PROCEEDING BOOK
RHEUMATOLOGY UPDATE 2020
“Clinical Rheumatology in Daily Practice”
Tiara Convention Centre and Prof. Boloni General Hospital, 17-19 January 2020
Editor:
Dr. dr. Blondina Marpaung,Sp.PD,K- Rdr Andi Raga Ginting, M.Ked (PD),Sp.PD,K- Rdr. Rizqi Arini Siregar, M.Ked (PD),Sp.PD
dr. JunitaTarigan
Reviewer:
Dr.dr. Juliandi Harahap,MA
USU Press
Art Design, Publishing & Printing Gedung F
Jl. Universitas No. 9, Kampus USU Medan, Indonesia
Telp. 061-8213737; Fax 061-8213737 Kunjungi kami di:
http://usupress.usu.ac.id
USUpress 2020
Hak cipta dilindungi oleh undang-undang; dilarang memperbanyak, menyalin, merekam sebagian atau seluruh bagian buku ini dalam bahasa atau bentuk apapun tanpa izin tertulis dari penerbit.
ISBN: 978-602-465-209-8
Perpustakaan Nasional: Katalog Dalam Terbitan (KDT)
Proceeding Rheumatology Update 2020 / Editor: Blondina Marpaung [et.al.] – Medan: USU Press.
2020.
iv, 129 p.; ilus.; 29 cm Bibliografi
ISBN: 978-602-465-209-8
Dicetak di Medan, Indonesia
KATA PENGANTAR
SalamSejawat,
Selamat bertemu kembali di awal tahun ini.Pada saat ini, penyakit autoimun menjadi trending topik di kalangan masyarakat.Sebagai seorang dokter, kita wajib terlibat untuk berkontribusi baik secara edukasi maupun terapi.
Keluhan nyeri sendi dan muskuloskeletal juga banyak dijumpai baik di tempat praktek maupun di rumah sakit.Meskipun telah diperoleh banyak kemajuan dalam pengetahuan tentang patogenesis penyakit reumatik dan nyeri, banyak topik-topik penelitian menunjukkan bahwa sebahagian besar penderita tidak mendapatkan pengobatan yang optimal untuk mengatasi keluhan mereka.
Dengan berkembangnya ilmu pengetahuan dan teknologi di bidang kedokteran terutama Reumatologi, pada kesempatan yang baik ini Divisi Reumatologi Departemen Ilmu Penyakit Dalam FK USU/ RSUP.
H. Adam Malik berencana mengawali tahun 2020 dengan mengajak para sejawat bersama-sama untuk berdiskusi secara scientifik pada acara “Rheumatology Update 2020” tentang materi yang hangat di masyarakat dengan mengundang para pakar lain yang berhubungan dengan penyakit reumatik.
Acara ini merupakan kegiatan yang berisi symposium dan workshop injeksi Intra Artikular dan Muskuloskletal dengan para pembicara Nasional serta pemeran farmasi yang nantinya diharapkan akan memberikan kontribusi yang meningkatkan layanan kesehatan masyarakat.
Medan, Januari 2020 Ketua Panitia
Dr. dr. Blondina Marpaung Sp.PD, K-R
DAFTAR ISI
KATAPENGANTAR ... iii
DAFTARISI ... iv
Myths & Facts inRheumatic Diseases ... 1
To introduce the Interesting Diseases inRheumatology Field ... 3
Perdarahan Gastrointestinal padaPasien Rematik... 11
Current Pain Management ofRheumatic Disease ... 14
The Pathogenesis and Management of Neuropathic Pain: Focus PainfulDiabeticNeuropathy ... 21
Current Management of Rheumatic Arthritis: FocusConventional DMARD ... 35
Peran Anti Tumor Necrosis Factor (TNF) Alfa pada PenatalaksanaanArtritisReumatoid ... 41
Febuxostat: The New Treatmentof Hyperuricemia ... 45
Peranan Kolkisin dalam TatalaksanaKristalArtropati ... 49
Fibromyalgia: Is it aRheumatic Disease? ... 53
Pendekatan Psikosomatic pada PenyakitRheumatoidKronis ... 59
Musculoskeletal Complications inDiabetic Patient ... 64
Manifestasi Kelainan Muskuloskeletal pada PenyakitGinjalKronis ... 71
Fever in Autoimmune Disease: is it FlareorInfections? ... 75
Clinical and Manifestation ofLupus Nephritis ... 78
Efikasi OAINS dalam Penatalaksanaan Osteoarthritis: Fokus padaData Meta-Analisis ... 86
DiagnosisSpondiloartritis ... 90
PenatalaksanaanAnkylosingSpondylitis ... 94
Clinical and Diagnostic Approach ofPsoriatic Arthritis ... 100
Long Term Efficacy in Adalimumab for RhematoidArthritisTherapy ... 108
Mekanisme Aksi Vitamin D & EfekterhadapTulang ... 111
Clinical Approach and Update Management ofVasculitis Syndrome ... 116
Clinical Approach and Management ofSystematic Sclerosis ... 125
Immunopathogenesis of Autoimmune Rheumatic Disease ... 132
CLINICAL AND MANIFESTATION OF LUPUS NEPHRITIS
Blondina Marpaung
Division of Rheumatology, Department of Internal Medicine Faculty of Medicine
Universitas Sumatera Utara
1. Introduction
Systemiclupuserythematosus(SLE)isachronicautoimmunediseaseofunknowncausethatcan affectvirtuallyanyorganofthebody.Immunologicabnormalities,especiallytheproductionofanumber ofantinuclearantibodies(ANA),areaprominentfeatureofthedisease.SLEpatientspresentwithvariable
clinical features ranging from mild joint and skin involvement to life-threatening renal, hematologic, or central nervous system involvement. The clinical heterogeneity of SLE and the lack of pathognomonic features or tests pose a diagnostic challenge for theclinician.1
One of the most common and severe manifestation in SLE is Lupus nephritis. LN is a glomerulonephritis characterized by the accumulation of immune complexes in glomeruli and often an inflammatory response in all kidney compartments. Over time inflammation leads to chronic damage of the renal parenchyma and loss of kidney function. 2
In the US, approximately 35% of adults with systemic lupus erythematosus (SLE) have clinical evidence of nephritis at the time of diagnosis, with an estimated total of 50–60% developing nephritis during the first 10 years of disease. The prevalence of nephritis is significantly higher in African AmericansandHispanicsthaninwhites,andishigherinmenthaninwomen.Renaldamageismorelikely to develop in nonwhite groups. Overall survival in patients with SLE is approximately 95% at 5 years after diagnosis and 92% at 10 years after diagnosis (5,6). The presence of lupus nephritis (LN) significantly reduces survival to approximately 88% at 10 years, with even lower survival in African Americans.3
SLE complicated by LN has a worse outcome than SLE without kidney involvement. Although there are treatment options for LN, its prognosis has remained unchanged in recent years. Early recognition and prompt treatment of LN are critical to improving outcomes.
2. Definition For LupusNephritis
2
LN is defined as clinical and laboratory manifestations that meet ACR criteria (persistent proteinuria>0.5mgperdayorgreaterthan3+bydipstick,and/orcellularcastsincludingredbloodcells [RBCs], hemoglobin, granular, tubular, or mixed. A review of the ACR criteria has recommended that a spot urine protein/creatinine ratio of 0.5 can be substituted for the 24-hour protein measurement, and “active urinary sediment” (>5 RBCs/high-power field, > 5 white blood cells [WBCs]/hpf in the absence of infection, or cellular casts limited to RBC or WBC casts) can be substituted for cellular casts. An additional, perhaps optimal, criterion is a renal biopsy sample demonstrating immune complex–mediated glomerulonephritis compatible withLN.
3. Clinical Manifestation of LupusNephritis
3
The clinical manifestations of LN are often subtle and most commonly will be discovered by examination of the urine as opposed to physical examination (Table 1) All patients with SLE should be evaluated for kidney involvement at initial diagnosis and at least yearly there- after even if they do not have symptoms of kidney disease. It is also recommended that patients be re-evaluated for LN if SLE flares.Evaluationisstraightforwardandshouldincludeaurinalysisandmeasurementofkidneyfunction,
generally a serum creatinine concentration oreGFR.2
Table 1.Prevalence of clinical manifestation in patients with lupus nephritis.
Clinical Manifestation Approximate Prevalence, %
Proteinuria 100
Nephrotic range proteinuria/nephrotic syndrome 50
Microscopic hematuria 80
Macroscopic hematuria <5
Urinary red blood cell casts 30
Other urinary cellular casts 30
Renal insufficiency 60
Rapid decline in kidney function 15
Hypertension 30
Tubular abnormalities 70
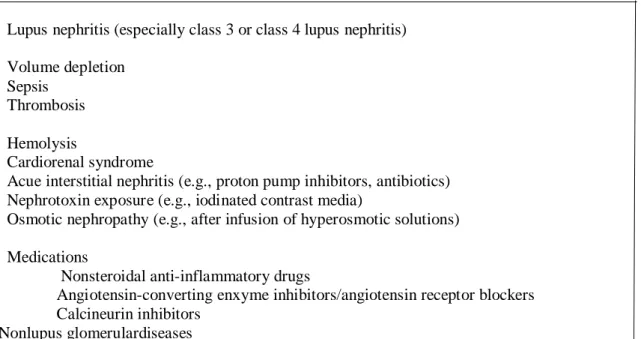
The clinical diagnosis of LN requires only the presence of abnormal proteinuria in a patient with SLE. The diagnosis of LN is supported if the proteinuria is accompanied by hematuria, especially if the urine red blood cells are suggestive of glomerular bleeding (Fig.1). Impaired kidney function may also support the diagnosis of LN, but because patients with lupus are at risk for acute kidney injury, other causes should be excluded (Table 2) before attributing renal insufficiency to LN.
Figure 1.Urine sediment ndings in lupus nephritis. Acanthocytes are dysmorphic red blood cells that indicate glomerular bleeding. Several examples are shown in (A) and (B) (arrows). A white blood cell cast is shown in (C), and a red blood cell cast is shown in (D).
Table 2. Causes of Acute Kidney Injury in SLE patients
Proteinuria is not, however, specific for LN and can be seen in SLE patients without the immune complex glomerulonephritis characteristic of LN. The diagnosis of LN should be verified by kidney biopsy (which is discussed later). Furthermore, the absence of proteinuria does not exclude LN. In subclinical or silent LN glomerular immune complexes are found despite an absence of proteinuria, hematuria, and impaired kidney function. Because this diagnosis requires a kidney biopsy in patients without typical clinical indications for a biopsy, the true prevalence of silent LN is difficult to determine.
However,protocolbiopsystudiesinSLEpatients suggestsilentLNmaybecommon.Thenaturalhistory ofuntreatedsilentLNisalsonotknown.AlthoughmostofthesepatientshaveamildmesangialLN(class
1orclass2),15%to24%haveproliferativeLN(class3orclass4).SilentLNmaythereforerepresentthe earliest stage of what will become clinically relevantLN.2
LN can generally be divided into nephritic or nephrotic presentation, although there can be overlap. Nephritic patients variably display hypertension, hematuria, impaired kidney function, and peripheral edema; whereas nephrotic syndrome is characterized by heavy proteinuria (≥3.5 g/24 hours), low serum albumin (<3 g/dL), peripheral edema, and hypercholesterolemia.
4. Laboratory Assesment of Lupus Nephritis Proteinuria
2
The 24-hour urine collection is the gold standard for quantifying proteinuria in glomerular diseases. Although 24-hour urine specimens may not always be accurately collected, the urine protein/creatinine ratio (UPCR) of an intended 24-hour collection that is at least 50% complete is an accurate reflection of daily proteinuria. The first morning void UPCR also provides an accurate estimate of 24-hour proteinuria. In contrast, although convenient to collect, the random spot UPCR does not correlate well enough with 24-hour proteinuria to be used to inform important management changes for individual LN patients.Although patients can be monitored with random spot UPCR, if there are changes in the spot UPCR and/or the patient’s condition, a 24-hour urine collection should be obtained for confirmation and decision-making.
Urine Sediment
2
Examination of the urine sediment (the cellular pellet remaining after centrifugation) of a fresh urinespecimenishelpfulinmonitoringLNdiseaseactivity.Theurinesedimentisexaminedforevidence of glomerular bleeding and renal infammation. Glomerular bleeding is indicated by red blood cell casts or, more commonly, dysmorphic red blood cells called acanthocytes (see Fig.1). Renal inflammation is suggested by the presence of white blood cell casts or, more commonly white blood cells in the absence ofbacteriuriaorurinarytractinfection.Theidentificationofcellularcastsdependsonthequalityand
Lupus nephritis (especially class 3 or class 4 lupus nephritis) Volume depletion
Sepsis Thrombosis Hemolysis
Cardiorenal syndrome
Acue interstitial nephritis (e.g., proton pump inhibitors, antibiotics) Nephrotoxin exposure (e.g., iodinated contrast media)
Osmotic nephropathy (e.g., after infusion of hyperosmotic solutions) Medications
Nonsteroidal anti-inflammatory drugs
Angiotensin-converting enxyme inhibitors/angiotensin receptor blockers Calcineurin inhibitors
Nonlupus glomerulardiseases
freshness of the urine sample, how the sediment is prepared, and the skill of the reader. For these reasons the presence of casts in LN urine samples is often missed.2
Changes in the urine sediment over time may herald a disease are, whereas resolution of glomerular bleeding and renal inflammation suggests that LN is responding to treatment. Urine sediment examinationisdifficulttostandardizeacrosspracticesites,whichmayexplainitsperceivedlackofutility in multicenter clinical trials. Nonetheless, for the management of individual patients in practice the urine sediment examination isvaluable.
Assessment of Kidney Function
2
Glomerular Filtration rate (GFR) is accepted as the best overall index of kidney function. It providesaroughmeasureofthenumberoffunctioningnephrons.NormalGFRis120to130mL/min/1.73 m2 body surface area, and it dynamically varies according to age, sex, body habitus, and diet.There is no linear correlation between loss of nephrons and loss of GFR because the kidney compensates for the loss of some renal mass. As such, serum creatinine remains normal until approximately 50% of nephrons are lost or when the GFR approaches 60 mL/ min/1.73 m2. True GFR is cumbersome and costly to measure, and in clinical practice it has been replaced by equations that estimate GFR (eGFR) from the serum creatinineconcentration.2
The eGFR equations have some weaknesses. None has been validated against true GFR measurements in a typical SLE population. Because all of these equations are based on the serum creatinineconcentration,theyhavealowsensitivityforearlydetectionofrenaldisease.Additionally,the
serumcreatinineconcentrationmaybeincreasedordecreasedbyconditionsthatareindependentofGFR but that are commonly seen in patients with LN. For example, tubular secretion of creatinine may be decreased by certain drugs like trimethoprim, or increased in hypoalbuminemic patients, and this will increase or decrease serum creatinine concentration, respectively. High-dose corticosteroids can affect skeletal muscle metabolism, alter creatinine production, and increase serum creatinineconcentration.
Serum creatinine may increase if the diet is high in cooked meats and decrease if the diet is vegetarian. Finally, all of the GFR estimating equations assume patients of the same age, sex, race, and serum creatinine concentration have the same rate of creatinine production.
Biomarker of Lupus Nephritis
2
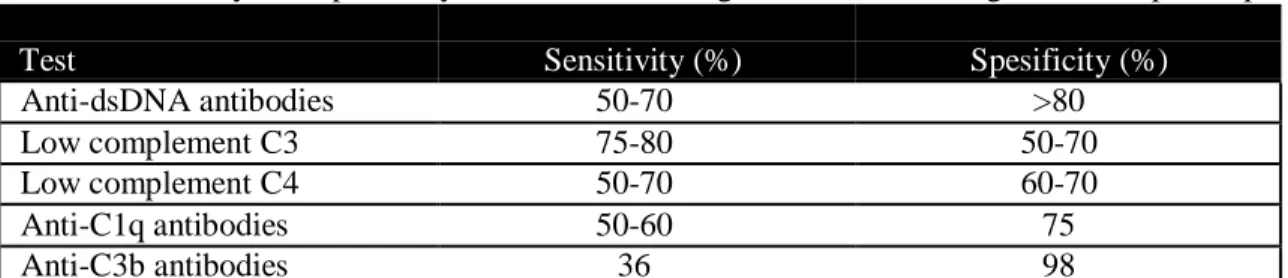
Serum complement levels and anti–double-stranded DNA (anti-dsDNA) antibodies are the traditional serologic biomarkers that have been used clinically to monitor LN activity. Overall, however, theirsensitivityandspeficityarepoortomodest(Table3).Thismaybecausedbythedependenceofanti- dsDNA results on the measurement technique used and the fact that complement component C4 serum levels are strongly in uenced by gene copy number, which varieswidely.2
Autoantibodies to complement proteins C1q and C3b have also been suggested as biomarkers of LN activity. Although these have limited sensitivity, the presence of anti-C3b antibodies is very specific for active LN (see Table 3). The combination of anti-C1q and anti-C3b improves the diagnostic powerof complement autoantibodies.2
Table 3.Sensitivity and Specificity of Common Serologic Tests for the Diagnosis of Lupus Nephritis.
Test Sensitivity (%) Spesificity (%)
Anti-dsDNA antibodies 50-70 >80
Low complement C3 75-80 50-70
Low complement C4 50-70 60-70
Anti-C1q antibodies 50-60 75
Anti-C3b antibodies 36 98
dsDNA, Double-stranded DNA
Although there has been a dedicated effort to develop novel biomarkers of LN activity, renal histology,prognosis,andresponsetotherapy,nonehasbeenapprovedforclinicalusethusfar.Oneofthe major barriers to biomarker qualification has been the lack of validation in independent, prospectively followed patient cohorts.2
5. RenalBiopsy
Unlessthereisacontraindication,arenalbiopsyshouldbeperformedinalmostalllupuspatients who have clinical or laboratory evidence of renal involvement (eg, abnormal proteinuria, active urine sediment, elevated serum creatinine and/or decreased glomerular filtration rate) to establish the correct diagnosis and determine the histologic subtype of LN. Patients already on therapy for LN do not require arepeatrenalbiopsyunlessthebiopsyfindingscouldaltermanagement(eg,asinsomeonewithworsening
clinical parameters despite appropriatetreatment).2
A renal biopsy generally perform in patients who have one or both of the following clinical manifestations: Protein excretion greater than 500 mg/day, an active urinary sediment with persistent hematuria (five or more red blood cells per high-power field, most of which are dysmorphic) and/or cellularcasts.Theurinemaybecontaminatedwithvaginalbloodinmenstruatingwomen.Redcellsfrom this source are not dysmorphic, a rising serum creatinine that is not clearly attributable to another mechanism.2
Renal biopsy should be performed promptly (ie, within days to weeks) in patients who have an appropriate indication. Prompt diagnosis after the onset of LN and subsequent initiation of appropriate therapy are associated with improved outcomes, regardless of the histologic class. A rapidly risingserum creatinine and/or the development of new nephrotic range proteinuria are indications for urgent renal biopsy so that an accurate diagnosis can be established and appropriate treatment can be initiated as soon as possible.2
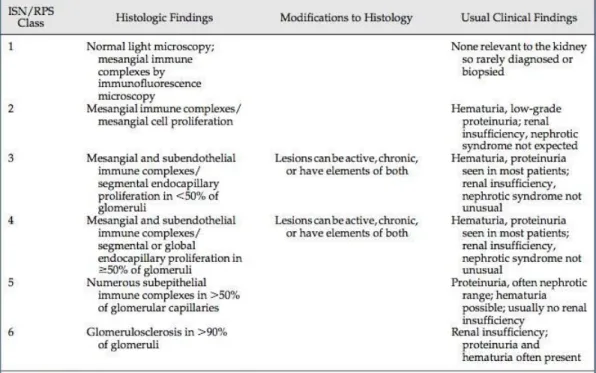
Immune-complex LN is described pathologically using the 2003 International Society of Nephrology/RenalPathologySociety(ISN/RPS)nomenclature.TheISN/RPSsystemclassifiesLNonthe basis of where immune complexes accumulate in glomeruli, the presence or absence of mesangial or endocapillaryproliferation,theoverallextentofglomerularinvolvement(focalordiffuse)andglomerular injury(globalorsegmental),andwhetherglomerularinjuryisactive(inflammatory)orchronic(sclerotic) (Table 4).2
Table 4. The histologic classification of lupus nephritis
The current pathologic classification of LN, known as the International Society of Nephrology/Renal Pathology Society (ISN/RPS) classification, is based on the light microscopic appearanceoftheglomeruliandthelocationofimmune-complexdepositswithintheglomeruli.Inclasses
1and2LNimmunecomplexesarefoundintheglomerularmesangium.Inclass1LNtheglomeruliappear normal, whereas in class 2 LN the glomeruli show mesangial cell proliferation (Fig.2).2
Classes 3 and 4 LN, also called focal and diffuse proliferative LN, respectively, have mesangial andsubendothelialimmunecomplexes(seeFig.2).Thisisaccompaniedbyendocapillaryhypercellularity and in some cases extracapillary hypercellularity. In endocapillary hypercellularity the glomerular capillary lumens are narrowed by leukocyte in ltration. Extracapillary hypercellularity refers to crescent formation. These proliferative lesions involve fewer than 50% of the glomeruli in class 3 and over 50%
in class 4. Proliferative LN is further classified as active, chronic, or active plus chronic. Inflammatory lesions such as endocapillary hypercellularity, glomerular capillary necrosis, and cellular crescents characterizeactivedisease.Inchronicdiseasethehealedremnantsoftheseinflammatorylesions,usually in the form of scarring, are found. LN patients with relapses (flares) of LN often demonstrate active and chronic lesions at the sametime.2
The immune deposits in Class 5 LN, also called membranous LN, are found in the mesangium and subepithelial space, below the glomerular podocytes and their foot processes. In contrast to classes 3 and 4, there is no glomerular hypercellularity or in ammation in pure class 5 LN; instead, the glomerular basement membrane thickens in response to the subepithelial immune deposits (see Fig. 2). Proliferative LN and membranous LN can occur simultaneously.2
Finally, class 6 LN is diagnosed when the kidney biopsy shows 90% glomerular sclerosis in the absence of active, inflammatory lesions.
IndividualLNclasseshavecharacteristicclinicopathologiccorrelations.Class1hasnoclinically relevant renal or urinary abnormalities. hat would prompt a kidney biopsy, and so is seldom diagnosed.
Class 2 LN normally presents with preserved kidney function, mild, non- nephrotic proteinuria (<3.5 g/day),andglomerularhematuria.Prolifera-tiveLN(class3orclass4)generallypresentswithsignicant,
oftennephroticrangeproteinuria,glomerularhematuria,leukocyturia,cellularurinarycasts,andimpaired kidney function. Patients with proliferative LN are at risk for rapid deterioration of renal function. Class 5 LN is characterized by heavy proteinuria, usually nephrotic range, and normal kidney function often without hematuria. Progressive loss of renal function is seen in Class 6 LN. Such patients often have proteinuria, but this is caused by chronic damage as opposed to acute in ammatoryinjury.
2
2,5
Figure2.InternationalSocietyofNephrology/RenalPathologySociety(ISN/RPS)classificationoflupus nephritis (LN) illustrated with examples of patients’ biopsies. The class 1 light microscopy with hematoxylinandeosinstainingisessentiallynormal.Electronmicroscopyshowselectron-denseimmune- complex deposits in the glomerular mesangium, which is verified by positive immuno fuorescence for IgGinthemesangialregion.Class2showsmildmesangialcellproliferationonlightmicroscopyandthe
samefindingsasclass1onelectronandimmunofuorescencemicroscopy.Intheexampleofproliferative class 3 LN light microscopy shows segmental endocapillary proliferation, electron microscopy shows subendothelial electron-dense immune deposits, and immuno fuorescence microscopy shows IgG along the glomerular capillary walls. In the class 4 example, light microscopy shows diffuse endocapillary proliferation and a large area of glomerular capillary necrosis. Electron microscopy shows extensive subendothelialimmune-complexdepositsaswellassmallersubepithelialdeposits,suggestingthispatient has combined class 4 + 5 LN. Immuno fluorescence staining was done for complement component C1q, demonstratingitspresenceintheglomerularcapillaries.Theclass5biopsywasstainedwithsilverinstead
ofhematoxylinandeosintobetterillustratetheglomerularbasementmembranematerial(black).Immune complexesinclass5localizetothesubepithelialsideoftheglomerularbasementmembrane(seenreadily
onelectronmicroscopy)andappeartobe“holes”betweenblackareasofglomerularbasementmembrane on
(Photomicrographs courtesy of Dr. Gyongyi Nadasdy, The Ohio State University Wexner Medical Center, Division of Nephropathology.)
REFERENCES
1. Wallace DJ, Gladman DD, Pisetsky DS, Curtis MR. Clinical manifestation and diagnosis of systemic lupus erythematosus in adults. UpToDate.2019.
2. Mejia-Vilet JM, Rovin BH. Epidemiology and management of Lupus Nephritis. 2019.727-35 3. Hahn BH, McMaho MA, Wilkinson A et al. American College of Rheumatology Guidelines for
Screening, Treatment and Management of Lupus Nephritis. Arthritis Care & Research. 2012.
797-808.
4. Almaani S, Meara A, and Rovin BH. Update on Lupus Nephritis. Clin J Am Soc Nephrol. 2016.
1-11
5. Falk RJ, Dall’Era M, Appel GB. Indications for renal biopsy in patients with lupusnephritis.
UpToDate. 2018. 1-10