I, No l,
Jtttttrrtrl
Murtlt 1994
Antibiotic GuidelinesAntibiotic
Guidelines
:
Pharmacological Parameters to
be
Considered
I
Darmansjah
,RHH Nelwan
Abstrak
Tujuan pedoman penggunaan antibiotik adalah untuk membinbing penggunaannya secara rasional, sehingga antibiotik digunakan secara efektifdan efisien dengan efek satnping sekecil-kecilnya bagi penderita dan nasyarakat. Tindakan inijuga berdatnpak mengurangi biaya tanpa mengorbankan penderita,hnasyarakat terhadap penilihan antibiotikyang salah. Pedotnan ini harus mernenuhi
persyaratan tertentu agar dapat diterima oleh pemakainya dan berlaku bagi sebagian besar (kira-kira 9O%) kclotnpok penderita. Antibiotik
terpilih
yang diusulkan harus efektif tanpa adanya hasil antibiogratn. Pedomanini
harus berdasarkan pengetahuan mikrobiologi, fannakologi dan klinik. Paratneter farnakologi yang akan dibahas antara lain adalah fannakodinatnik, fannakokinetik,efekbksik dan efek samping, hasil uji klinik, percobaan epidemiologi obat sertafarnakolctgi perbandingan antibiotik. Strategi petnilihan teruta,na berdasarkan penerapan rasio nanfaat-risiko serta biaya; nanfaat antibiotik yang diperkirakan untuk indikasi tertentu harus lebih besar dari kemungkinan risiko yang dapat ditimbulkannya. Prinsip "Priuutn non nocere" haruslah merupakan pertùnbangan utana. Antibiotik sering menimbulkan efek satnping dan karena penberiannya perlu bertujuan
jelas.
Menganggap bahwa "bila tidak berefek tentunya tidak berbahaya" tidaklah benar. Pedontan bukanlah suutu aturan yang kaku; pertimbangan iltniah harus selalu merupakan petunjuk akhir, terutatna pada keadaan klinik yang konpleks. Pedonan pemilihan antibiotik perlu diperbaharui terus ,nenerus bilatnana ada infonnasi yang baru. LaTitnnya tidak perlu ada sanksi terhadap penyinpangan kecil dari pedotnan yang ada, namun penyitnpangan jauh dari suatu pedoman menerlukan dasar ilniah yang jelas.Abstract
The aim of antibiotic guidelines is to provide guidance on the rational use of antibiotics, so that they serve effectively and eficiently with the least adverse effects on patients and co,n,tturtity. Tlrc iupact of such strategy nny also be seen in the containtnent of cost without ieopardizing the patient to un-successful atteupts of antibiotic treatnent. Guidelines have to satisfy certain requiretnents in order to be accepted by its users. It should workfor the majority (approx.go%) of patient groups and the antibiotic selectiorx suggested should be effective without or before the results ofantibiograns. Antibiotic guidelines nust be based on nicrobiological, phannacological and
clinical
knowledge. Among phannacological parantetersof
the antibioticthat will
be discussed are pharmacodynanics, phar-macokinetics, toxicity and adverse effects, results of clinical trials and drug-epideniological studies, and the conparative phannacology of antibiotics. The main strategyfor
selection is based on benefit-risk-cost csscssrlent; the presu,ned benefit that the antibiotic couldoffer
for
a certain indication should be greater that the possible risksit
conld give rise to. The principle of treatnent: "Pritnum nonnocere" should always be a
prior
consideration.In
this respect the great potential of antibiotics to cause adversity is very oftenoverlooked, causing the erroneous attitude of "if it does not work, it does not harn either". Guidelines.are neyeruneant to be rigid rules; scientific judgetnent should always be the
final
guide, especially in complicated clinical conditions. Renewal of choices of antibiotics should be instituted whenever recent infonnation is available and updating of an antibiotic guideline is nandatory every year or two.Usually there are no sanctions
for
violating good advice, but najor deviations frotn guidelines nust be scientifically justifiable.Keywords : Antibiotic use, Antibiotic selectiotr, Ratiornl use
INTRODUCTION
The aim of guidelines
for
antibiotic-use
is to provide
guidance on therational
useof antibiotics,
so thatthey
serveeffectively
andefficiently with
the least adverseeffects
onpatients
andcommunity,
and that resistanceof microorganisms could
beminimized,l'2
The impact
of such strategy may also
be seenin the containment
ofcost withoutjeopardizing
the patient to unsuccessfulantibiotic
treatment.Antibiotic
guidelines
set general guidanceonhow
antibiotics should be correctly used.
It
gives
sugges-Department of Pharmacology, Faculty of Medicine University of Indonesia, Jakorta, Indonesia
Darmansjah and Nelwan
tions
on the bestantibiotic
choice
(s)available
for
thetreatment
and prophylaxis
of bacterial,
fungal
andparasitic
infections.r
Guidelines
have tosatisfy
certain requirementsin
order to be acceptedby
its users.It
shouldwork
for
themajority
of patient population
and theantibiotic
selec-tions
suggestedshould
beeffective without
of
before
the results
of
sensitivity
testings. The
majority of
in-fections in fact
may be treatedwithout
the necessityof
doing
any
culture of
aninfected
biological
specimen.Therefore
antibiotic
guidelines must be
basedon
theintegration
of
microbiological, pharmacological
andclinical knowledge; the results
of
clinical trials
andepidemiological
studies
especially should
determine
the
validity of
the selections made.Not
to beunderes-timated
is
the
value of
a
correct diagnosis
before
prescribing
anantibiotic
in
order todistinguish
the real needsfor
eradicating
or
preventing
aninfection.
Fur-thermore, guidelines should be
updated
or renewed
whenever new knowledge
becomesavailable.
GENERAL CONSIDERATIONS
Among pharmacological
parameters that areimportant
to
beconsidered are
:pharmacodynamics,
pharmaco-kinetics, toxicity
and adverseeffects
of
the
antibiotic
underscrutiny,
siteofinfection,
special effects onhigh
risk patient group
in
relation
to
the antibiotic
being
considered,
results
of
clinical trials,
drug-epidemio-logical
studies, and above
all,
the comparative
phar-macology of all antibiotics, especially
of thosebelong-ing to
the same class.The
main
strategy
for
selection
of
atreatment
is based onbenefit-risk-cost
assessment; the presumedor
calculated
benefit that
an
antibiotic could offer
for a
certain indication
should
be
greater that
the
possiblerisks
it
could give rise
to.
The
principle of
treatment
:"Primum
non nocere",
which broadly
means
"do
not
harm when
treating patients", should
always be aprior
consideration.
Cost should only be
decided
after
all
scientific
judgements
have been made andtreatment-cost
should
beput before drug-unit-cost. When
two
or
more
antibiotic
selections can be
madewith
more or
lesssimilar
predicted outcome,
then cost should be thedetermining factors,
As
for
each
guideline,
it never should be
con-sidered
asrigid
rules; sound
scientific
judgement
anda scientifically
based
selection
for
using
antibiotics
should always be the
final
guide.But, major deviations
from
guidelines must
bescientifically justifiable,
be-cause goodguidelines should apply
for
themajority of
subjects for
whom
the
guidelines are
developed,
Guidelines
also should takeinto consideration
thelevel
Med
J
Univ ltrdonof
competenceof
thehealth service
andprescriber
for
which
it
is meant;while
gentamicin
is a goodantibiotic
to
be usedin
ahospital setting where
the closeobser-vation
of
the patient
is
neededand where
monitoring
of
antibiotic blood levels may be determined, in
aprimary
health setting
it
may
be dangerous.PHARMACODYNAMIC
PARAMETERS
Antibiotics
areusually
chemicalswith
no orlittle
phar-macodynamic properties; they
donot
exertsignificant
actions
on
the organs of the host.
This
is
a
goodcharacteristic
of
anantibiotic,
becausethey preferably
should
only
have
killing
properties on the
invading
microorganisms
without
doing
harmby
stimulating
or
inhibiting
other receptorsof
thehost.
Someantibiotics
however, may
haveactions
onintact
human organsor
give rise to
effects
that
are
adversein
nature, and
assuch
may
limit
the
use
or
dose
of
an antibiotic.
Ex-amples of suchantibiotics
are theaminoglycosides
thatinhibit
neuromuscular conductions
whenadministered
in high
doses.This curariform-like
effect is
seenwith
streptomycin, kanamycin, gentamicin, neomycin,
andprobably other aminoglycosides
in high
doses.When
used
with
other muscle relaxants
this
effect
will even
be
enhanced.
Circumoral
paresthesia
is also
well-known
with
drugs
like
streptomycin;
and vestibular
dysfunction occurs
with
relatively
high
therapeutic
doses.Other reactions may be seen
with
antibiotics,
such asbone-marrow depression
with
chloramphenicol
or
cephalosporins,
hypoprothrombinaemia
with
moxa-lactam, etc.
Thesemay not
beregarded
aspharmaco-dynamic
becausethey occur seldom
and areonly
seenwith very high
dosesor
are a
result
of
idiosyncratic
reactions and aretherefore unpredictable
for
anygiven
patient.
Phenotyping
and genotyping
of
the way
in-dividuals
dometabolize
certain drugs may in thefuture
determine
which
patient
would
beprone
to
the abovementioned
adverseeflects.a')
The
pharmacodynamic
effects on the
micro-or-ganisms
arereflected
in
the eradicating properties
of
the
antibiotic itself; the may be bactericidal or
bac-teriostatic. The
degreeof
eradicating
abilities
may
be expressedby
the
minimum inhibitory
concentrations
(MICs)
of
theantibiotic. While
this simple
in vitro
testis
an
important
parameter,
it
mty
not
be used
as thesingle
determinant
to
select an
antibiotic
for
therapeutic
or prophylactic
purposes, becausein vivo
conditions
do not always produce the same results. Theclinical
evaluation
of the patients must always betaken
into
account.htl
.1, No I,Jtutuurt
Marclt 1994may be
divided into
groups
of
microorganisms.
Thusthere
areantibiotics
that
mainly
attack Gram positive
bacteria such
as
benzylpenicillin,
phenoxymen-thypenicillin, cloxacillin
or
flucloxacillin,
erythro-mycin, spiraerythro-mycin,
andother macrolides. The
fluoro-quinolones are
more specific
against
Gram
negative
bacteria and although
it
may
be
active
against Gram
positive cocci,
it
is not to
be used
when the
narrow
spectrum
antibiotics
aresensitive
to
it
andtherefore
fluoroquinolones are
not
recommended
as the first
choice
for
definite Gram positive infections
such
asstreptococcal
or
staphylococcal.
In
a group
however
the antibiotics may
have
individual specific
actions;gentamicin
for
instance
would be
more effective
against pseudomonas
than
kanamycin,
and
thecephalosporins
may have different
emphasis
on
an-tibacterial
activity
according
to the time
of
develop-ment
of
this
classof
drugs during
the last 20 years.PHARMACOKINETIC
PARAMETERS
First
it
must be
ascertainedthat the
antibiotic
chosenis
absorbedby
the proposed route
andis
available
atthe site
of infection in
therequired concentration in its
active
form.
Many antibiotics, although having
anade-quate
MIC
may
not qualify
for
some
of
the
other
parameters
mentioned
andtherefore may not
produceclinically
good results.Orally available antibiotics such
as macrolides
(erythromycin, spiramycin, etc), lincomycin,
certain
beta-lactams
like
ampicillin
and
phenoxymethyl-penicillin
are
incompletely
absorbed.
Despite their
clinical
usefulness
it
may
not
produce sufficient
enoughantibiotic
concentrations
in
certainindividuals
to rely on in
severeinfections
when given
by
mouth,
especially when taken
with
food. Injectable
dosageforms
are mostappropriate
whenhigh
antibiotic
levels
are required immediately, such as
in
contaminated
surgical prophylaxis.
Tissue
levels
of
an
antibiotic
is
an
important
parameter
for clinical efficacy;
somemay show
rela-tively
high
concentrations
at the site
of
infectjon
despite
a
low
bioavailability
(spiramycin,
azithro-mycin).
Chemical
configuration of
the
antibiotic
may determine thisproperty; fat-soluble antibiotics, having
higher
afinity
to tissue,
will
passcell-membranes
andthe blood-brain
at
greater ease
(clindamycin
versuslincomycin).
Other
important
pharmacokinetic
parameters are:
speed
of
absorption, peak and trough levels,
con-centration
half-lifes, formation
of
active metabolites,
and
pathways
of
excretion,
Antibiotic Guidelines
SPECIAL PRECAUTIONS
There are
special precautions
that
need
to
be
taken
when choosing
antibiotics in
patients
with
thefollow-ing characteristics
:*
thepremature
babies and thegeriatric
patients*
child-bearing women
andnursing
mothers*
organdeficient
patients,especially
organs ofexcre-tion (liver,
gastrointestinal tract,
andkidney)
*
specific
diseases*
patients who are
on
concomitant treatment with
drugs
that
are incompatible
with
the
antibiotic
given.
ADVERSE EFFECTS OF
ANTIBIOTICS
Although
antibiotics may
belife-saving
when needed,it
may produce
adverseeffects that
arenot to
be
dis-regarded. These side
effects rank
among the highestin
frequency.of
all
drug
classes.It
may
therefore
mini-mize
the usefulnessof
the
antibiotics
prescribed.
Ad-verse reactions
varying from skin
rashes, nausea andabdominal
discomfort (the most frequent)
to
blood
dyscrasia,
hepatitis
andfatal anaphylactic
reactions arewell
known. The propensity
of
one
antibiotic giving
morefrequent
adverse reactions that another should betaken
into
account
in
theselection
process.An important fact
to be considered is thefrequen-cy of
useof
acertain
antibiotic;
the morefrequent
it
isused the more adverse reactions
it
will elicit.
Assuming
the incidence
rates
of
adverse reactions
to
a
certain
antibiotic
tobe
constant, the absolute numberof
caseswill
therefore increase and become noticeable
as theantibiotic
is used morefrequently.
Two
examplesmay
highlight
this
statement.When
in
earlier
yearspenicil-lin
G procaine injections were
socommon
thatalmost
every other patient got
apenicilline
shot,anaphylactic
reactions were rampant.
Although
most of
theseinjec-tions
weregrossly inappropriate
andtherefore did
only
contribute falsely
to
cure,
this practice went on for
more than
2
decades. Some caseswith fatal
outcome
at last brought a drastic
change
becauseof
casesof
litigation. Although it
strangely
endedwith
theverdict
"not
guilty",
thepractice of
penicillin
injections
disap-peared andnow
70%
of primary
health
centres donot
even use
penicillin uny
-or",u
a
phenomenon
to be
deplored.
This
suggeststhat
if
antibiotics
were
usedmore appropriately, fever
patients
would
have
beeneligible
for
penicillin
injections
with
a
resultant
decrease in the numberofadverse
effects. The opposite happenedwith flucloxacillin;
a
total
of
I79
casesof
hepatitis
associatedwith
the
useof flucloxacillin
has been reported to theAustralian Drug
AdverseReaction
Darnnnsiah and Nelwan
widely promoted
in the Australian Antibiotic
Guide-lines'
as the drug
of
choice against staphylococcal
infections. The resultant
steep increaseof its
use hascaused
a
drastic rise
of flucloxacillin
associated
hepatitis which
in turnmight
notjustify
thebenefit-risk
equation
for using flucloxacillin routinely
any
more. Theindication for flucloxaccillin
use hasrecently
beenlimited
to include only
severe staphylococcal
infec-tions,
andcaution
was mandatedwhen presribing
the drugfor older
people or when the drug is usedfor
morethan
14 days.RESULTS OF
CLINICAL
TRIALS
The results of clinical trials
are theultimate "proof of
the pudding", that the antibiotic is
efficacious
for
aspecific indication.
However, the accessability
of
theresults on several clinical trials to make
aninformed
judgement on the profile
of
an antibiotic
is
usually
scarce.
The information is
scatteredin
manyjournals
andcontradictory results
aredifficult
to unify,
not
the least becauseof the industry's promotional activities
in
the
form
of
seminars and literature.
Evaluated
textbooks should
give
anobjective
view
on
theprob-lem.
The American Medical Association's Drug
Evaluationse is
anannual which is
anobjective guide
for selecting drugs
including antibiotics;
it
describesdrug
classesand individual drugs. Another book
en-titled Therapeutic Drugslo
i,
rnonogruph that has beenpublished recently; each monograph deals,
among others,with "Major
outcometrials" which
describesin
a
nutshell
the resultsof important
clinical
studies. Thegeneralizability
or externalvalidity
of suchtrials,
how-ever,
aresometimes difficult to
assess.Therefore
an-tibiotic
guidelines
would
bevery
useful in the
every-day application
of
thesepotent
drugs. Studios,involv-ing
largerpopulations,
such asin
drugepidemiological
research are also
valid to supplement
thesmaller
scaleclinical
trials.
LEGAL
ASPECTS OF AN ANTIBIOTIC GUIDE.
LINE
The
statusof
ascientific
guideline should
necessarilydeal
with scientific
issues. Some may have the idea thata
guideline of this sort should
also bethe
standardof
measure
when
one is confronted
with legal
implica-tions when deviaimplica-tions
from
it
become
a
matter
of
dispute in
alitigation
case.'We
must emphasize
that the legality
for
such
purpose cannot be
fully
attributed
to
an antibiotic
guideline
or any othertreatment guidelines. Treatment
modalities
are acomplex subject
andadhering simply
Med
J
Univ Indonto
aguideline may
sometimes be erroneouswhen
oneis confronted
by a complex situation or ramification
which
necessitates oneto deviate
from
aguideline.
It
may however
not be
assumedthat
aguideline
can beviolated any
time
for
invalid
reasons.
One
may
reasonably speculate
that a
guideline
works
for
themajority
(907oor more) of
cases,but
if one
departssubstantially
from
it
there must be valid
reasonsto
justify one's
choice.In
acourt
casewhere
drugsmight
have caused injury or death
to
a patient, there
will
usually
be one or more expertswho will testify whether
the treatment had caused the
injury.
But
even thenit is
not easy to establish
causality
asit
wasexemplified by
the "Bendectin
case"recently in
anAmerican
Court-roo..ll
Bendectin is an antihistaminic
used
againtsvomiting in early pregnancy
that was on theAmerican
market
from
1956
until
1983, when
it
was
bannedbecause
of
accusations
that
it
may have
causedphocomelia
in 2
cases.The Court
acceptedonly
peerreviewed
journals as "good science" and in 1991
aCalifornia
appealscourt
rejected theparent's suit. This
was challenged
by other scientists and the
SupremeCourt
will
reopenthe
case atthe time of this writing.
The problem
becomesmore entangled
becauseof
theihvolvement
of
the notorious American lawsuit
onhealth related matters
andnot the
least,the
statementmade
that
"
'experts'
will
testify
to anything,
for
a.
,,tl
pnce
QUICK
REFERENCE
FOR
ANTIBIOTIC
IN-DICATIONS
It
may be useful
to
design a quick reference
in
atable-form
in
which
diseases are matched
with
theappropriate
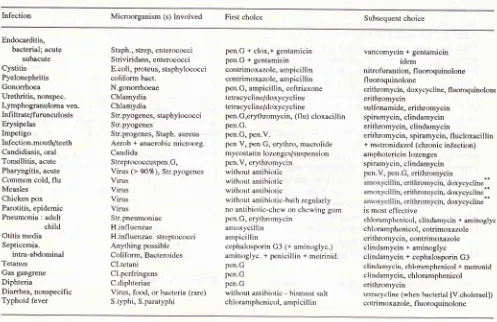
antibiotics. Table
I
depicts
such a
guidance;
afirst
and subsequentchoice is provided to
accomodate
for situations in which
thefirst
one cannot be used.This gives
afirst impression on what to
useroutinely
before
going into the details
of the clinical
condition.
It will
serve
the reader
with a useful
an-tibiotic
tostart with, which
is correct according to
theauthors' view
at thetime of this publication.
It
must beemphasized however
that in
making the final
judge-ment,
many
of the abovementioned
parametersshould
be taken into
consideration,
This guideline should
beused in
conjunction
with
other(authoritative) literature
so that nuances caused
by
individual
conditions
ofthe
patient
can be accomodated.There are
certain
generalprinciples
that areincor-porated
into this model guideline,
someof them
are :a.
Vy'henantibiotic
treatment has beeninitiated before
an
antibiogram is
madeand clinical improvement
Vt;l 3, No l,
Jurtuury
Murch 1994Table
l.
Antibiotic Choice In Selected Infections*Antibiotic Guidelines
lnfection Microorganism (s) Involved First cholce Subsequent choice
Endocarditis, bacterial; acute
subacute
Cystitis
Pyelonephritis Gonorrhoea
Urethritis, nonspec.
Lymphogranuloma ven. Infi ltrate/furunculosis
Erysipelas
Impetigo
Infection.mouth/teeth
Candidiasis, oral
Tonsillitis, acute
Pharyngitis, acute
Common cold, flu Measles Chicken pox Parotitis, epidemic Pneumonia : adult
child Otitis media Septicemia.
intra-aMominal
Tetanus
Gas gangrene
Diphteria
Dianhea, nonspecific
Typhoid fever
Staph., strep, enterococci
Striviridans, enterococci
E.coli, proteus, staphylææci coliform bact.
N.gononhoeae
Chlamydia Chlamydia
Str.pyogenes, staphylococci Str.pyogenes
Str.progenes, Staph. aureus
Aerob + anaerobic mictrnrg. Candida
Strept(rcoccuspen.G,
Virus (> 9O%), Str.pyogenes
Virus Virus Virus Virus Stt.pneumoniae H.influenzae
H.infl uenzae- streptococci
Anything possible
Coliform, Bacteroides CI.tetani
CLpcrfringens
C.diphteriae
Virus, ftxxl, or bacteria (rare)
S.typhi, S.paratyphi
pen.G + clox,+ gentamicin pen.G + gentamisin contrimoxazole, ampicillin contrimoxazole, ampicilli n
pen.G, ampicillin, ceftriaxone tetracycline/doxycycl ine tetracycline/doxycycl i ne
pen.G,erythromycin, (tlu) cloxacil lin
pen.G. pen.G, pen.V.
pen V, pen G, erythro, macrolide mycostalin lozenges/susJnnsion pen.V, erythromycin
without antibiotic without antihiotic without antibiotic
without antibiotic-bath rcgularly
no antibiotic-chew on chcwing gum pen.C, erythromycin
amoxycillin ampicillin
cephalosporin G3 1+ arn1n,rt;t".,
aminoglyc. + çrenicillin + metrinid.
pcn.G
pen.G
pen.G
without antibiotic - bismust salt chloramphcnicol, ampicillin
vancomycin + gentamicin
idem
nitrofurantion, fl uoroquinolone
fluoroquinolone
etithromycin, doxycycline, fl uoroquinolone
erithromycin
sulfonamide, eritfuomycin
spiramycin, clindamycin erithromycin, clindamycin
erithromycin, spiramycin, flucloxacillin
+ metronidazol (chronic infection)
amphotericin lozenges
spiramycin, clindamycin
,
cinr
, doxycycline**r
, doxycycline*.r
, doxycyclineis most effective
chloramphenicol, clindamycin + aminoglyc chloramphenicol, cotrimoxazole crithromycin, contrimoxazole
clindamycin + aminoglyc clindamycin + cephalosporin G3 clindamycin, chloramphenicol + metionid cl indamycin, chloramphenicol
erithromycin
tettacycline (when bacterial [V.choletael]) cotrimoxazole, fl uoroquinolone
Adapted from Katzung B, ed. Basic and Clinical Pharmacology,4th etl., 1989:619-21, Gllman AG, Gu.xlman LS, Rall TW, Muracl F, ed.
ThePharmacologicalBasisofTherapeutics,8thed., 1990, l}24-33,and AnlibioricGui<ielines,6therllggg-gl,HealrhDepartmentofVictoria, Australla.
** Only when secondary Infection is evident
not
to change
the antibiotic
initially used
for
another
that
was
more sensitive
according
to
theantibiogram
results. These results may be usedlater
when
thefirst
treatment fails.
The
local
experience based onscientific judgement
and the
local
sensitivity
patternof
pathogens tested must be takeninto
account whenmaking
antibiotic
selections. When recent sensitivity patterns
arelacking, Table I
may
be used as a guide.Ampicillin
may
beinterchanged
with amoxycillin,
while cloxacillin with flucloxacillin, without
caus-ing significant clinical
outcome.Although penicillin
G danpenicillin
V
havealmost
the
sameantibiotic
spectrum,
penicillin
V
should
never be used
for
seriousinfections.
Its action is tooweak
andaborption
of
thedrug is
limited,
so that ahigh concentration
in
theblood
cannot be attained.Different
macrolides may be used interchangebly
for
the
indication
cited
in
the
table. Although
erythromycin
is
the
prototype and is
the
most
studied,
it
may
causeunbearable gastric
irritation
for
some patents.
Other
macrolides
may
be more
tolerated by
the stomach.It
should
always begiven
ll2
an hour before
meals
to
guarantee
adequateabsorption.
Cotrimoxazole
may
besubstituted
by trimetoprim
alone, especially
in
urinary tract infections.
The
sulfa component
in cotrimoxazole
gives rise
to
frequent
andsometimes serious
adverse reactions,while
the
efficacy of trimetoprim
alone
is not
dif-ferent.
When
mycostatin
lozenges are notavailable, it may
be
substituted
by
drops
or
syrup
or
even
tablets [image:5.595.58.555.97.419.2]h.
Dannansjah and Nelwan
mouth-wash;
the solution should be kept
in
themouth
for
afew
minutes.
The
viral infections listed in
the table should
nor-mally not
be treated
with
an
antibiotic, but
situa-tions may
arise where a
patient may
be
having
acomplication
with
a
bacterial
superinfection
eachtime
he/she
suffers
from
flu
and
in
this
case
anantibiotic
is well justified.
Lately,
epidemic
parotitis have
been treated
with
all
kinds
of
an-tibiotics
andisoprinosine. None
of these are
effec-tive
and
the
only
sensible
"treatment"
is to
give
chewing
gumto chew
on, sothat
themovement
of
the jaws
will
openthe
canal
of
the parotis gland,
thereby
draining
the
contents. Patientswith
chick-enpox should also take
abath
regularly with
soapand
water
so asto keep
the
skin
clean, preventing
secondary
infections. The use
of
potassium
per-manganate
in the
bath water is
redundant.Fluoroquinolones may not
be usedin
trivial
condi-tions,
and where otherantibiotics
arevery effective,
fluoroquinolones should
be reserved when the firstchosen
antibiotic
hasfailed to produce
satisfactory
results.
Finally,
guidelines
haveto
be regularly updated.Med
J
Univ IndonREEERENCES
l.
ParkerMT.
Antibiotic resistancein
pathogenic bacteria.WHO Chronicle 1982;36(5): 19
l-6.
2. Control of antibiotic resistant bacteria : Memorandum from
a lù/HO meeting. Am J Hosp Pharmacy L984;41:1329-31.
3. Antibiotic Guidelines 6th ed. 1990-1991, Victorian Medical
Postgraduate Foundation Inc. Australia.
4. Vessel ES, Pharmacogenetic perspectives : genes, drugs, and
disease. Hepatology 1984;4:959-65.
5. Weber WW, Hein DW, Litwin A, l.ower GM. Relationship
of
acetylator status to isoniazid toxicity, lupus erythema-tosus, and bladder cancer. Federation Proceedings 1983;42:3086-97.
6. Pudjiadi LL, Darmansjah I. Survei syok anaphylactik akibat
penisilin
G
di
Puskesmas, Jakarta.Maj
Farmakol Terapi Indonesia 1988;5:9- I2.7. Flucloxacillin hepatitis. Australian Adverse Drug Reactions
Bulletin 1992 February.
8. Australian Adverse Drug Reactions Advisory Committee.
Personal communication.
9.
AMA
Drug Evaluations, Annual 1993. American MedicalAssociation, Chicago, Illinois.
10. Dotlery, ed. Therapeutic Drugs Livingstone, 1992. London Churchill.
ll.
The meaning ofjunk. Newsweek 1993 March 29:42-4.