Vol 4, No
I,
January-March, 1995 Fragile X Mental Retardationt7
Fragile
X
Mental
Retardation
in
an Indonesian Family
Sultana,l
Ag.
Soemantri,2 P.R.L. Lam-Po-Tang,3 Fionu Wright,a Robert Lindeman,4 Stuart purvis-Smith3
Abstrak
Sindronnfragile X adalah petryakit retardasi nental nenurun yang paling unun dan dikaitkan dengan adanya 'fragile site,, pada
uiung akhir lengan panjang kromoson X. Dalan penelitian penyaringan untuk nencari kelainan krotnosottr
pada
siswa laki-laki retardasi mental dari sekolah luar-biasa, lcani pertatna kali nengidentifikasi keluarga dengan sindrotna fragite X di Indonesia pada pemeriksaanfisik, riwayat keluarga dan penteriksaan sitogenetila dan DNA nenbuktil<an dua kakak beradik laki-laki denganfenotip abnonnal, positif fragile X nasing-nasing 3%( Dn) dan 4%(Pù. Kakak perenpuan dan ibunya nenunjukkan fenotip dan intelektual nonnal, tetapi secarasitogenetikpositif untukfragileX(6% padakaknkperentpuandan3% padaibunya). Analisis nolekuler nte,akinkan bahwa kedua anak laki-lnki tersebut adalah penderita sindronafragile X, sedangkan kakak perentpuan dan ibunya adalah petnbawa srfaLAbstract
Fragile X syndrome is the nost cotnntonform
offanilial
nental retardation and is associated withafragile site
at the end of longarn
chrotnosonre X. Whilst screeningfor
chrontosoual abnornalities in nentally retarded nales attending special school, we have identifiedthefirst fanily
withafragile
x
syndrone, to be reported in Indonesia. ph1,sis.1 exatnination,fatnill, l1isg6r, as well as cyto9enetic and DNA studies identified tv,o pheno4,pically abnonnal brorhers who were fragile X posirive 3% (Dn) and 4% (pr). Their sister (Cl) and utother were pheno\,pically and intellectually nornalbut
were cytogenetically positive for fragile X (6% in the sister and 3% in lhe nother). Molecular analysis confirnted that both broîhers were afected and that their sister and tnother werecarriers-Keywords : Fragile
X
syndrone, ntental retardation, Indonesiry Javanese, chronosotne studies, restriction fragtnent length poll,norphisn, pfxa3.INTRODUCTION
Mental
retardation
(MR) is a
common
disease which isclinically
andetiologically
heterogenous.MR
can bedivided up according to intelligence quotient
(IQ)
test scoresinto
severe ormoderate (IQ
50 or less) andmild
(IQ 50-70),1-3
with
aprevalence
of
about 3
per
l0O0
for
severemental
retardation and
30per
IOOOfor
mild
mental retardalion.2
Causesof
mental retardation
in-clude obstetric problems, perinatal
trauma,
neonatalinfection and
genetic
abnormalities
such as
Down's
syndrome
(trisomy 21) and
X-linked
mental
retarda-tion (XLMR). Almost all surveys
of mentally
retarded persons show that males tendaffected
moreoften
than females.Of
all mentally
retardedpeople,
2O7o aredue
to
XLMR.a-6 About
4O7oof XLMR
and4%
of
all
mental retardation
have been
attributed
to
fragile
X
syndrome. l'6Fragile
X
syndrome is
the mostfrequent
known inherited cause
of
mental retardation,
with
anestimated prevalence
in
predominantly
Caucasianpopulations ranging from 0.4/1000
to 0.8/1OOO
in
males and from0.2/1000 to 0.6/1000
in females.4'7
Affected individuals have
minor
physical
abnor-malities
andmay
fail to thrive in infancy or
childhood
or
havelearning
difficulties in
school.
Thesechildren
have areasonably long
life span, but
require
constantcare
from
either the
family
or an institution.
They
usually
attend special schools
for
the
mentally
hand-icapped.
Fragile
X
syndrome is
characterized
by
acytogenetically
detectablefragile
sitewhich
appears ast
D"port,rrnt
of Hisrology, Faculty
of
Medicine, Dipouegoro lJniversity/ Cytogenetics
IJttit
Telogorejo Hospital, Sennrang, Indonesia.a
-
Departn
of Medicine,Dip
etilarartg, Itrdonesia.'r'C)togen
4 Department of of Wales Hospital, S),dnq,, Australia18
Sultana et al.a break
near
the
end
of
the long arm
of the
X
chromosome. The basic defect
of
fragile
X
is
expan-sion of
the numberof
thetrinucleotide
CGG repeats atthe
5'
endof
theFRAXA
gene.8Chromosomal disorders
in
mentally
retarded
children
havenot
beenstudied
in Indonesia
becauseof
the lack
of
diagnostic
facilities. While
undertaking
a survey
of
chromosomal
abnormalities
in
mentally
retarded
children
in
Semarang,
Indonesia, we
iden-tified a family with two
mentally retarded
malesdemonstrating
the presenceof fragile X
chromosomes.This is
the
first
reported
family
with
fragile
X
in
Indonesia.
MATERIALS
AND
METIIODS
Patients
The
family
wasidentified in
the courseof
a screeningprogram
of MR
maleswho
appearedto
bephenotypi-cally normal.
There weretwo
brothers(Dm
age 13 andPr
age8) in
aspecial school, reported
to
be
intellec-tually
handicapped.
They
have one
sister(Cl
age
14)who is
intellectually normal and
attends
a
normal
school. Both
parents arealive
andwell
(see pedigree).Findings from
a
physical
examination
including
tes-ticular
measurement
(comparative palpation)
usingtesticular models
of known
volume (orchidometer
)
eof
thesetwo
brothers
areshown
in
Table
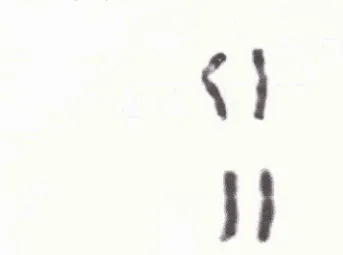
1 .Table l.Clinical description of the two brothers"
Case I
(Dm)
Case 2 (Pr)ItreàJ Inàones
Blood collection
Ten
ml
of
heparinized
peripheral blood were
drawn
from
each
individual
for cytogenetic
and
DNA
analysis.
Blood
was also screenedfor hypothyroidism
by
blotting it
onspecial
filter
paper.Cytogenetic
studies
Chromosome preparations were
madeby
culturing
10drops
of
peripheral blood
at
37oC
for
72 hours in
duplicate
tubes each
containing
5 ml
Iscove's Low
Folate medium
supplemented
with
57oFetal
Bovine
Serum (FBS)
and 0,025
ml
Phytohaemaglutinin-P
(Gibco). To
eachtube,
0.1
ml thymidine (final
con-centration 0.3 pg/ml) and
3
drops colchicine (final
concentration
I
pg/ml)
were
addedrespectively
at 24 hours and 25minutes
beforeharvesting. Chromosome
spreads
were
made according
to routine
procedures.Chromosome
analysisfor fragile X
wasperformed by
scanning 50
unbanded Giemsa-stained
metaphases.When
cells
with
chromosome breakage
in
group
Cwere
found,
a
further
50
cells
and
100 cells
werecounted
in
males andfemales respectively. The
coor-dinates of
positive
cells were noted and the metaphasesphotographed. Subsequently, the slides were destained
in
3:1 methanol:acetic acid,
and G-bandedfor
confir-mation
of
the
fragile
X.
Six further
new
bandedcells
were analyzed
andanother
20 cells
were
counted
toassess
structural and numerical
chromosome
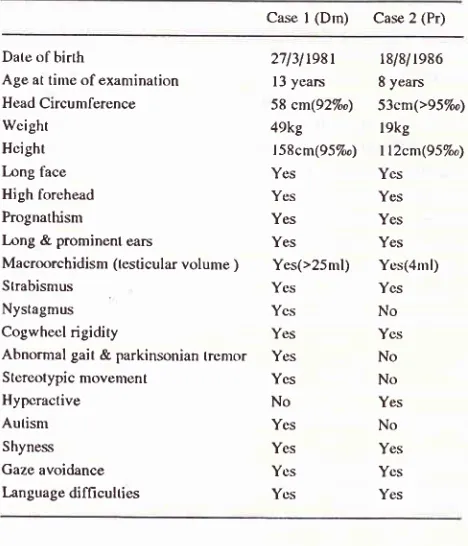
abnor-malities (Figure
1 shows one chromosomewith fragile
X in
Cl),
Molecular
studies
DNA
was extractedfrom peripheral blood
by using the saturatedsalt
method.t' Eight
micrograms
of
DNA
were digested
with
one
unit of
the restriction
en-donuclease
PstI
(Pharmacia)
in
the
buffer
recom-mended
by
themanufacturer
togetherwith
spermidine
in
atotal volume of
20pl
. Agarose gelelectrophoresis
was
performed
(0.757o agarose,xl
Tris-borate
EDTA
buffer, 35 volts
for
16
hours). An SPPI
ladder
(Bresatec)
andnormal control DNA
were included
in
each gel.
After capillary blotting
toHybond
N*1Amer-sham),
prehybridisation
wasperformed for
one hourin
rapid-hyb
buffer
(Amersham
RPN
1636) at 65oC. TheFRAXA
probe pfxa3 and an X-chromosome
single
locus control probe pSS (both
kindly
supplied by
Professor
G.
Sutherland,
Adelaide)
were
preparedby
32P-in"o.po.ation
by
random
hexamer
pi-ing,
unâ
hybridisation performed
in
the
same
buffer
for
16hours at
65"C. Washing
wasperformed
in
2x
SSC and0.1% sodium
dodecylsulphate
(SDS)
three
times
atDate ol birth
Age at lime of examination
Head Circunrlerence Weight
Hcight
bng tàce
High forehead Prognathisnr
L)ng & prominent eârs
Macroorchidism (testicular volume ) Strabismus
Nystagmus Cogwhecl rigidity
Abnormal gait & parkinsonian tremor Stereotypic movenlent
Hypcractive
Aulism Shyness Gaze avoidance
language difficulties
27l3lr98t l3 years
58 cm(92Væ) 49kg
| 58cm(95loo)
Yes Ycs Yes Yes Yes(>25m1) Yes Ycs Yr:s Yes Ycs No Ycs Yes Ycs Ycs
l8i 8i 1986 8 years
[image:2.595.49.283.477.750.2]VoI 4, No
l,
January-March, 1995 Fragile X Mental Retardatiottl9
Figure
I.
Fragilex
chrotnosone (Ieft) and nontnl X chrotnosonre (right) in fettnle(cl)
room
temperaturefor
20minutes
and thentwice
for
30minutes
ar
65oC
in 0,lx
SSC
and 0.1%
SDS.
Autoradiography
wasperformed
for
l-3
days at _7OoCusing intensification
screens.Screening
for
hypothyroidism
Iter paper
(S&S
903for hypothyroidism
the Oliver
Latham
Laboratory,
Sydney.RESULTS
Clinical
finding
A
family
of five (2 parents
and
3
siblings)
wasstudied.Two affected
brothers
were
examined. Both
no obstetric
and
ms
asata
ofhypothyroidi
ts andnormal
on
physic
The
pedigree
is shown
in Figure 2
andclinical
featuresof
the
two
brothers are presentedin Table
I
andFigure
3.Cytogenetic Analysis
Cytogenetic study
of
two affected sons identified
abreak
in
thelong arm
of
theX
chromosome
atq27.3
(FRAXA
locus)in
IOOmetaphases:3To
inDm
and4Toin
Pr. The mother
anddaughter(Cl)
had
3 %
and,6Tofragile
X cells
in
150
metaphasesrespectively.
No
fragile sites
were identified
in
50
metaphasesin
thefather.
Molecular Analysis
The
Restriction fragment length
polymorphism
(RFLP)
using thepfxa3
probe detected a constant bandbetween 1.0 and
l.l
kb
in normal controls.
Simul_taneous
hybridisation with
pSgyielded
a0.g kb
bandwhich provided an intensity control
for
normal
X_chromosome copy number in all individuals.
In proband
sonI
(Dm)
thenormal
pfxa
band was replacedby
1.60 kb andZ.6kbbands, while
hisbrother
son II (Pr)
hada2.2
kb but nonormal
band.Their sister
(Cl)
was
a
carrier,
with
an abnormal 2.2 kb
and anormal 1.1 kb band which was
also present
in
their
father.
Their mother
was also acarrier,
with abnormal
1.3
kb
andnormal
l.l
kb
bands (seeFigure
2).Screenin g
for
hypothyroid
ism
Screening
for
hypothyroidism was negative
for all
five
membersof family.
DISCUSSION
We report the first recorded
casesof
Fragile
X
in
an20
Sultana et al. MedJ Indones-5
4
3
I
2
1
[image:4.595.67.548.60.664.2]j 'yÀ: ,'J
Figure 2. Shows five lines of a Southern blot. The band obtained by hybridising Pstl digested genonic DNA with the
X chronosone
probe pS8 is used as a control (C)for densitonetry, while the nonnal band size (N) obtained using the
FMXA
probe is indicated. Thefather (lane 1) has only a nornal band, while the nother (lane 2) k a cariier, since thereis
an
additional higher band. EachFMXA
band is of reduced densiry relative to lhe control, C. The daughter (lane 3) is also a carrier, while the sonsDil (lane 4) and
Vol 4, No
l,
January-March, 1995Figure
j.
Two affected brothers, Dm (lefi) and Pr (right)donesia
except
for
a caseof fragile
X
mental
retarda-tion in
oneDutch-Indonesian
in
Hawaii,
whoseethnic
background
wasnot
reported. I IThe affected males
(Dm
andPr)
showed
macro-orchidism.
In
the
caseof
the
8year
old
the testicular
volume
should be
lessthan
4 ml. In the
13 yearsold
who is showing early sign
of
puberty
such as
somepubic hair the testicular size should be
4 ml
but
is already over 25ml.
Both
have long ears andprominent
jaws,
shyness,
no
speech
difficulties but both
havelanguage
deficits
such
asabnormally
frequent
useof
short
sentences. These featureswere
presentin
many
patients
of fragile
X syndrome.o'''tt
Th.y
also
hadstrabismus and nystagmus
which
are occasional
fea-Fragile X Mental Retardation
2l
,g
tures
in
these individuats.4'13
The two
affected
boyshave
different
characters: one
is
hyperactive and
theother quiet
andautistic. Both traits
are seenin fragile
X MR
syndrome
The frequency
of fragile
X
cells
is
37o-
4%
in
the
affected
males(two
sons) appearto
belower
thanin
other studies
which reported an incidence of
2-5O7o.r'1
Interestingly,
thefrequency
offragile
cells washigher
in the carrier daughter than in her
affected
brothers.
The fragile X locus
is
a folate
sensitive
fragile
site.
Detection
is dependent on either aculture medium
deficient
in
folate
or
containing
an inhibitor
of
folate metabolism
(eg.FUdR,
methotrexate,
excess22
Sultanaeral.thymidine)
and reduced content
of
FBS.la'15'16It i"
possible that although
low
folate medium was
usedthere
was
enough
folate
and
FBS
in
the medium
to
reduce theincidence of fragile
X
expression .Recently
two other folate sensitive fragile sites (FRAXE
andFRAXF) were found
in
mentally retarded
cases
atxçl-zâ.r7't8'1e,20
Th"""
,r"*
.ui"
fragile sites
canonly
be distinguished
from
the fragile
X
by
DNA
analysis.
DNA
analysis
using the probe pfxa3 and
therestriction
enzyme Pst I
is
diagnostic
of
thefragile
X
genotype. The band sizereflects
the numberof CGG
repeats
with
the
following finding:
in
non-carriers
(male orfemale)
there is a constant bandof
I .0 - 1.I
kb;
in
phenotypically
normal
malecarriers,
there is a bandbetween
1.1
and 1.6 kb
in
size
representing
7O-2OOCGG
copies .t6'2r'22In
affected males
there arelarger
and/or
multiple
bandswith
the sizeof
the band greaterthan
about
1.6
kb
(>2OOcopies)together
with
hyper-methylation
of
CpG dinucleotides.
In
female carriers,
7O-2OO
copies
are
designated
premutation and
>200copies
afull
mutation.Ï6,te,zl
in
o*
casefamily,
weidentified
a
1.1kb
band
in
the
father.
One son
(Dm)
had 1.6 and2.6 kb
bands
suggesting
mosaicism
for
premutation
andfull
mutation,
while
the other son(Pr)
hadonly
a2.2 kb band indicating
that
hehad
afull
mutation. The mother had
1.3
kb
band suggesting
apremutation
and
is
therefore
a carrier. The
daughterwho
had herfather's
l.l
kbnormal
band and anabnor-mal2.2
kb
band,indicating that
herCGG
repeats hadexpanded
to
full
mutation, consistent
with
thefinding
of
othersin
theliterature
that thereis
a Drosressionof
expansion
from
onegeneration to
rhen;xt.Zl9'22
The
implications
of
thesefindings
arethat other
membersof
thefamily,
in
particular
aunts and unclesof
the proposita should be studied
to
determine
theorigin
of
thefragile X.
Genetic counseling
can then bepromoted
for
members
of
the
family who
have
beeninvestigated.
Acknowledgments
We
aregrateful to
the Rector
of
Diponegoro
Univer-sity,
Deanof Medical
Faculty
of
Diponegoro
Univer-sity
and
Director
of
Six
Universities
Development
Rehabilitation Project who
supported
this study.
We
thank the
Director
of
Telogorejo Private Hospital
Semarang and
the Cytogenetics
Unit
staff who
helpedin
thecollection,
preparation
of
samples andprovided
the laboratory
in which
cytogenetic studies were
per-formed.
We
thank
the
members
of
the Fragile X
Department,
Prince
of
Wales Hospital Prof. Gillian
Turner,
Dr,
SamanthaWake
andMs.
Hazel Robinson
for discussions.
Particular thanks
are extendedto
theMed J Indones
head
of
Dharma
Bhakti
foundation
and the teachers atthe Dharma
Bhakti
Special School,
for their
willing-ness to
participate
in
this study.
REFERENCES
1. Connor
JM,
Ferguson-SmithMA.
Essential Medical Genetics. 4th ed. Oxford, Blackwell Scientific Publications, 1993;123:148-9.2. Harper PS. Practical Genetic Counselling. 4th
ed.
Oxford, Butterworth Heinemarm, 1993; 185-91.3. Thapar
A,
GottesmanII,
Owen MJ, O'Donovan MC,Mc-Guffin P. The Genetics
of
Mental Retardation.Brit
J Psy1994; 164:747-58.
4. Hagerman RJ, Silverman
AC
(ed). FragileX
syndrome diagnosis, tleatment, and research. Baltimore: The JohnsHopkins University Press, 1991.
5. Turner G, Turner B. X -linked mental retardation. Am I Med Gen 1974;
l1:
109-13.6. Mikkelsen
M.
Sexlinked mental retardation. In : Vogel F,Sperling
K
(ed). Human Genetics. Berlin,Springer-Verlag, 1987;441-9.7. Davies
KE.
The FragileX
syndrome.Oxford:
Oxford University Press, 1989.8. Verkerk AJMH, Pieretti M, Sutcliffe IS, Fu YH, Kuhl DPA, Pizzuti A, et al. Identification of a gene (FMR-l) containing a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in the fragile
X
syndrome. Celll99l;
65: 905-14.9.
PraderA.
Testicular size: Assesment and clinicalimpor-tance. Triangle 19 66; 7 :24O-3.
10.
Miller
SA, Dykes DD, Polesky HF.A
simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Research 1988; 16:1215.11. Rhoads FA. Fragile
X
syndrome in Hawaii: a summaryof
clinical experience. Am
I
Med Gen 1984;17: 209-14. 12. Ienkins EC, Shapiro LR, Brown WT. Prenatal Diagnosisof
fie
FragileX
syndrome.In:
MilunskyA,
(ed).
Geneticdisorders and the fetus, diagnosis, prevention and treatment.
Baltimore: The Johns Hopkins University
Prcss,l992;241-55.
13. Chudley AE, Hagerman
RI.
FragileX
syndrome, medicalprogress. Ped, 1987;l l0:82 l-3 1.
14.
Sutherland
GR, Hecht
F.
Fragile sites on
humanchromosome, Oxford: Oxford University Press, 1985.
15. Sutherland GR, Baker E, Fratini
A.
Excess thymidine in-duces folate sensitive fragile sites. AmI
Med Gen1985;22:, 433-43.16. Richards
RI,
Sutherland GR. FragileX
syndrome. The molecular picture comesinto
focus. Trendsin
Genetics1992; 8: 249-55.
17. Knight SJL, Flarurery
AV,
Hirst MC, CampbellL,
Chris-todoulou Z, Phelps SR, et al, Trinucleotide repeatamplifica-tion
and hyper methylationof
a
CpG islandin
FRAXE mental retardation.Cell
1993;7 4: 127 -34.Vol 4, No 1, January-March, 1995
19. Hirst MC, Barnicoat A, Flyrur G, Wang Q, Da\er M, Buckle
Vf,
et al: The identification of a third fragile siie , FRAXF,nXq27n28
distal to both FRAXA and FRAXE. HumanMolecular Genetics L993; 2z 197 -2C{J,.
20. Bates G, læhrach H. Trinucleotide repeat and human genetic
disease. BioEssays 1994; 16: 277 -83.
21. Sutherland GR, Gedeon A, Komman L, Donnelly A, Byard
RW, Mulley
IC,
et al.
Prenatal Diagnosisof
fragileX
Fragile X Mental
Retardation
23syndrome by direct detectionof the unstable DNA sequencc.
New England
I
Med.;l99l:
l72O-2222. Yu S, Pritchard M, Kremer E, Lynch M, Nancanow f,Baker
E et al. Fragile
X
genotype characterizedby
an unstableregion
ofDNA.
ScienceL99l;252:
lL79-81.23. Taylor A, Safanda JF, Fall Mf, Quince C, I-ang KA, Hull CE
et all.
Molecular predictorsof
cognitive involvementin
female carriers of fragile X syndrome. Iama SEA; June 1994:
25-31.