Vol 4, No 3, July - September 1995 Breast Cancer Among Japanesse Women 177
A
Case-Control Study of Breast Cancer among
Japanese
\ilomen
in Tokyo
Kenji
Wakai', Yoshiyuki
ohno', Sadao
Suzuki*,
Susurnu WatanabeT,Goi Sakamotot
andNakako
Kubo$Abstrak
Untuk meneliti faktor risika kanker payudara saat ini, dilakukan penelitian kasus-lantrol pada runah-sakit di Tolcyo, dari tahun 1990 sampai 1991. Informasi mengenai faktor risiko potensial didapat dari kwesioneryang diisi sendiri oleh 5.084 pasien rawat jalan.
Dari
pasien tersebut diilapati00
kasus kanker payudara, dan dipilih 900 kontrol secara acak yang umurnya sesuai. Temuan bermalon adalah: (a) semakin tinggi jumlah kelahiran hidup, semakin kecil risiko pad.a wanita pramenopause (risiko relatif (RR) yang itisesuaikan untuk 3 atau lebih kelahiran hidup terhadap tanpa kelahiran hidup: 0,24; 95Vo interval kepercayaan (IK) : 0,08 - 0,65); (b) pada wanita Pramenopause, siklus haid teratur meningkatkan risiko (RR yang disesuaikan: 2,50; 95Vo IK : 1,16-5,35), dan peningkatan lama siklus mengurangi risiko (P untuk kecenderungan linier < 0,05); (c) perokok masa kini mengalami peningkalan risiko(1,6j;
1,11-2,j9)
untuk semua wanila, dan(2,7j;
1,38-5,39) untuk wanita pasca menopause); (d) wanila yang kegemukan mengalamirisiko
lebih besar mendapat kanker payudara pasca menopause: RR yang disesuaikan untuk yang berbobot 70 kg atau lebih terhadap yang berbant 50 kg atau kurang adalah 4,82 (95VoIK:
1,53-15,2); (e) semakin tua usia melahirkan anak pertama, semakin tinggi risiko kanker payudara pasca menopause (2,85; 1,16-6,99, dan 3,54; 1,03-12,2 untuk umur 30-34 dan 35 tahun atau lebih). Risiko kanker payudara pra menopause dan pascamenopause ridak berhubungan dengan riwayat kanker payudara pada keluarga, riwayat penyakit payudara jinalg umur saat haid pertama dan menopause, Ialaasi, kebiasaan mkum alkohol dan linggi badan.Abstract
To explore the risk factors
for
recent female breasl cancer, a hospital-based case-conlrol study was conducted in Tokyo,from
1990 ro 1991. Information on potential risk factors was obtained by a self-administered questionnaire from 5.084 out-patients. Of the patients,300 incident breast cancer cases were recruited, and 900 age-matched controls were randomly selected. Significant
findingi
are: (a) the more the number of livebirths, the smaller the risk in premenopausal women (adjusted relative .a,sk (RR) forj
or more binhs relativeto none: 0.24; 95Vo confidence intental (CI): 0.08-0.65); (b) in premenopausal women, regular menstrual cycle increased the risk (adjusted RR: 2.50, 95Vo CI: 1.16-5.38), and its increasing duration decreased the risk (P
for
linear trend <0.05); (c) current smokersexperienced an increased risk (1.6j, 1.11-2.39 for allwomen and (2.73; 1.38-5.j9) for postmenopausalwomen; (d) obesewomenwere al a Sreater risk of postmenopausal breast cancer: adjusted. RR
for
those weighingT0 kg or more relative to those weighing 50 kg orIess being 4.82 (95Vo
CI:
1.53-15.2); (e) the later the age at first livebirth, the higher the postmenopausal breast,onr"riitk
g2-.BS;1.16-6.5q and
j.54;
1.03-12.2for
ages of j0-34 and 35 years and more, respectively). Neither premenopausal nor postmenopausal breasl cancer risk was independently associated with family history of breast cancer, history of benign breast disease, iges at meiarche and menopause, lactatiory drinking habits and body height.Keywords
Z breast cancer, risk factor, premenopausal, postmenopausalRisk
factors
incriminated for
female
breast cancerin-clude
farnily
history
of
breast
caucer,l-8
history of
benign breast
disearç,t'''o early
menaréhe,l'5,0-tz'tur" rnenàpause,2-4'10'll'13'
lale
aze at firstbirth/full-lenn
pr"grlun.y,
l'3-6'8'e'12't4' t5 unJlo*
pa ri ty (a s rna I I num-ber
of
full-term
pregnancies).1,6,8,e'10'14Obesity
is also an establishedrisk
factor for
lreast
cancer among postmenopausal women .l'8,11,16,17Breast-feeding is reported as a
protective factor
againstbreast cancer.
Alcohol
consumotionz'3's'6.8.12'13'18.19 andsmoking
habits3'8'1e-22,"-"in to
beexplbred
fur-ther assignificant risk
factors
of
breast cancer.In Japan,
age-adjusted
incidence
(adjusted
by World
Population)
of breast
cancer
was 13.5
per
100,000population
in
1.g7523andZ4.3in19B5.2a
this
increase isconceivably
ascribable torapidly changing
lifestyles
among
Japanese women.It
is, therefore,
of
impor-Departme,tt of Præentive Medicine, School of Medicine, Nagoya_University,
t_Departmen
lrclitnte Hospital, Tokyo 170, Jopan+
Departmen
rcer lrctilule Hospitat,Tolqo
170, Jaoanç D)portmenr
of
Pubtic Health, Med.ical School, Nagoyo Citytance and
significance
toexplore
the recentrisk factors
for
breast cancer among Japanesewomen.
METHODS
Inforrnation on potential risk factors
wasobtained by
aself-administered questionnaire from all out-patients
who visited
theDepartment of
BreastSurgery,
CancerInstitute,
Tokyo from May 10,
1990 toMay
31,199I.
Items surveyed
were age, menopausal staius,
family
history
of
breast caneer,history of benign
breastdis-easç,
regutarity
and duration
of
menstrual
cycle (for
premenopausal
women),
ages
at
menarche
andrnenopâuse, age
at first birth,
number
of
livebirths,
episodes
of
lactation, smoking and drinking
habits,height
andweight.
Theseinformation
have beenreadi-ly
collected
from all out-patients before examination,
that
iq
prior
to diagnosis.
Of the
5,084 female patients during
thestudy period,
314
were newly
diagnosed
as having
breast
cancerhistologically. Of
the 314
breast cancerpatients,
weexcluded 11 patients
with
missing information
on rnenopausal status, onepatient
under 25 yearsold,
and2
patients
with
history
of
other malignant
tumors.Tbus, 300 incident
patientswere eligible
casesfor
the presentstudy.
Controls were randomly selected from
the rernaining
4,770 patients without
breast cancer,excluding
thosewith missing
information
on menopausal statusand/or
with history of
othermalignant tumors.
Threecontrols
per case
were randomly
selected,rnatching
eachother
for
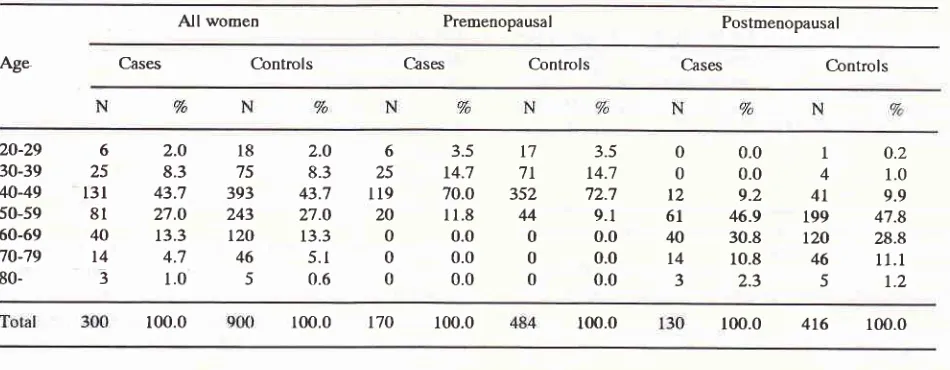
age (as nearest aspossible). Table
I
shows the agedistribution of the study subjects (300
casesand
900controls),
and those relatedto
the menopausal status.Table
l.
Age Distributionso[
Cases and C.ontrols in general and classified by menopausal statusAll
analyseswere performed for premenopausal
andpostmenopausal
women,
separately
and totally.
Obesity index was calculated as Quetelet's index,
defined
asweight (in kilogram) divided by
the secondpower of height
(in
meter).Unconditional multiple logistic regression
analysis2swas undertaken
to
obtain RRs adjusted
for
age
andother variables
potentially confounded. In the
multi-variate
analysis,study subjects with missing
informa-tion were also included
as anadditional category.
A
linear trend
in RRs, derived from the
logi-s-ticmodel,
was
examined by
themethod of
Rothman.zÔRESULTS
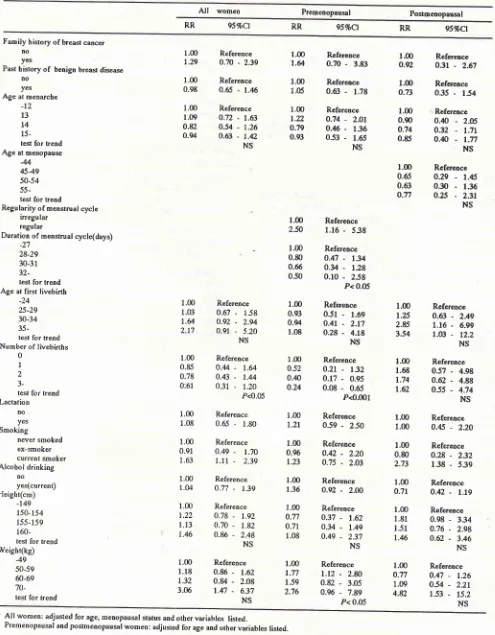
Table
2
shows
the RRs obtained
by
unconditional
multiple logistic
regression analyses.After
adjusting
for
other variables
(see footnote
of
Table2),
asignificantly
increasedrisk ofbreast
cancerwas apparent
among premenopausal
women,
when
menstrual
cycle
wasregular (RR: 2.50;
957oCl:
l.16-5.38). The longer
theduration
of menstrual
cycle,
the smaller the riskwith statistical significance
(P fortrend
<0.05).
Late
age
at first birth
was linked
to
the risk
in
postmenopausal women (2.85; l.L6-6.99)
and
(3.54;I.03-12.2)
for
ageof 30-34
years,and
thatof
35 years andolder
respectively. Number of livebirths
was
in-versely correlated
to
breast cancer
risk
in
premenopausalwomen
andall
women, independently
of other factors (P
for trend
< 0.001 and<0.05,
respec-tively).
All
women Premenopausal PostmenopausalAg.
Cases
C)tntrols
Cases
Controls
Cases Controls20-29 30-39 40-49 50-59 60-69 70-79
80-2.O
8.3 43.7
27.O
t3.3 4.7
1.0
2.O
8.3
43.7
27.O
13.3 5.1 0.6
3.5 14.7
70.0 I1.8 0.0 0.0 0.0
3.5 t4.7 72.7
9.1
0.0 0.0 0.0
0.0 0.0 9.2
46.9
30.8
10.8
2.3
0.2
1.0 9.9
47.8 28.8
LI.I
1.2l7
7t 352
44 0
0 0 6
25
119
20
0 0
0
18
75
393 243 120
46
5
6 25
t3l
8l
40
t4
-5
0
0
t2
61
40
t4
31 4
4I
199t2a
46 5 [image:2.595.56.531.538.723.2]Vol 4, No 3, July - September Ig95
Table
2.
Adjusted Relarive Risksfor
Breasr cancerin
UncondirionarBreast Cancer Among Japanesse
Women
179I-ogistic Regression Analysis'
All
women Premenopausal PosmeoopausalRR 95%Ct RR 95%Ct RR 95%Cl
Family history of b,reast cancer
lto yes
Past hislory
of
benign breasa disease noyes Age at nrenarche
-12 t3 t4
15-test for trend Age at menopause
-44 4549 50-54 55-test for trend
Regularity of menstrual cycte
irregu lar regular
Duration of menstrual cycle(days) -27
28-29 30-3r
?7_
tesl for lrend Age at first livebirtb
-24 25-29 30-34
35-test for lrend Number of livebirths
0
1 2
3-tesl for trend Lactation
no-yes
Smoking never smoked ex-smoker currenl snoker Alcobol drinking
no yes(current) Height(cm) -149 150-154 155-159
160-test for arend
Weiglrt(kg) -49 50-59 ffi-69
70-test for trend
1.00
Reference1.29
0.70-
2.391.00
Reference0.98
0.65-
1.461.00
Reference1.09
0.72-
1.63o.82
0.s4-
1.260.94
0.63-
1.42NS
1.00
Referencet.u
0.70-
3.831.00
Reference1.05
0.63-
1.781.00
Referencet-22
0.74-
2.Oto.79
0.46-
1360.93
0.53-
1.65NS
Reference
o.2t
-
132 0.17-
0.95 0.08-
0.65 P<).001Reference 0.59
-
2.501.00
Reference0.96
0.42-
2.201.23
0.75-
2.031.00
Reference1.36
0.92_
2.W1.00
Refereoce0.77
0.37-
1.620.71
0.34-
L.491.08
0.4e-
2.37 NS 1.00 1.77 1.59 2.76 Referencet.t2 -
2.8A0.82
-
3.05 0.96-
7.89 P< 0.051.00
Referenceo.92
0.?l
-
2-671.00
Referenceo.73
0.35-
1541.00
.Rèference0.90
0.,10-
2.05o.74
0.32-
t.1l
0.85
0.&
-
t.n
NS
l.m
Reference0.65
0.29-
1.450.63
0.30-
1.36o.Tt
o.25-
2.37NS
1.00
Referencer.û3
0.67-
158l.Q
O.Ez-
2.942.17
0.91-
5.20 NS1.00
Reference0.85
0.44- t.u
0.78
0.43-
1.440:61
0.31-
1.20P<0.05
1.00
Reference1.08
0.65-
r.801.00
Reference0.91
0.49-
1.70t.63 t.tl -
2.391.00
Referencer.u
o.77-
1.391.00
Reference1.22
0.78-
1.921.13
0.70-
1.821.46
0.86-
2.48 NSl.m
Reference250
1.16-
5381.00
Reference0.80
0.47-
1340.66
0.y
-
1280.50
0.10-
258 P< 0.051.00
ReferenceO.ca
0.51-
1.690.q
0.41-
2.171.08
0.28-
4.18 NSl.m
Referencet-25
0.63-
2A92.85
1.16-
6.ee3.54
LA3-
12.2NS
1.00
Reference1.68
0.57-
4.981.74
0.62-
4.881.62
0.55-
4:t4 NS1.00
Reference1.00
0.45-
2.201.00
Reference0.80
0.28-
2322.73
1.38-
5391.00
Reference0.71
o.42-
t.tg
1.00
Reference1.81
0.98-
3341.51
0.76-
2.981.46
0.62-
3.46 NS1.00
Refereoceo.n
o.47-
1.261.09
0.54-
2.214.82
1.53-
15.2NS r.00 o-52 0.,m 0.24 1.00 t.2t 1.00 1.18 1.32 3.ffi Reference 0.86
-
1.620.84
-
2.08 1.47-
6.37 NS'
All wonren: adjusted for age, menopausal slatus and other variables listed. [image:3.595.51.546.96.731.2]Current
srnokers were atsignificantly
greaterrisk
inall
women
(1.63;
l.ll-2.39)
and
in
post-menopausal
wornen
(2.73;
1.38-5.39).
Women, when
weighing 70 kg or
more, were also
atgreater
risk (RR:
3.06
in all
women,
2.76
i.npremenopausal
women,
ancl4.82
in
postmenopausalwomen).
For
premenopausal
women, a significant
trend
of
increasing risk
with
increasing
weight
was detected(P
for
trend <0.05).
Farnily
history
of
breast cancer, history
of
benign
breast disease, ages at menarche and menopause,
lac-tation,
drinking
habits andheight
were notsignificant-ly
related
to breast cancerrisk.
DISCUSSION
In
our study, there
is
one
important
methodological
lirnitation.
Our
control
seriesrnight
rnoreprevalêntly
include women
with
benign breast disease than generalfemale
population,
becausewe
selected,though
ran-domly,
thecontrols from women
who soughtforbreast
examination at the
department
of
breastsurgery
andwere later
proved not to
have breastanllcer.
Accord-ingly,
when
apotential risk factor for
breast cancer ispositively
associated
with
the risk
of
benign
breast disease,then
theRR
obtained
for
such afactor rnight
be
conservative.
Conversely,
therisk
for breast cancermight
be over-estimated, when
apotential risk
factor
for
breast cancer
is
negatively
linked
to
the risk of
benign
breast disease.Farnily
history
of
breast cancer
is
cottsisteutly
in-crirninated
as arisk factor for
female
breast cancer.lSOur failure
in
finding
an association between
breastcancer and
family history
may
bepartly
ascribable tothe excessive
inclusion of
wornen
with
benign
breast diseasein
our control
series,
since family history of
breast cancer is
knowu
to bepositivelv
associatedwith
the
history of
benign
breastàir"ur".27'28
Both early
menarchel'5'9-12 andlate
menopause2-4'10' l1'13 arewell-established
risk factors.
In
Jàpan,how-ever,
significant
relevance
of
early
rnenarche and late lnenopauseto
breast cancer
risk
hasnot always
been detected,S'19likewise
our study.
Decreasing
risk of
breast caucerwith
increasing
dura-tion of
rnenstrual
cycle
hasbeen
suggestedin
some stuclies,l'29 asclid
our
study.
We
foùna
asignificant
association
between regular
rnenstrual
cycle
and
anincreased prernenopausal breast caucer
risk, but
this
was
not
detected
in
previous
studies.l9
Thesetwo
particular findings on mer$truation
tnay suggestively
indicate that
breastcancer
risk
appearsto
be
directly
related
to
thecumulative number
of
regular
ovulatory
cycles.29'30
I-ate
age atfirst
birth/full-term
pregn4qcJ_is.known tobe linked
to
breast cancer
ri;k.r'3-6'8'q'12'14'15
our
study
also detected asignificantly
larger
RR for
later
age
at first
birth,
particularly
in
postmenopausal
women.
Several recent studies
have noted that frequent
full
term
pregnancyor
birth
has aprotective
effect
against breastcancer, independently
of
ageat first birth/full
term pregnancy.l'10'14
In
our sùdy
also,
an
inde-pendent and
significant
trend
of
decreasing
risk with
increasing
number
of
livebirths was
observed,
par-ticularly
in
premenopausalwomen. This finding
may
essentially
indicate that
a recently
increasing
breast cancer incidence in Japan ispartly
related to therapidly
declined
birth rate.'r
Premenopausal women
who
had ever lactated werenot
found
to
be at a significantly smaller
risk of
breast cancerby
themultivariate
analysis.An
association between
smoking habits and
breastcancer
risk remairs
inconclusive. Most
studies
have founclno clear
association,3'8'20'22while
some
inves-tigators
have suggested anunfavorable effect of
smok-ing
traUitson
breast.un
"r.r9'21
In
the
present study,smokiug
habits wasfound
to be associatedwith
breastcarcer risk, likewise a previous study
conducted
in
Nagoya,
Jupuu.lg
The
RR for
current smokers
in
our
study, particularly
in
postmenopausal
women, might
be
over estimated, possibly
dueto
the
potentially
ex-cessivenumber
of
women
with
benign
breast diseasein
our
controls, since benign breast disease
was reported asnegatively
associatedwith
smoking
habits in postrnenopausal wàme n.28'32In
our study, wefailed
to detect dose-response
relationship
between thenum-ber of cigarettes smoked per day and breast cancer
risk.
A
positive
associarion berween
atcohol -"i},Tp,rtjlrtÀ
and breast cancer has been reported
in
many, :but not
all,2'5'ts'to epidemiological
studies.
The preseutstudy,
however,
did not show
a
significantly
larger RR
for
current drinkers.
Obese
women
were
at significantly
greater
risk
of
postmenopausal breast cancer,
which
isin good
a9ree-ment
*itn
previous
finaings.l'8'1fi6'17
"
In
prelnenopausalwomen,
asignificant
trend
of
increas-ing
breast cancerrisk
with
increasing
weight
was
ob-served. This findiug might,
however, be attributable
to
excessiveinclusion of
benign
breast diseasein
our
Vol 4, No 3, July - September 1995
prevalent
in
prernenopausal
worneu and obesity
isnegatively
associated
with
the
risk
of
this
dis-ea;e.27 '28'13
Several
studies have
reported
a positive
associatioubetween height and fernale
breasi.un""r,l1'34
but
wedid
not
find
such an association.CONCLUSION
Our study disclosed the
following
rnajor
findings:
(a)the rnore the nurnber
of
livebirths, the smaller
thefemale breast cancer
risk,
particularly
in
prernenopausal
women; (b) in
premenopausalwomen,
regular rnenstrual cycle
significantly
increased
therisk,
audits increasing duration
decreaserl therisk;
(c)
current
srnokers experienced asignificantly
larger RR,particularly
in
postmenopausal wornen;
(d)
obesewomen
were
at a significantly
greater
risk
of
postmenopausal
breastcancer; (e) the later the
age atfirst
livebirth, the higher the
postmenopausal
breastcancer
risk;
(f)
family history
of
breast cancer,history
of
benign
breast disease, ages
at
menarche
andlnenopause,
lactation,
drinking
habits andheight
wereindependently
not associatedwith
female breast cancerrisk.
Acknowledgments
The authors are
grateful
to the nurses andpublic
healthllurses
for
excellent
care
aud data collection
of
thebreast
callcer
cases andcontrols.
This
work
was supportedby
theMinistry of
Education
and Culture,
Japan, Grants
No.
01042007
and
04042013; and was
partly
supportedby
theIndonesian
Caucer
Fouudation. This collaborative
study was a partof
Special Cancer
ResearchProject
in
Monbusho
[n-ternational
Scientific
ResearchPrograrn,
with
theap-proval
of
the Dean,Faculty of Meclicine,
University of
Indonesia, No. 4383ÆT02.H4.FIÇE/88.
REFERENCES
1. Yuan JM, Yu MC, Ross RK, Gao
yT,
Henderson BE. Risk factors[or
lrreast cancerin
Chinese womenin
Shanghai.Chncer Res 1988;48: I 949-53.
2. Rosenberg L, Palnrer JR, Miller DR, Clarke EAn Shapiro S.
A case-control study ofalcoholic beverage consumption and breast cancer. Am J Epideuiol 1990;13l:6-14.
3. Nasca PC, flaptiste MS, Fielct NA, Metzger BB, Black M,
Kwon
(5,
et al. An epidenriological case-control studyof
breast cancer aod alcohol consunrption. Int
J
Epidenriol l99O;19:532-8.4. Sega la C, Gerber M, Richa rclsoo S. The pa ttern of risk factors for breast cancer in a southern France population. Interest
Breast Cancer Among Japanesse
Women
181for a stratified analysis by age at diagnosis. Br J Cancer l99I;64:919-25.
5. Simon MS, Carman W, Wolte R, Schorrenleld D. Alcohol consumption and the risk of breast cancer: a report from the
Tecumseh Community Health
Study.
J Clin
Epidemioll99l;44:755-61.
6. Ferraroni
M,
Decarli A, Willett WC, Marubini E. Alcohol and breast cancer risk: a case-control study from northernIraly. Inr J Epidemiot I99t;20:859-64.
7. Yoo KY, Tajima K, Kuroishi T, Hirose
[i
yoshida M, Miura S, et al. Independent protective effectof
lactation againstbreast cancer: a case-con trol study i n Ja pan. Am J Epidemi ol 1992;135:726-33.
8. Kato l, Miura S, Kasumi F, Iwase T, Tashiro H, Fujita
y,
etal.
A
case-control study of breast cancer among Japanesewomen:
with
special referenceto family
history
andreproductive and dietary [actors. Breast Czncer Res Treat 1992;24:51-9.
9. Bouchardy C, Lê MG,
Hill
C. Risk factors [or breasr canceraccording to age at diagnosis in a French case control study.
J Clin Epidemiol 199O;43:261-75.
10. Yu SZ, Lu RF, Xu DD, Howe GR. A case-control study
of
dietary and nondietary risk factors [or breast cancer inShan-ghai. Cancer Res 1990;50:5}11-ZI.
11. Hsieh CC, Trichopoulos D, Katsouyanni K, yuasa S. Ageat
menarche, age at menopause, height and obesity as risk factors for breast cancer: associations and interactions in an i nternational case-con trol study. In t J Ca ncer 199O;46:7 96-800 .
12. Gapstur SM, Potter JD, Sellers TA, Folsom
AR.
Increasedrisk
of
breast cancerwith
alcohol consumptionin
post_menopausal women. Am J Epidemiol 1992;136:1221_31.
13. TandzeD, Lifanova Y, Maximovitch D, Day NE, Duffy SW.
Diet, alcohol oonsumption and reproductive factors
in
acase-control study of breast cancer i n Moscow. Int J Ca ncer
l99l;48:493-5O1.
14. Ewerz M, Duify SW, Adami HO, Kvâle G, Lund E, Meirk
O, et
al.
Age at first birth, parity and risk of breast cancer: ameta analysis of 8 studies from the Nordic countries. Int J
Cance.r 199O;46 : 597 -6O3.
15. la Vecchia C, Negri E, Franceschi S, parazzini F. Long_rerm
impact
ol
reproductive factors on cancerrisk.
Int J Cancer1993;53:215-9.
16. Parazzini F, la Vecchia C, Negri E,Bruzzi p, palli D, Boyle P, et al. Anthropometricvariables and risk oIbreastcancer. Int J Cancer 1990;45:397-4O2.
17. Sellers TA, Kushi LH, porter JD, Kaye SA, Nelson CL, Mc
Govern PG, et al. Effecr ot lamily history, body-far distribu_ tion, and reproductive factors on the risk of postmenopausal breast cancer. N Engl J Med 1992;326:1323-9.
18. Howe G, Rohan
T,
DecarliA,
Iscovich J, Kaldor J, Kat_souyanni
K,
etal. The association between alcohol
and breast cancer risk: evidence from the combined analysisol
six dietary case-control studies. Int J Cancer l99L;47:7O7_
10.
19. Yoo KY, Tajima
li
Kuroishi T, Hirose K, Miura S, MuraiH,
etal.
Lit'e-style in relation to the risk of breast cancer. JEpidemiol 1992;2 (Suppt) :S 155-65.
20. Rohan TE, Baron
JA.
Cigarette smoking and breast cancer.21. Chu SY, Stroup NE, Wingo PA, Lee NC, Peterson HB, Gwinn
ML,
et al. Cigarette smoking and the risk o[ breastcancer. Am J Epidemiol 199O;13I:244-53.
22. Fielcl NA, Baptiste MS,
Nasq
PC, MetzgerBB.
Cigarettesmoking and breast cancer. Int
I
Epidemiol 1992:21t842-8. 23. The Research Group [or Population-based CancerRegistra-tion.
Cancer incidence in Japan, I975-1979. Osaka: TheOsaka Cancer Registry, 1984.
24. Research Group for Population-based Cancer Registration in Japan. Cancer incidence and incidence rates in Japan in 1985-Estimates based on data from seven population-based
cancer registries. Jpn J Clin Oncol l99O;2O:212-8. 25. Breslow NE, Day
NE.
Unconditional logistic regression forlarge strata. In Davis W edi tor. Statisti ca I Methods in Cancer Research,
vol
l.
Lyon: IARC, lS80:192-246.26. Rothman KJ. Modern Epidemiology. Boston: Little, Brown
and Company, 1986.
27. Pastides
H,
KelseyJL,
Hollord TR,
LiVolsi
VA.
Anepidemiologic study of [ibrocystic breast disease with
reier-ence
to
ductal epithelial
atypia.
Am
J
Epidenriol1985;,121:44O-7.
28. tserkowitz GS, Kelsey JL, LiVolsi VA, Hollotd TR, Merino MJ, Ort S, et
al.
Risk factors for fibrocystic breast diseaseand
its
histopathologic components.J
Natl
Cancer Inst 1985;75:43-50.29. Olsson
H,
tandin-OlssonM,
GullbergB.
Retrospectiveassessment of menstrual cycle length in patients with breast cancer, in patients with benign breast disease, and in women without breast disease. J Natl Cancer InsT 1983;70:17 -20.
30. Henderson BE, Ross RK, Judo HL, Krailo MD, Pike MC.
Do
regular ovulatory cycles increase breast cancer risk?Ca ncer 1 985;5 6: 12O6 -8.
31. Ministry of Health and Welfare of Japan. Vital Statistics of
Japan 1991, vol 1. Tokyo: Kousei Toukei Kyoukai, 1993.
32. Berkowitz GS, Canny PF,
LiVolsi
VA,
Merino MJ,O'-Connor TZ,Kelsey JL, et
al.
Cigarette smoking and benignbreast disease.
J
Epidemiol Community
Health1985;39:308-13.
33. Yu H, Rohan TE, Cook MG, Howe GR,
Miller
AB.
Risk factors for fibroadenoma: a case-control study in Australia. Am J Epidemiol 1992;L35:247-58.34. Vatten
LI,
Kvinnslaird S. Body heigbt and riskol
breast