178
Diference of the orphans in Ar-Rohman Foster Home Bandung oral health (Nurayni Tri Hapsari et al.)
Corresponding author: Nurayni Tri H, Department of Community Dentistry Faculty of Dentistry Univ. Padjadjaran, Indonesia Jl. Sekeloa Selatan No. 1 Bandung, West Java-Indonesia, Email:[email protected]
P-ISSN 1979-0201, e-ISSN 2549-6212 Available from:http://jurnal.unpad.ac.id/pjd/index DOI:http://dx.doi.
Submission: Aug 2017 Publishing: Nov 2017
Diference of the orphans in Ar-Rohman Foster Home Bandung
oral health status before and after three times of oral health
education
Nurayni Tri Hapsari*, Anne Agustina Suwargiani*, Cucu Zubaedah
*Department of Community Dentistry Faculty of Dentistry Universitas Padjadjaran, Indonesia
ABSTRACT
Introduction: Oral hygiene status is a condition of a person’s oral cavity. Oral hygiene status can be
assessed using the Oral Hygiene Index Simpliied (OHI-S) by Greene & Vermillion. The education given
regarding oral health is one of health promotion with the purpose to increase the ability of children in
terms of maintaining and improving their oral hygiene. The purpose of this study was to determine the diference of the orphans in Ar-Rohman Foster Home Bandung oral health status before and after three
times of oral health education. Methods: The type of this research was a pre-experimental study with
one group of pretest-posttest design with total sampling technique. Subjects of this research were or-phans aged 13-15 years old. The respondents got the clinical examination of OHI-S before and after the oral health education was given for three times. The data obtained then tested using normality test, if the data were normally distributed, then analysed with a paired t-test, and if the data was not nor-mally distributed, then will be analysed with a Wilcoxon test. Results: The results showed a signiicant decrease of plaque index after oral health education was given to the orphans. The examination of the calculus index (CI-S) did not show any change before and after oral health education. OHI-S of children, however, showed a signiicant decrease. Conclusion: There was a signiicant increase in the orphans in Ar-Rohman Foster Home Bandung oral health status after given three times of oral health education.
Keywords: Oral hygiene, oral health education, orphans
INTRODUCTION
Oral health is one of the most vital components
of human bodies. The poor degree of oral health can disturb the quality of a human’s life.1,2
Based on Indonesia Household Health Survey in
2001, the oral problem was reported to be sixth
of the most common disease that the society
experienced. According to Riskesdas in 2013, this problem increased from 23,2% to 25,9%.3
According to WHO in 2003, dental treatment is the
179
Padjadjaran Journal of Dentistry 2017;29(3):178-181.
dental problems are avertible and their initial
occurrences are reversible. Thus, it is preferable
to maintain good oral health to avoid having an expensive dental treatment.
Based on many research, the pattern of foster home living is diferent from family living as it provides physical security, food, and shelter but
is devoid of psychological security. Often these foster homes can only barely meet the needs of their inmates because of poor funding and the
low caretaker to child ratio. These children form a population at risk with reference to abnormal
psychosocial development.5 Research showed that the oral health status of the foster home children
hasn’t been able to be classiied as good.2 The
knowledge of the children and the caretaker at this
foster home on how to maintain oral health is still
lacking. Furthermore, dental health education is still rather neglected. Generally, orphans acquire
dental health education needs to be delivered
to the children and the caretakers in order to
achieve a better dental and oral health status.6
The purpose of this study was to determine the diference of the orphans in Ar-Rohman Foster Home Bandung oral health status before and after
three times of oral health education.
METHODS
This pre-experimental study used the one group pretest-posttest design with a total sample of 31 respondents at the age of 13-15 years old. Clinical examination was conducted using the Oral Hygiene Index-Simpliied (OHI-S) by Greene and Vermilion. The index was examined at the
beginning of the study before a dental health
education and a demonstration on the right way
to use a toothbrush and dental loss was done. The
education was done in several times at the 7th, 14th,
and 21st day by presenting the same topics. At the
28th day, another OHI-S examination prevailed as
a inal inspection. The data was analyzed by using
normally test if the data is normally distributed
the used a T-paired test and if the data is not normally distributed, the Wilcoxon test is used.
RESULTS
Based on Table 1 below showed that before dental
health education, most of the orphans have a moderate category of plaque index, which is 26 children (83,9%). Most of orphans calculus index at the moderate category, which is 16 children (51,6%), and most of orphans OHI-S is in the moderate category, which is 22 children (71%).
At the last clinical examination show, the
most of orphans calculus index change into good
category, which is 25 children (80,6%). After dental health education, most of orphans OHI-S score is in a good category, which is 23 children (74,2%) as
presented in Table 1 below.
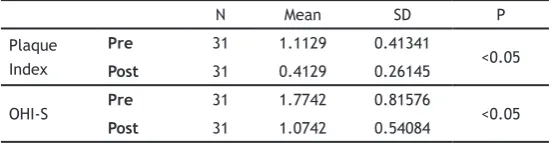
The inal result of the 28th day, after three
times dental health education and demonstration, showed signiicant decreasing OHI-S score from 1,7742 to 1,0742, and also decrease on the plaque index score from 1,1129 to 0,4129. However,
the calculus index was found to be persistent
with a score of 0,6606. The Wilcoxon analysis showed a statistically signiicant decrease in the plaque index (p<0,05). OHI-S score that showed statistically signiicant decrease using T-paired test (p<0,05) as presented in Table 2.
Table 1. Distribution of plaque, calculus, and OHI-S index of orphans in Ar Rohman Foster Care Bandung
180
Diference of the orphans in Ar-Rohman Foster Home Bandung oral health (Nurayni Tri Hapsari et al.)
DISCUSSION
Three times dental health education which was given to the orphans, was determined signiicant decreasing of OHI-S score include plaque score. The decreasing score exists because there is a
change of oral behaviour after dental health
education was given. Through this education,
dental health information could be given to the orphans. Several of dental health education for
12-13 years old children could increase knowledge of oral health also control plaque.7
The other research that conducted by Maheswari et al (2014) in 8-10 years old children
which compared education efectiveness about oral hygiene between conventional technique and the combination of conventional technique and game, could be seen that plaque index decreased signiicantly on both techniques. This education research that conducted by Maheswari
is given every day for seven days.8 The repetition
aimed to emphasize the message on the dental
and oral health issue.9 Edgar Dale concluded that
participants will remember what they see and
listen as much as 50% more than by just listening.10
In the dental health education that we
conducted, we instructed the children to do a mechanical plaque control in order to maintain a good oral health. Mechanical and chemical plaque control can decrease the plaque index score.11
Furthermore, oral hygiene instruction aims to prevent plaque and calculus formation.12
In this study, the calculus index score was never altered. This happened because, during the study, all respondents did not undergo calculus removal. Calculus could only be removed by techniques such as scaling and root planning, using certain instruments such as scalers, curette,
and ultrasonic instruments.12 A study that was
conducted to observe the efect of dental health education on calculus and plaque index score in 200 children with the age of 12-15 shows the
Table 2. The average and p-value of plaque index and OHI-S
N Mean SD P
OHI-S Pre 31 1.7742 0.81576 <0.05
Post 31 1.0742 0.54084
alteration of calculus index score is only slightly;
from 0,40 to 0,38, with signiicant score of 0,481.13
Furthermore, research that conducted to discover education efectiveness about oral and dental
health and also given mouthwash which used twice a day showed that there was no calculus index
diference. This research conducted by 54 navy personnel who were sailing for 201 days. There was no diference occurred in this research, which
can be concluded that with counselling and the use of mouthwash can prevent calculus forming.
This is in contrast to the alteration of plaque index and OHI-S score that is more signiicant.14
CONCLUSION
There was a signiicant increase in the orphans in Ar-Rohman Foster Home Bandung oral health
sta-tus after given three times of oral health educa -tion.
REFERENCES
1. Kwan SYL, Petersen PE, Pine CM, Borutta A.
Health-promoting schools : an opportunity for oral health promotion. Bull WHO. Sep 2005;83:677–685.
2. Markeviciute G, Narbutaite J. Efectiveness of a motivation and practical skills development
methods on the oral hygiene of orphans
children in Kaunas, Lithuania. J Oral Maxillofac Res. Jun 30, 2015;6(3):e2. DOI: 10.5037/ jomr.2015.6302.
3. National Institute of Health Research and
Development (NIHRD). Indonesia basic health research (RISKESDAS) 2013. Jakarta: Ministry of Health Republic of Indonesia; 2013.
4. WHO. Continuous improvement of oral health
in the 21st century – the approach of the
WHO Global Oral Health Programme. The World Oral Health Report 2003. Geneva: Oral
181
Padjadjaran Journal of Dentistry 2017;29(3):178-181.
Prevention and Health Promotion; 2003. 5. Sharma A, Gaur A, Pareek S, Raja V, Sanadhya S,
Sharma AB. Oral Health Status and Treatment Needs among Orphanage Children of Jaipur City. Sch J App Med Sci. 2014;2(5D):1776-80.
6. Ojahanon PI, Akionbare O, Umoh AO. The oral hygiene status of institution dwelling
orphans in Benin City. Niger J Clin Prac. Jan-Mar 2013;16(1):41–4. DOI: 10.4103/1119-3077.106732.
7. Shenoy RP, Sequeira PS. Efectiveness of a school dental education program in improving
oral health knowledge and oral hygiene practices and status of 12-to 13-year-old schoold children. Indian J Dent Res. Apr-Jun 2010;21(2):253-9. DOI: 10.4103/0970-9290.66652.
8. Maheswari UN, Asokan S, Asokan S, Kumaran ST. Efects of conventional vs game-based
oral health education on children’s oral
health-related knowledge and oral hygiene status-a prospective study. Oral Health Prev Dent. 2014;12(4):331-6. DOI: 10.3290/j.ohpd. a32677.
9. Haleem A, Khan MK, Suia S, Chaudhry S, Siddiqui MI, Khan AA. The role of repetition
and reinforcement in school-based oral health education-a cluster randomized controlled trial. BMC Public Health. Jan 4, 2016;16(2):1-11. DOI: 10.1186/s12889-015-2676-3.
10. Dale E. Audiovisual Methods in Teaching. New York: Dryden Press; 1969.
11. Reddy S. Essentials of Clinical Periodontology and Periodontics. 4th ed. New Delhi: Jaypee
Brothers Medical Publishers Pvt. Ltd.; 2011. 12. Newman MG, Takei H, Klokkevold PR, Carranza
FA. Carranza’s Clinical Periodontology. 12th ed.
Philadelphia: W.B Saunders; 2015.
13. Sanadhya YK, Thakkar JP, Divakar DD, Pareek
S, Rathore K, Yousuf A, et al. Efectiveness of oral health education on knowledge, attitude, practices and oral hygiene status among 12 - 15-year-old schoolchildren of ishermen of Kutch district, Gujarat, India. Int Marit Health. 2014;65(3):99-105. DOI: 10.5603/ IMH.2014.0022.
14. Wang G, Li W, Liu Y, Chen X, Huang J, Zhao
Y, et al. Eicacy of dental health education
and a novel mouthwash on periodontal health