Presented on Neuropathic Pain Congress - NeuPSIG 2015 | Nice, May 2015 1
NEUROPATHIC PAIN CORRELATED WITH QUALITY OF LIFE
IMPAIRMENT IN MORBUS HANSEN PATIENTS
Ernesta P Ginting, Thomas Eko Purwata, Purna Putra, Arimbawa, Eka Widyadharma Neurology Department Udayana University/Sanglah General Hospital Denpasar, Bali, Indonesia
ABSTRACT
Morbus Hansen (MH) is still one of the dreaded disease due to the complications and quality of life (QoL) impairment that it inflicts. Many factors can lead to the QoL impairment in patients with MH, including the presence of lesions on the skin that interferes with the appearance, bad stigma about the disease in community, a long therapy duration, recurrence of leprosy reactions, the incidence of disability, and the presence of complications of chronic neuropathic pain (NP). This research aims to find out the proportion and characteristics of NP in MH patients, as well as to find out the correlation between the NP with the QoL impairment in MH patients.
This research was a cross sectional study. Sampling method was using a non random consecutive sampling. Data were analyzed with SPSS 20.0 for window. A descriptive analysis was conducted to determine the proportion of NP incidence and characteristics in MH patients, lambda test to determine the correlation between the NP with the QoL impairment.
A total sample of 49 people has been obtained since January 6th, 2014 until March 29th,
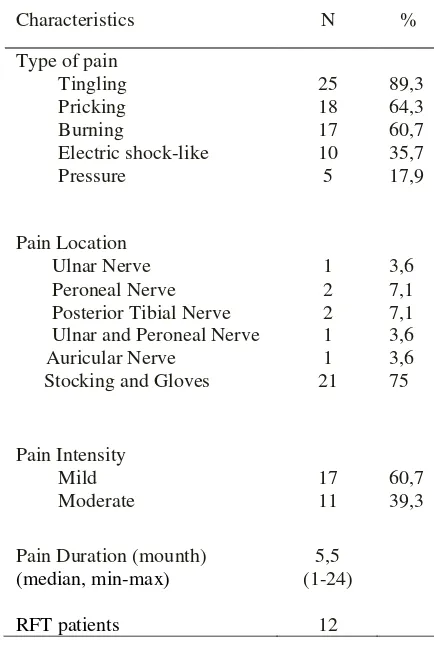
2014. The proportion of NP in MH patients was 57,1%. The most frequent type of NP was the sense of tingling (89,3%), with mild intensity (60.7%), the most frequent location was at the hands and feet (gloves and stockings) (75%), with the average of pain duration was 5.5 months. The proportion of QoL impairment was 44,9%; with the impairment of Physical Component Scale (PCS) was 95.5% and the impairment of Mental Component Scale (MCS) was only 27.3%. This study showed a significantly strong positive correlation between NP and QoL impairment (p=0,004; r=0,636).
It can be concluded that the presence of NP was more likely in disrupting the QoL in MH patients.
Keywords : Morbus Hansen, Neuropathic Pain, Quality of Life.
INTRODUCTION
Morbus Hansen (MH) or leprosy, is a chronic infectious disease caused by Mycobacterium leprae, a microorganism that has predilection areas, especially in the skin and peripheral nerves. It is one of the most common cause of non-traumatic peripheral neuropathy.(1)
MH is still a problem faced by most people of the world, especially in developing countries. According to the WHO Weekly Epidemiological Record, based on the reports from 130 countries, there are 228,474 new cases of MH during
2010. Indonesia ranks as the third largest number of MH cases in the world, after India and Brazil. During 2010, there was 17,012 new cases of MH in Indonesia, with 1,822 cases were already in a state of second-degree disability.(2)
Presented on Neuropathic Pain Congress - NeuPSIG 2015 | Nice, May 2015 2
Chronic pain that is not treated properly can cause negative effects on various aspects of life, including psychological and functional capacity of daily life.(4) Pain and the severity degree of pain has a significant correlation with physical functioning impairment, emotional functioning, social role functioning, sleep disturbances, and decreased quality of life (QoL).(5)
This study aims to determine the proportion and characteristics of NP in patients with MH, as well as to determine the correlation between NP with the QoL impairment in MH patients.
METHODS
This was a cross-sectional study with non random consecutive sampling method, conducted at the Dermatology Clinic of Sanglah Hospital and Indera Hospital in Denpasar Bali Indonesia, between January 2014 to March 2014. Subjects are MH patients who meet the inclusion and exclusion criteria, and willing to be respondent by signing the informed consent. Inclusion criteria of this study are: 1). MH patients. MH diagnosis was made based on clinical symptoms and examinations that was conducted by Dermatology Division (data taken from a medical record). 2). Patients who were cooperative and willing to participate in this study and sign the informed consent. The exclusion criteria of this study are: 1). Patients with second degree disabilities. 2). Patients with NP risk factors such as diabetes mellitus, use of alcohol, impaired renal function, malignant disease, other infectious diseases both locally and systemically.
MH is diagnosed by finding at least one of the following cardinal signs (6): 1). Loss of sensation in a hypopigmented or reddish skin patch. 2). Peripheral nerve enlargement, which is accompanied by loss of sensation and or accompanied by muscle weakness in
the area supplied by the nerve. 3). Presence of acid-fast bacili in a slit skin smear.
NP was diagnosed with DN4 instrument, which consists of seven items description of sensory and three items of sensory dysfunction examination. Scores ≥ 4 is classified as NP, and a score of <4 were classified as nosiceptive pain.(7)
QoL was evaluated by using SF-36 questionnaire, which contains 36 questions of eight domains. Adjusted final score will range from 0-100, zero reflects the worst QoL and 100 indicate the status of the best QoL. Score of ≤ 50 on each domain indicates the impairment of QoL. SF-36 scale is then divided into two dimensions, ie the mental component scale (MCS) and the physical component scale (PCS).(8)
The intensity of pain was assessed using Visual Analogue Scale (VAS). Patients were asked to mark on the horizontal line 10 cm (100 mm) in accordance with the perceived pain intensity, then it was measured. The pain intensity interpretation are: no pain (0-4 mm), mild pain (5-44 mm), moderate pain (45-74 mm), and severe pain (75-100 mm).(9)
Depression was evaluated using the Hamilton scale (Ham-D), which is interpreted as depression (score ≥7) and no depression (score <7).(10)
Data were analyzed with SPSS 20.0 for windows. Descriptive analysis was performed to determine the proportion and characteristics of the NP, and lambda test to determine the correlation between NP with the QoL impairment.
RESULTS
Presented on Neuropathic Pain Congress - NeuPSIG 2015 | Nice, May 2015 3
treatment (RFT). The subject characteristics are presented in Table 1.
Table 1 patients with NP. The most frequent type of NP was the sense of tingling (89,3%)with mild intensity (60.7%), the most frequent location was at the hands and feet (gloves and stockings) (75%), with the average of pain duration was 5.5 months (tabel 2).
Lambda test was used to determine the correlation between NP and QoL impairment. It can be seen that most of MH patients with impaired QoL are also experiencing NP (75%) (N = 21), and by using Lambda correlation test, it was obtained that r = 0.636. This value shows that there is a strong and positive correlation between NP and QoL impairment (p =
Characteristics of Neuropathic Pain
Characteristics N % Ulnar and Peroneal Nerve Auricular Nerve
Presented on Neuropathic Pain Congress - NeuPSIG 2015 | Nice, May 2015 4
DISCUSSION
The NP proportion in this study is quite high at 57.1%. This result is consistent with the study by Stump et al. (2004) in Brazil who got a proportion of 56.1%(11), Chen et al. (2012) in China got a proportion of 45.8%(12), and Reis et al. (2013) found the proportion of 66.3%.(13)
The proportion of QoL impairment in MH patients in this study was 44.9%. PCS was the most impaired dimension (95.5%); and the MCS impairment was only 27.3%. PCS consists of four domains: physical functioning, role of physical, bodily pain, and general health. MCS consists of four domains: mental health, vitality, social functioning, and role emotional. These findings are similar to the results of the study by Pratama (2011) who got the proportion of poor quality of life of 41.2%. A total of 76.5% of patients said that they have a poor physical health, and poor psychological state found only in 5.9% of the subjects.(14) Study by Mankar et al. (2011), which evaluates the level of QoL in MH patients by using the instrument WHOQOL-Bref, getting results that MH patients have lower levels of QoL than the control group.(15)
The most frequent type of pain that was obtained in this study was the tingling sensation (89.3%). Other type of pain is the pricking sensation (64.3%), burning sensation (60.37%), electric shock-like sensation (35.7%), and the least is the pressure sensation (17.9%). These results are consistent with the study by Chen et al. (2012), Lasry-Levy et al. (2011), and Saunderson et al. (2008) who also got that tingling sensation is the most frequent type of pain.(12,16,17) Subjects who have the pricking sensation type complained of limitations in physical activity due to the pain that is felt getting worse while doing strenuous or long duration activities. Most subjects with the burning sensation type also
have trouble to start sleeping because the pain is felt especially at night.
The most frequent pain location was the gloves and stockings type (75%). Similar results were also obtained by Lund et al. (2007) who get 71% of subjects with pain in the hands and feet, Hietaharju et al. (2000) got 62.5%, and Stump et al. (2004) got 47.3%.(18,19,11) Different results seen in the
study by Chen et al. (2012) who got the most frequent pain location on the ulnar nerve (79.4%), tibial nerve (42.1%), peroneal nerve (32.5%), and none of the patients complained of pain in the hands and feet.(12) In some theories, location of the damaged nerve can be associated with the type of MH which underlies the pathogenesis of nerve damage process. In tuberculoid type, nerve tissue damage is caused by the massive infiltration of lymphocytes that cause granulomatous reaction, thus forming epithelioid granulomas and fibrosis process in the epineurium. Nerve tissue damage is limited or local, so the clinical symptoms that appear is usually mononeuropathy, in accordance with the entrapped nerve by granuloma. In lepromatous type, the inflammatory response is not too massive so that the bacilli invasion into Schwann cells is asymptomatic, accompanied by a slow process of degeneration.
Presented on Neuropathic Pain Congress - NeuPSIG 2015 | Nice, May 2015 5
characteristics of this type is the formation of small granulomas in various locations according to the involved skin tissue and nerves. In addition, type 1 leprosy reactions are common in this type, that cause neuritis, and formed granulomas that will cause pressure on Schwann cells and cause early damage and nerve dysfunction. The clinical symptoms of this type is extensive, it can be multiple mononeuropathy or gloves and stockings type polyneuropathy.(20,21)
Most of the subjects complained of pain with mild intensity (60.97%), 39.3% with moderate intensity, and no subjects with severe pain intensity. This is differ from the results of previous studies. Chen et al. (2012) found the majority of subjects with severe pain intensity (55.5%); and Stump et al. (2004) found that 41.5% subjects have severe pain.(11,12)
Study by Reis et al. (2013), Haroun et al. (2012), Saunderson et al. (2008) and Lund et al. (2007) found the majority of patients with moderate pain.(13,17,18,22) These different results may be because in this study, patients with disability level 2 or with severe nerve damage has been excluded. The mean time duration of pain is of 5.5 months, ranged from 1 month to 24 months. Haroun et al. (2012) and Stump et al. (2004) found that most patients had NP for more than 6 months.(11,22) Hietaharju et al. (2000) and Lund et al. (2007) who assessed the characteristics of NP in patients who were RFT, get the result that most of the patients still feel pain until a few years after being RFT.(18,19) This results suggest that patients with MH tend to have chronic NP.
The sample consisted of 18 people who were RFT, and 12 of them have NP. This proves that NP can occur before, during, and even after treatment. NP in patients who have been declared RFT may occur due to the irreversible nerve damage complication that has occurred previously or because of leprosy reactions that still can arise for many
years after a patient completed MDT and generate new nerve damage. During MDT treatment, M. leprae die and disappear from the lesion. However, in the immunohistochemical examination, M. leprae antigens can still be found on the lesion for a very long time, and occasionally can stimulate the immune system response that resulting leprosy reactions and cause damage to nerve tissue.(23)
MH is still one of the dreaded disease because of the complications and the QoL impairment that it caused. Many factors can lead to the impaired QoL, including the skin lesions that interfere the patients appearance, the bad stigma of the disease, long treatment duration, recurring leprosy reactions, the disabilities, and the complication of chronic NP.
Proportion of the impaired QoL was 44.9% (N = 22), and 21 of them were also with NP. There is a significant strong positive correlation (p <0.005; r = 0.636) between NP and the impaired QoL. This means that the presence of NP will increase the likelihood of impaired QoL in MH patients. Reis et al. (2013) in his study found that the QoL domain that is most disrupted by the NP is the physical and the environment domain, and the pain intensity has a significant negative correlation with the low scores on psychological domain.(13)
Lasry-Levy et al. (2011) found 41% of patients with NP is also accompanied by psychological morbidity.(16) Study by Haroun et al. (2012) showed that the QoL of the MH patients with NP are also impaired, especially in the domain of ability to work and general activity.(22) Chen et al. (2012) found 40.5% of the subjects stated that the NP cause severe disruption to daily life.(12)
CONCLUSION
Presented on Neuropathic Pain Congress - NeuPSIG 2015 | Nice, May 2015 6
REFERENCES
1. Bhat, R.M., Prakash, C., 2012. Leprosy: An Overview of Patophysiology. Interdisciplinary Perspectives on Infectious Diseases, 2012: 1-6.
2. World Health Organization (WHO). 2011. Weekly Epidemiological Record. Leprosy Update, 38(36): 389-400.
Available from:
http://www.who.int/lep/en.
3. Rao, PN., Jain, S., 2013. Newer Management Options in Leprosy. Indian Journal of Dermatology, 58: 6-11.
4. Kvarnstrom, A. 2003. Neuropathic Pain; Quality of Life, Sensory Assessments and Pharmacological Treatments. Acta Universitatis Upsaliensis. Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1302. 107 pp. Uppsala. ISBN 91-554-5798-3.
5. Jensen TS, Baron R, Haanpää M, Kalso E, Loeser JD, Rice AS, Treede RD. 2011. A New Definition of Neuropathic Pain. Pain, 152:2204–2205.
6. World Health Organization (WHO). 2006. Global Strategy for Further Reducing the Leprosy Burden and Sustaining Leprosy Control Activities (2006-2010).
7. Bennet, M.I., Attal, N., Backonja, MM., Baron, R., Bouhassira, J., 2007. Using Screening Tools to Identify Neuropathic Pain. Journal Pain, 127: 199-203.
8. Jenkinson, C., Brown, S.S., Petersen, Sophie., Paice, C. 1999. Assessment of the SF-36 version 2 in the United Kingdom. J Epidemiol Community Health, 53: 46-50.
9. Hawker, GA., Mian, S., Kendzerska, T., French, M., 2011. Measures of Adult Pain. Arthritis Care & Research, 63: S240-S252.
10.Scharg, A., Baroke, P., Brown, R.G., dkk. 2007. Depression Rating Scales in
Parkinson’s Disease: Critique and Recommendations. Movement Disorder, Vol.22(8): 1077-1092.
11.Stump, PR., Baccarelli, R., Marciano, LH., Lauris, JRP., Teixeira, MJ., Ura, S., Virmond, MCL., 2004. Neuropathic Pain in Leprosy Patients. International Journal of Leprosy, 72(2): 134-138. 12.Chen, S., Qu, J., Chu, T., 2012.
Prevalence and characteristics of neuropathic pain in the people affected by leprosy in China. Lepr Rev, 83: 195-201.
13.Reis, JJF., Gomes, MK., Rodrigues, J., Gosling, AP., Fontana, AP., Cunha, JLA., 2013. Pain and Its Consequences in Quality of Life: A Study with WHOQOL-Bref in Leprosy Patients with Neuropathic Pain. ISRN Tropical Medicine, 2013: 1-7.
14.Pratama, S.E., 2011. Tingkat Kualitas Hidup Pasien Kusta yang Datang Berobat ke RSUD Dr. Pirngadi Medan September-Oktober 2011. Available from:
http://repository.usu.ac.id/bitstream/123 456789/21538/5/Chapter%201.pdf. (Accessed: 2013 November 16).
15.Mankar, M.J., Joshi, S.M., Velankar, D.h., Mhatre, R.K., Nalgundwar, A.N. 2011. A comparative study of the quality of life, knowledge, attitude and belief about leprosy disease among leprosy patients and community members in shantivan leprosy rehabilitation centre, Nere, Maharashtra, India. Journal of Global Infectious Disease, 3(4): 378-382.
Presented on Neuropathic Pain Congress - NeuPSIG 2015 | Nice, May 2015 7
17.Saunderson, P., Bizuneh, E., Leekassa, R., 2008. Neuropathic pain in people treated for multibacillary leprosy more than ten years previously. Lepr Rev, 79: 270-276.
18.Lund, C., Koskinen, M., Suneetha, S., Lockwood, DNJ., Haanpaa, M., Haapasalo, H., Hietaharju, A., 2007. Histopathological and clinical findings in leprosy patients with chronic neuropathic pain: a study from Hyderabad, India. Lepr Rev, 78: 369-380.
19.Hietaharju, A., Croft, R., Alam, R., Birch, P., Mong, A., Haanpaa, M., 2000. Chronic neuropathic pain in treated leprosy. The Lancet, 356: 1080-1081. 20.Haanpaa, M., Lockwood, DNJ.,
Hietaharju, A., 2004. Neuropathic pain in leprosy. Lepr Rev, 75: 7-18.
21.Job, CK., 2001. Pathology and pathogenesis of leprous neuritis; a preventable and treatable complication. International Journal of Leprosy, 69(2): 19-29.
22.Haroun, OMO., Hietaharju, A., Bizuneh, E., Tesfaye, F., Brandsma, JW., Haanpaa, M., Rice, ASC., Lockwood, DNJ., 2012. Investigation of neuropathic pain in treated leprosy patients in Ethiopia: A cross-sectional study. Pain, 153: 1620-1624.