (pregnant)
p > 0,05 OR = 3,38
0t
l-6
157-12
1312+
I
13,40
0,0010,99
4,389,24
2,95l7,to
0,0014,86
4,0511,88
3,6815,20
3,54l5
l3
8 20 2
ll
p > 0,05 p > 0,05The results
showed
no influence
of
age,parity
andeducation
with
regardto vitamin A level.
These threefactors
in
our study did not
seemto affect
the study onvitamin
A in
both the case group and thecontrol
group. Thus, these resultsdiffered
from
several studieswhich
suggestedthat the
above three factors
play
arole in
affecting
vitamin A
level.
Vitamin A defïciency
The
assessment
of risks for
the
occurrence
of
hydatidiform
molein vitamin A deficiency
showedOR
-)
\1
Table
5.
Distributionof
casesand
controls
according to the presence or absenceofvitamin
A deficiencyGroup
Vit.ADef.
(+)
Vit.A Def.()
Total2t
l2
l8
Cases Controls
Total
p > 0,05 OR = 2,51
Although there was no statistical difference,
it
wasevident
that the percentageof vitamin A
deficiency
in
the patients
with hydatidiform
mole
(43,33Vo) was
higher than that
of
control
group
(23,33Vo).In
thedistribution of
age andparity,
themajority of
age andparity
in
the casesof
hydatidiform
mole
were the casesof
less than 24
years
of
age,
and parity
of
1.
This
finding
wasin
according
with
theliterature
suggestingthat the highest incidence of
hydatidiform mole
oc-curred
in
theyoung women
with low parity. It
will
beof
interest
to
study
suchtendency
separately.On
theother
hand, analysisof
thepatients
with parity
of
1 showedno significant difference (OR
-
3,38).
It
will
be
of
interest, therefore,
to
perform a
separate studyof
the caseswith nil parity.
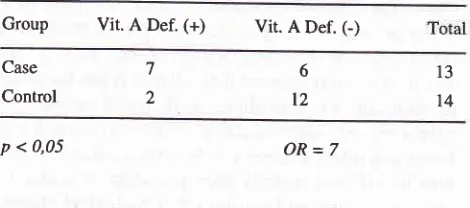
Table
8.
Vitamin A deticiency in the case and control groupwith nil parity
and age less than 24 years oldl3
7
t7
23
30 30
40 20
Group Vit. A Def.
(+)
Vit. A Def. (-)Case Control
7 2
6
l2
13
14
p < 0,05
OR=7
It
isobvious
that there is asignificant different
betweenthe
caseand
control
groups
with
nil
parity,
age less [image:3.595.297.531.93.282.2] [image:3.595.294.529.589.693.2]156
Andrtjonoetal.of hydatidiform mole
in the women
of
less
than
24years
with
nil
parity and suffering
from
vitamin
A
deficiency
is 7 times higher
thanin
thecontrol
group.
Histologic Classifrcation
Several investigators
did not
find the influence
of
histologic classification
on the
likelihood of
thepost-hydatidiform mole malignancy. However,
this
his-tologic classification did not provide
a
brief
description
of the essential changes in trophoblast cellsthat
occurred, i.e.
the
more severe and
the
more
numerous cases
were classified
as
the more
severecases.
Histologic classification
of
hydatidiform
mole
commonly referred to is
theclassification
accordingto
Hertig-ManseI.rr
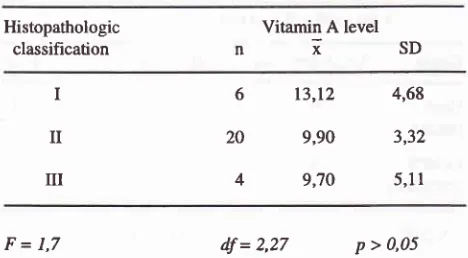
Table 9" The relationship between histopathologic classifi-cation and
the
average vitamin A levelHistopathologic classification
Vitamin A level
nisD
6
13,12
4,6820
9,90
3,324
9,70
5,11F=1,7
df = 2'27 p > 0,05Statistically, there was no significant difference
be-tween
histologic level
andvitamin
A
level. However,
it
was evident
that
the
higher
the
histologic
changes, thelower
thevitamin
A
level.
DISCUSSION
One of the diagnostic parameters of
hydatidiform
mole
is
the presence
of
trophoblast
cell proliferation.
Thedirect
causeof
this proliferation
is
not
known
yet.
The in vivo study showed that
vitamin A has
theeffect
of inhibiting
or
controlling
cell
proliferation
and enhancingcell differentiation.T'8'e How vitamin
A
per-forms that
role is unclear
yet. Several mechanisms
that
may
be
affecæd
include protein
system
of
kinase
C, cascadesystem, and several other
biological
effects,
such
as
enzyme
synthesis,
genomic
expression,
ex-tracellular effects, immunologic activity
and protein
kinase
C cascade.r2'13'14'15
It is of
interest,
therefore"Med.tr Indones
to study whether
vitamin A also
plays
arole against the
proliferation
of trophoblast cells.
Started
by
clinical
study, i.e. control
case
study to
identify the correlation
of
the
occurrence
of
hydatidiform
mole
and vitamin Alevel, the analysis
of
vitamin A level
showedthat the
majority of
the
casesand
controls had vitamin
A
level
below the
normal
(20 -40
pg/dl).
These results su ggest that mo st pregn antwomen
in
the studysuffered
from vitamin A
deficien-cy. This
situation calls
for
special attention
on
the impacts it may have on pregnancy and how to deal withthem. The
level of
vitamin
A deficiency
ismildif
blood
retinol level is 10-20
pgldl,
andthedeficiency
is severeif
theretinol
level is
< 10 pgldl.
However,
the average resultsof vitamin A
level
in
the cases of hydatidiformmole
and
in
the
control group were statistically
dif-ferent.
Analysis
of
age,parity,
and education factors
did not
seemto show
different
result. Education
factor
is suspected to
play
amajor role
because there is a closecorrelation between education and
socioeconomic
conditions. Furthermore,
the
socioeconomic
condi-tions
play
a majorrole in thequality
ofnutritional
food.
This correlation
suggests aprobable role
of vitamin A
deficiency
in
the incidenceof hydatidiform
mole.
One
of
the
hypotheses
explaining the
occurrence
of
hydatidiform
mole is the
"blighted-ovum"
theory. The
genetic study
revealed
that the
genotype
of
hydatidiform mole
was
of
the
father's
gene,
without
the mother'r.16
Thur,
hydatidiform mole
originates
from
fertilization
without
mothers factor, i.e. theovum
whose _gene
factor
is
not
fertilized
by the father's
sperm.tt However, this situation
still
requires other
factors because notall
theblighted ovum develops
into
hydatidiform
mole.
This
otherfactor
is yet to be
iden-tified.
And the factor that we
attempted
to
study
is
vitamin A
deficiency.
Epidemiological
study
of hydatidiform
mole revealed
that hydatidiform
mole was generally
developed by
pregnant women
of
young
agewithout children. This
risk factor
also constitutes the problem that is yet to be answered.It
isofinterest,
therefore, to perform astudy
on'the
factors
of
young
age,low parity or
nil
parity,
and
vitamin
A
deficiency.
The
interesting
dataof
our
study are the data cf hydatidiform mole patients of<
24years
of age
suffering
from severe
vitamin A
deficien-cy. These data suggest a
significant difference between
the case and the control group. The risk
for
developing
hydatidiform
mole increases
6,29 times
if
the woman is under 24 yearc, pregnant, and sufferingfrom
severevitamin A
deficiency.
I
II
[image:4.595.53.287.345.474.2]Vol 6, No 3, July - September 1997
Similarly,
in
the casesof
< 24 yearswith nil
parity,
thedata
found
revealed
therisk
of
7 times higher
thanin
the
control group.
Themagnitude of risk for
theoccur-rence
of hydatidiform mole
by
the
accumulation
of
these
factors
underlines
that the etiology of
hydatidiform
mole is
multifactors.
Thus, the
prevention
for
the
occurrence of
hydatidiform mole should
be
attempted through
various
aspects. Nevertheless, as
it
is
a
natural
phenomenon that
thefirst
pregnancy occurs
atyoung
age, therisk
factors
thatplay
a role, such asvitamin
A
deficiency. The
severity
of histologic
changes can be seenfrom
the compared data ofhistologic lèvel
and theaverage
vitamin A level. The lower vitamin
A level
reflects the more
severe
histologic
changes
of
hydatidiform
mole,cells.
Several studies
of
histologic
levels ofhydatiform mole
revealed
that
this histologic level did not affect
therisks
for
the
occurrence
of
malignancy
degeneration(Genest
DR
et al.personal communication).
Thus, theresults
of
this
study are sufficient
to
show that
thewomen
of
<24
yearswith nil parity
andsuffering
from
severe
vitamin A
deficiency
have therisk for
develop-ing hydatidiform mole
seventimes higher.
Vitamin
A
level
in
thepatients
with hydatidiform
mole
comparedwith
thepregnant woman
control
andhistologic
chan-ges,
which
occurred more severely
with
the lower
vitamin A level,
suggest a stronglikelihood
of
therole
of vitamin
A
level deficiency
in the
occurrence
of
hydatidiform
mole.
CONCLUSION
There
is
asignificant
difference
of vitamin A
level
in
the patients
with
hydatidiform mole
and
the
control
group.
Therisk for
developing
hydatiform
mole
in
thewo-1nen
less
than 24
years
of age
with
nil
parity
andsuffering from
severevitamin
A
deficiencyls
7times
higher.
Vitamin A Level in Hydatidifurm
Mote
157REFERENCES
l.
Sastrawinata S. Permasalahan penyakit Trophoblas. Semi_ nar Sehari Penanggulangan Penyakit Trofoblas, Band,rng,1987
2. Martaadisoebrata D. Epidemiologi penyakit Trophoblas di Indonesia. Simposium Sehari Neoplasma Trofoblas, Jakar-t41984
3. Kashimura
Y,
KashimuraM,
Sugimori H, Tsukamoto M.Prophylactic chemotherapy
of
hydatidiform mole. Cancer 1986:'58:624-94. Kim DS, Moon H, Kim KT, Moon
yJ,
Hwangyy.
Effectof
prophylactic chemotherapyfor
persistent trophoblastic disease in patients with complete hydatidiform mole. Obstet Gynecol 1986; 67:690-95. Lurain JR. Natural History Gestational Trophoblastic
Dis-ease. In: Szalman AE, Buchsbaum HJ, editors. Gestational Trophoblastic Disease. New
York:
Springer-Verlag, l9g7:3-8
6. Tyrey L. Laboratory Methods for the euantitation of Human Chorionic Gonadotropin. In: Szalman AE, Buchsbaum HJ,
editors. Gestational Trophoblastic Disease.
New
york
Springer-Verlag, 1987
7. Sporn
M.B.
Retinoids and Cancer: Introduction. Cancer Surveys 1983;2:221-28. Goodman De Witt S. Vitamin A and retinoids. In: Health and disease. N Eng J
Med
1984; 16:1023-319. Menkes MS, Comstock GW, Vuilleumier Jp, Helsing KJ. Serum Beta Carotene, Vitamin
A and
E, Selenium, and the risk of Lung Cancer. N Eng J Med 1986; 13:1250-4 10. Neeld JB, Pearson WN. Macro and micro method for thedetermination of serum vitamin A using Trifluoroacetic acid.
J Nuh 1963; 79:454
11. Hertig AT, Sheldon WH, Boston M. Hydatidiform mole.
A
pathological-clinical correlation of 200 cases. Am J Obstet Gynecol, 1947; 53:l-3612. Schroder
E,
RapaportE,
Blackj pH.
Retinoids and cell proliferation. Cancer Survey. 1983; 2:223-3713. Bertram JS. Inhibition of neoplastic transformation in vitro by retinoids. Cancer Survey 1983; 2:23g-53
14. Sporn MB, Roberts. AB. Retinoids in Differensiation and carcinogenesis, JNCI 1984; 73:
l38l-9
15. Muso Y, Moriwaki H. Antitumor activity of vitamin A and
its derivativos. JNCI 1984; 73:1384-93
I 6. Inchinoe K.,lVlechanism of Origin of Hydatidi form mole and
Its
ropensity
to
malignancy.
In:
Ichinoe
K, editor.