Effect of hypertension and risk factors on diameters of abdominal
aorta and common iliac and femoral arteries in middle-aged
hypertensive and control subjects
A cross-sectional systematic study with duplex ultrasound
Markku J. Pa¨iva¨nsalo
a,*, Jukka Merikanto
a, Tapani Jerkkola
b,c,
Markku J. Savolainen
b,c, Asko O. Rantala
b,c, Heikki Kauma
b,c, Mauno Lilja
b,c,
Antti Reunanen Y.
d, Antero Kesa¨niemi
b,c, Ilkka Suramo
aaDepartments of Diagnostic Radiology,Uni6ersity of Oulu,FIN-90220,Oulu,Finland bDepartment of Internal Medicine,Uni6ersity of Oulu,FIN-90220,Oulu,Finland
cBiocenter Oulu,Uni6ersity of Oulu,FIN-90220,Oulu,Finland
dSocial Insurance Institution Research and De6elopment Unit,FIN-00381Helsinki,Finland
Received 30 April 1999; received in revised form 22 November 1999; accepted 5 January 2000
Abstract
There is a general tendency towards atherosclerosis and arterial dilatation in older age, and high blood pressure also tends to increase arterial diameters. The purpose of this study was to examine the effect of hypertension and other cardiovascular risk factors on aortic, common iliac and common femoral artery diameters. The diameters of the abdominal aorta and the iliac and femoral arteries and the extent of echogenic plaques in the aorta and the iliac arteries down to groin level were evaluated with ultrasound in 1007 middle-aged (40 – 60 years) men (505) and women (502), 496 with arterial hypertension and 511 controls. Twenty-eight subjects were excluded because of poor visualization. Men had significantly larger diameters of the abdominal aorta (mean 21.392.8 vs. 17.891.3 mm) and the common iliac (13.492.0 vs. 12.291.2) and common femoral arteries (11.091.4 vs. 9.790.9) than women (Pfor all B0.001), but arterial diameter was also related to the subject’s size. Atherosclerotic plaques, age and height were associated with the diameter of the abdominal aorta in men, while high body mass index (BMI) had less significance. The diameter of the aorta was larger in hypertensive men aged 56 – 60 than in controls of the same age. In women, height, BMI and diastolic blood pressure (DBP) were associated with the diameter of the aorta, while systolic blood pressure (SBP) had less and age no effect. Age, plaques, height, BMI, DBP and SBP were associated with the diameters of the common iliac arteries in both genders, while smoking had an inverse correlation. The results on lipid values were inconsistent and an abnormal glucose tolerance test proved nonsignificant. In conclusion, arterial size measured as a diameter related to the subject’s size was larger in men. Age, arterial plaques and blood pressure increased arterial diameter significantly. However, the hypertensive disease itself had only a minimal effect. The changes were smaller in women than in men. © 2000 Elsevier Science Ireland Ltd. All rights reserved.
Keywords:Ultrasound; Aorta; Iliac arteries; Plaques; Diameters; Hypertension
www.elsevier.com/locate/atherosclerosis
1. Introduction
Ultrasound (US) often shows plaques in the abdomi-nal aorta and the iliac and femoral arteries as signs of atherosclerosis, which may sometimes result in arterial obliteration, dilation or aneurysm [1]. There is a general
tendency towards arterial dilation in older age [2 – 5]. The purpose here was to examine the effect of hyper-tension and other risk factors on the diameters of the aorta and the common iliac and common femoral arteries in a population-based series of randomly (age-stratified) selected 40- to 60-year-old men and women with an established diagnosis of arterial hypertension, and controls.
* Corresponding author. Fax: +358-8-3155420.
2. Methods
2.1. Population
From the defined population of the City of Oulu, treated hypertensive patients of both sexes aged 40 – 60 years and age- and sex-matched controls were recruited for carotid [6] and abdominal ultrasound examinations as part of a survey on the cardiovascular risk factors (OPERA, Oulu Project Elucidating the Risk of Atherosclerosis). The treated hypertensives (300 men and 300 women) were randomly selected from the Social Insurance Institute’s register for the reimburse-ment of antihypertensive medication, and the controls from the same organization’s register of all inhabitants of the City of Oulu (about 100 000 persons) as de-scribed in detail previously [7]. The initial population consisted of 1200 subjects. The overall participation rate was 85.9%, and the aorta and the iliac arteries were examined in 1007 subjects, i.e. 505 men, 502 women, 496 with arterial hypertension and 511 controls.
The procedure for blood pressure measurement was in agreement with the American Society of Hyperten-sion [8]. All blood pressure measurements were recorded with an automatic oscillometric blood pres-sure recorder (Dinamap; Critikon, Ascot, UK). The resting blood pressure was measured three times at 1-min intervals on the right arm after patient had been seated for at least 5 min. The mean of the three sitting blood pressure measurements was used in the analysis. BMI was calculated as weight in kilograms divided by height in square meters. Details about the smoking habits, alcohol consumption, use of medications, and past medical history were sought in a questionnaire. A wide range of laboratory analyses were conducted. Af-ter the fasting blood had been drawn, the subjects were given a 75-g glucose load. Both 1- and 2-h glucose and insulin concentrations were determined. The glucose concentrations were measured with the glucose dehy-drogenase method (Diagnostica; Merck, Darmstadt, Germany). Plasma lipids and lipoproteins were ana-lyzed as described in the Lipid Research Clinic Pro-gram’sManual of Laboratory Operations [9].
The mean duration of hypertension was 6.9 years (SD 4.7 years, range 0.15 – 32.6 years). Of the hyperten-sive subjects, 262 were on selective b-blocking medica-tion, 210 on angiotensin-converting enzyme inhibitors, 190 on thiatzide diuretics, 125 on calcium channel blockers and 31 on non-selectiveb-blocking medication and loop diuretics, 294 women were postmenopausal.
2.2. Ultrasonography of aorta and iliac arteries
The data were collected over a period of 2 years. The ultrasound examination of the aorta and iliac arteries was carried out, using a duplex ultrasound system
(Toshiba Sonolayer SSD 270) with a scanning fre-quency of 5 MHz, by a single trained radiologist blinded to the presence or absence of hypertension and following the same protocol throughout. The abdomi-nal aorta and the common iliac and femoral arteries were imaged longitudinally and transversally. The whole scanning procedure was recorded on a Super-VHS video casette recorder (Panasonic). The videotapes were analyzed later. The same radiologist (MP) who performed the examinations made the mea-surements from the videotapes for the 380 successively youngest men, and another trained radiologist (JM) made the measurements for the other men and for all women. Twenty-eight of the 1007 subjects were ex-cluded because of poor visualization of the aorta and the iliac arteries.
All measurements were made about 4 years later from the video image on the monitor of the ultrasound device, using its electronic calipers. The maximal outer diameter (lumen plus wall thicknesses) of the lower abdominal aorta was measured in the sagittal and transverse planes and the maximal diameters of both common iliac arteries and both common femoral arter-ies in the groin in the sagittal plane. An arterial plaque was defined as a highly or moderately echodense struc-ture encroaching into the vessel lumen. Atherosclerosis was estimated on the basis of the plaques detected. The number of plaques was recorded and the length of each was measured as the maximal diameter from longitudi-nal ultrasound scans of the aorta and the iliac arteries between the level of the renal arteries and the inguinal ligament.
The moving mean technique [10] was used to assess the association of the diameters with increasing age, and the data on one third of the subjects in the overlap-ping subgroups were used to calculate the mean. Age was determined as of the day of the examination. The results were also calculated separately for the age classes of 40 – 45 years, 46 – 50 years, 51 – 55 years and 56 – 60 years. The diameters were correlated with sex, age and disease (hypertension/control) and other risk factors.
The method of Fleiss [11,12] was used to calculate interobserver variability. First, the variance of measure-ments in one plane by the two observers was calculated using the formula: (M1)
the videotapes 1 year after the subjects’ examinations, reader blinded to the original result. The intrareader variability/correlation coefficients (Pearson’s coeffi-cient) for the vessel diameters were: 3.7%/0.88 for the sagittal aortic diameter, 5.8%/0.72 for the transverse aortic diameter, 8.3%/0.78 for the iliac and 5.2%/0.86 for the femoral arterial diameters. The corresponding interreader values were: 4.5%/0.86 for the sagittal aortic diameter, 6.5%/0.71 for the transverse aortic diameter, 8.7%/0.76 for the iliac and 6.9%/0.89 for the femoral arterial diameters.
2.3. Statistical analyses
The data were analysed with the SystatTM statistical program [13], which estimated the dependence of the diameters on age by means of correlation analysis. The data are presented as means9SD values, unless other-wise stated. Thex2test was used to test the differences in frequencies, and Student’s two-tailed t-test for inde-pendent samples to compare two groups. P-values B 0.05 were considered statistically significant. The arterial diameters were related to the risk factor vari-ables in multivariate stepwise linear regression analysis by backward elimination. Only the variables significant at P50.15 were retained in the equation.
3. Results
The clinical data are presented in Table 1. Table 2 shows the arterial diameters in the male and female cohorts. Men had significantly larger diameters of the aorta (mean sagittal diameter 20.392.8 vs. 17.291.3 mm) and the common iliac (13.392.0 vs. 12.291.3) and common femoral arteries (11.091.5 vs. 9.791.0) than women (P for all B0.001). The transversal aortic diameters were larger than the sagittal ones, the former being 22.293.0 mm for men and 18.491.4 mm for women (PB0.001). The arterial diameters were more
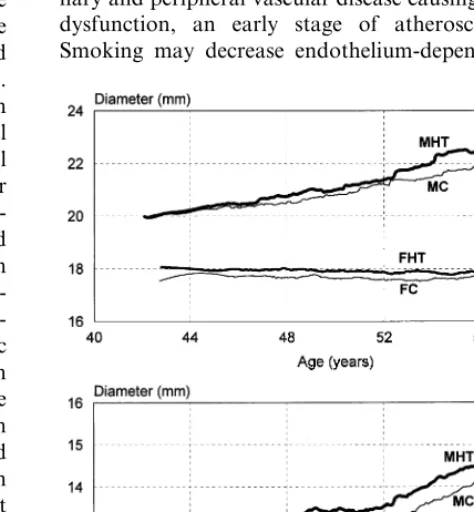
closely related to body height in women than in men. The diameters of the aorta in men and those of the common iliac and femoral arteries both in men and in women appeared to enlarge with age (Tables 2 and 3) (Fig. 1.). The aortic diameter was larger in hypertensive men aged 56 – 60 than in control men of the same age (Table 2) (Fig. 1). The mean aortic diameter was larger than the mean plus 2 SD (20.0 mm) in 2.5% of the control women aged 40 – 50 and, in 2.9% of those aged 51 – 60 years, and the corresponding percentages for hypertensive women were 3.0% and 1.5%. In the corre-sponding age groups of men, the aortic diameter ex-ceeded the mean plus 2 SD (25.4 mm) in 0.8% (40 – 50 years) and 3.9% (51 – 60 years) of the controls and in 0.8 and 7.0% of the corresponding hypertensives. In the common iliac arteries, the percentages for the same age groups were 1.3%/5.1% (mean+2 SD\14.6 mm) (con-trol women), 4.5%/8.0% (hypertensive women), 0.4%/ 5.8% (mean+2 SD\17.2 mm) (control men) and 1.6%/12.3% (hypertensive men). Hypertensive women in the age groups of 40 – 45 and 46 – 50 years had significantly larger common iliac and common femoral arteries than the controls. Obesity was significantly associated with arterial diameter and also with blood pressure (Table 3). The effect of lipid values, however, was nonsignificant. The diameters of the aorta in men and the diameters of the common iliac arteries in both men and women correlated well with the amount of plaques, which increased with age (Table 3) (Fig. 2). Hypertensive subjects had a larger plaque extent than controls, especially older women with a long duration of hypertension. The mean sum of plaque lengths in the aorto – iliac area was 79 mm in control and 107 mm in hypertensive women, and 100 mm in control and 104 mm in hypertensive men. Non-smoking men had sig-nificantly wider common iliac and common femoral arteries and slightly wider aortas than smoking men, and non-smoking women had only slightly wider com-mon iliac and comcom-mon femoral arteries than smoking women, but smoking women had wider aortas than non-smoking women (Fig. 3).
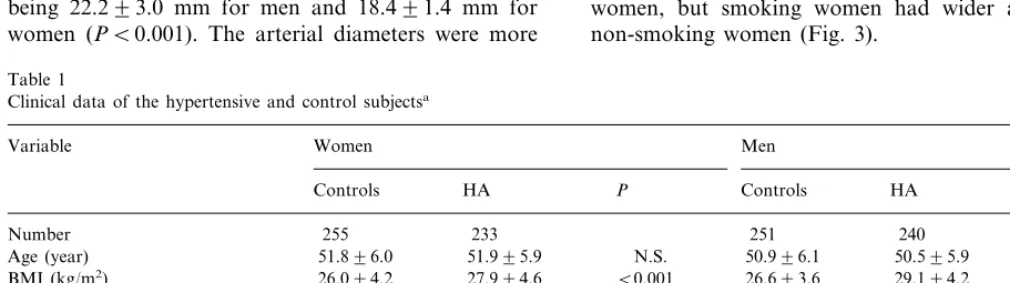
Table 1
Clinical data of the hypertensive and control subjectsa
Women
Variable Men
Controls HA P Controls HA P
255 233
SBP (mm Hg) 147920 159921 B0.001
83913 91911 B0.001
DBP (mm Hg) 89910 97910 B0.001
4.799.2 5.0910.6 N.S.
Smoking (pack- years) 16.1914.2 15.3913.6 N.S.
5.891.0 N.S. 5.791.1 N.S.
Total cholesterol (mmol/l) 5.591.0 5.891.1
HDL cholesterol (mmol/l) 1.5390.39 1.4590.38 0.016 1.2390.30 1.1990.32 N.S.
Triglycerides (mmol/l) 1.191.6 1.391.6 B0.001 1.491.6 1.791.6 B0.001
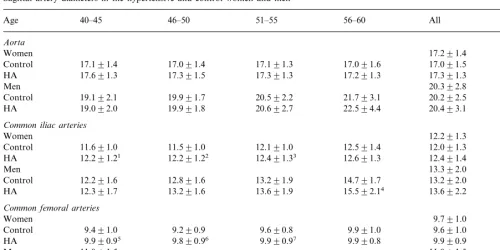
Table 2
Sagittal artery diameters in the hypertensive and control women and mena
Age 40–45 46–50 51–55 56–60 All Pb
Aorta
Women 17.291.4
17.091.4 17.191.3 17.091.6
17.191.4 17.091.5
Control
17.391.5 17.391.3 17.291.3
HA 17.691.3 17.391.3 0.022
20.392.8 Men
19.991.7
Control 19.192.1 20.592.2 21.793.1 20.292.5
19.991.8 20.692.7 22.594.4
19.092.0 20.493.1
HA 0.574
Common iliac arteries
12.291.3 Women
11.591.0 12.191.0 12.591.4 12.091.3
Control 11.691.0
12.291.22 12.491.33 12.691.3
12.291.21 12.491.4
HA B0.001
Men 13.392.0
12.891.6 13.291.9 14.791.7
12.291.6 13.292.0
Control
13.291.6 13.691.9 15.592.14 13.692.2
HA 12.391.7 0.007
Common femoral arteries
Women 9.791.0
9.290.9
Control 9.491.0 9.690.8 9.991.0 9.691.0
9.890.96 9.990.97 9.990.8
9.990.95 9.990.9
HA B0.001
Men 11.091.5 11.091.5
10.691.2 10.791.3 11.891.2
10.591.3 10.991.5
Control
10.891.2 11.191.2 12.191.6
HA 10.491.3 11.191.5 0.058
aValues are means9SD. Difference between hypertensives and controlst-test.
bSignificant differences between hypertensives and controls in subgroups:1P=0.004;2PB0.001;3P=0.035;4P=0.001;5P=0.001;6PB0.001; 7P=0.029.
4. Discussion
Duplex ultrasound is commonly used to diagnose aneurysms of the abdominal aorta by measuring its diameter. The variation in the measurements of the anteroposterior diameters of abdominal aortic aneu-ryms has been 2.2 – 8 mm [14,15]. In the series by Yucel et al. [11], the interobserver variability of the anteropos-terior measurement was 2.53 mm, which accounts for 7% of the mean diameter. In accordance with previous studies, interobserver variability was also larger for transverse measurements in our study, probably due to the superior axial compared to lateral resolution [11,14,15]. Our variability percentages were also com-parable to the previous results [11,16,17]. The in-trareader variabilities presented in millimeters in our series were 0.73 and 1.3 mm for the aortic sagittal and transverse measurements. The values are small because our series consisted of subjects with normal aortas compared to the series with aortic aneurysms [11]. The intra/interreader correlation coefficients were naturally poorer than in our carotid series [6], because of the smaller diameters of the aorta and the iliac vessels in relation to the ultrasound image, which leads to a poorer measurement accuracy compared to the carotid image.
The aortic diameter increases with age, being larger in men [18 – 20]. In a multivariate analysis, including age, height, body weight and sex, the distal aortic
diameter correlated only with age and sex in the series by Pedersen et al. (1993) [5]. According to our contra-dictory results, age had no effect on the female aortic diameter, but in men the diameter was significantly enlarged. However, the diameters of the common iliac and common femoral arteries slightly increased over age among women, while the corresponding increase in men was clearly higher.
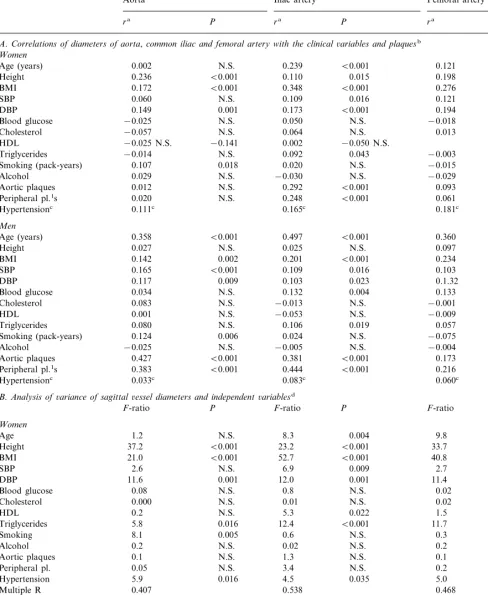
Table 3
A.Correlations of diameters of aorta,common iliac and femoral artery with the clinical 6ariables and plaquesb
Women
0.002 N.S. 0.239 B0.001 0.121 0.007
Age (years)
B0.001
0.236 0.110 0.015 0.198 B0.001
Height
Triglycerides −0.014 N.S. N.S.
0.020 N.S. −0.015
Peripheral pl.1s 0.020 N.S. N.S.
0.165c 0.181c
Height 0.027 N.S. 0.025 N.S. 0.097 0.031
0.201 B0.001 0.234
0.034 0.132 0.004 0.133 0.003
Blood glucose
Triglycerides 0.080 N.S. 0.106 0.019 0.057 N.S.
0.024 N.S. −0.075
0.006 N.S.
Smoking (pack-years) 0.124
−0.005 N.S. −0.004
Alcohol −0.025 N.S. N.S.
0.381 B0.001 0.173
B0.001 B0.001
Aortic plaques 0.427
0.444
Peripheral pl.1s 0.383 B0.001 B0.001 0.216 B0.001
0.083c 0.060c
0.033c
Hypertensionc
B.Analysis of6ariance of sagittal 6essel diameters and independent6ariablesd
P F-ratio P F-ratio P
11.6 12.0 0.001 11.4 0.001
DBP
Aortic plaques 0.1 N.S. N.S.
3.4 N.S. 0.2
SBP 0.16 N.S. 8.8 0.003 11.8 0.001
6.6 0.010 12.9 B0.001
Table 3 (Continued)
Variables Diameter
Iliac artery
Aorta Femoral artery
P ra
ra P ra P
N.S. 0.02 N.S. 0.7 N.S.
Blood glucose 3.6
N.S. 1.8 N.S.
0.4 0.008
Cholesterol N.S.
0.9
HDL N.S. 0.002 N.S. 0.07 N.S.
N.S. 0.8 N.S.
Triglycerides 0.6 2.9 N.S.
N.S. 9.1 0.003
0.02 8.6
Smoking 0.004
1.8
Alcohol N.S. 0.2 N.S. 0.05 N.S.
B0.001 0.4 N.S. 0.3
Aortic plaques 23.7 N.S.
N.S. 35.6 B0.001
3.8 8.1
Peripheral pl. 0.005
0.15
Hypertension N.S. 1.1 N.S. 0.4 N.S.
Multiple R 0.543 0.642 0.522
aCorrelation coefficient (Pearson).
bBlood glucose: 2 h blood glucose.1Peripheral pl., sum of plaque lengths in the common and external iliac arteries; aortic plaques=sum of
plaque lengths in the aorta.
cSpearman’s coefficient.
dLinear parameters: age, height, BMI, SBP, DBP, alcohol consumption, smoking (pack-years), cholesterol, HDL, triglycerides, 2 h blood
glucose value at glucose tolerance test; categorical parameters: hypertension (0=no, 1=yes).
mm. When the mean aortic diameter was calculated in the control subjects, the diameter was larger than the mean plus 2 SD more often in hypertensives than in controls, especially in older subjects (50 – 60 years), in the iliac arteries of both genders and in the aortas of men. Human arteries dilate in response to progressive atherosclerosis, as was also seen in our series, where aortic dilatation was associated with aortic plaques and iliac and femoral dilatation with plaques in these vessels. This compensatory mechanism results in an increase in arterial size that is proportionate to the cross-sectional area of plaques that have accumulated in the vessel [21,22]. Atherosclerosis may also lead to obliteration or occlusion of arteries. Atherosclerosis is the etiopatho-logic cause of about 90% of the aortic aneurysms found in elderly subjects, in men, in smokers and in subjects in poor health (defined as concurrent hypertension, cardio-vascular disease or diabetes mellitus) [23 – 25]. The defi-nitions of abdominal aortic aneurysm based on the aortic diameter vary [3,26 – 30]. The most widely used definition is maximal sagittal diameter ]30 mm [26,27,31]. The reported prevalence of abdominal aortic aneurysms in subjects aged 50 years and older varies between 1.4 and 8.8% [32 – 34]. An aneurysm was found in 8.8% of men and in 2.1% of women]50 years referred for their first abdominal ultrasonography without any suspicion of aneurysm [32]. The prevalence in patients with symp-tomatic peripheral or cerebral arterial disease may be as high as 11.2% (men) and 6.4% (women) [35]. We found an aneurysm (diameter ]3.0 cm) in 1.4% of men aged 40 – 60 (2.4/1.2% in control men and 3.8/1.7% (dilatation/ aneurysm) in hypertensive men), but none in the women. Aneurysms in the iliac arteries are rare.
In multiple regression analysis, high blood pressure
increased arterial diameter. The diagnosis of hyperten-sion in regreshyperten-sion analysis had a nonsignificant effect on arterial diameter in men, even when SBP/DBP was ignored, and a minimal effect in women.
Long-term smoking is a primary risk factor for coro-nary and peripheral vascular disease causing endothelial dysfunction, an early stage of atherosclerosis [36]. Smoking may decrease endothelium-dependent
Fig. 2. Moving mean curves showing the sagittal diameters of the aorta (A) and the common iliac artery (B); FNP, females without plaques; FP, females with plaques; MNP, men without plaques; MP, men with plaques.
common iliac and common femoral arteries were smaller in smokers compared to nonsmokers in our series. Lipid values did not have a significant effect on arterial diameters.
Arterial size, measured as a diameter related to the subject’s size, was higher in men. The significant risk factors increasing arterial diameter were age, atherosclerosis and blood pressure. However, hyperten-sive disease itself had only a minimal effect. The changes were smaller in women than in men.
References
[1] Hoogendam IJ, van Rinsum AC, Olyslager J. The diameter of the distal abdominal aorta and the etiology of local atheroma. J Cardiovasc Surg 1984;25:408 – 13.
[2] Horejs D, Gilbert PM, Burstein S, Vogelzang RL. Normal aortoiliac diameters by CT. J Comput Assist Tomogr 1988;12:602 – 3.
[3] Lucarotti ME, Shaw E, Heather BP. Distribution of aortic diameter in a screened male population. Br J Surg 1992;79:641 – 2.
[4] Macchi C, Giannelli F, Catini C, Gulisano M, Pacini P, Brizzi E. The original calibre of the lower limbs arteries as a possible risk factor for complications of atherosclerosis: a statistical investiga-tion in 90 subjects by echocolordoppler. J Anat Embryol 1994;99:219 – 28.
[5] Pedersen OM, Aslaksen A, Vik-Mo H. Ultrasound measurement of the luminal diameter of the abdominal aorta and iliac arteries in patients without vascular disease. J Vasc Surg 1993;17:596 – 601.
[6] Paivansalo M, Rantala A, Lilja M, Reunanen A, Kesaniemi YA, Suramo I. Prevalence of carotid atherosclerosis in middle-aged hypertensive and control subjects. A cross-sectional system-atic study with duplex ultrasound. J Hypertens 1996;14:1433 – 9.
[7] Kiema T-R, Kauma H, Rantala AO, Lilja M, Reunanen A, Kesa¨niemi YA, Savolainen MJ. Variation at the angiotensin-converting enzyme gene and angiotensinogen gene loci in rela-tion to blood pressure. Hypertension 1996;28:1070 – 5.
[8] American Society of Hypertension: Recommendations for rou-tine blood pressure measurement by indirect cuff sphygmo-manometry. Am J Hypertens 1992;5: 207 – 209.
[9] Manual of Laboratory Operations, Lipid Research Clinics Pro-gram. Lipid and Lipoprotein Analysis. Washington, DC, U.S. Govt. Printing Office, 1974, p. 51 – 59 (DHEW publ. no. [NIH] 75 – 628).
[10] Madrikakis S, Wheelright S, McGee V. Smoothing methods. In Forecasting: Methods and Applications. New York:Wiley, 1983, pp. 62 – 129.
[11] Yucel EK, Fillmore DJ, Knox TA, Waltman AC. Sonographic measurement of abdominal aortic diameter: interobserver vari-ability. J Ultrasound Med 1991;10:681 – 3.
[12] Fleiss JL. The Design and Analysis of Clinical Experiments. New York: Wiley, 1986:39.
[13] Systat for Windows, Version 5, Statistics, Systat Inc., 1992 [14] Ellis M, Powell JT, Greenhalg RM. Limitations of
ultrasonogra-phy in surveillance of small abdominal aortic aneurysms. Br J Surg 1991;78:614 – 6.
[15] Akkersdijk GJM, Puylaert JBCM, de Vries AC. Accuracy of ultrasonographic measurement of infrarenal abdominal aortic aneurysm. Br J Surg 1994;81:376.
Fig. 3. Moving mean curves showing the sagittal diameters of the aorta (A) and the common iliac artery (B) according to smoking status and gender. FNS, non-smoking females; FS, smoking females; MNS, non-smoking men; MS, smoking men.
[16] Persson J, Stavenow L, Wikstrand J, Israelsson B, Formgren J, Berglund G. Noninvasive quantification of atherosclerotic le-sions. Arterioscler Tromb 1992;12:261 – 6.
[17] Riley WA, Barnes RW, Applegate WB, Dempsey R, Hartwell T, Davis VG, et al. Reproducibility of noninvasive ultrasonic mea-surement of carotid atherosclerosis. Stroke 1992;23:1062 – 8. [18] Dixon AK, Lawrence JP, Mitchell JRA. Age-related changes in
the abdominal aorta shown by computed tomography. Clin Radiol 1984;35:33 – 7.
[19] Pearce WH, Slaughter MS, LeMaire S, Salyapongse AN, Fein-glass J, McCarthy WJ, Yao JST. Aortic diameter as a function of age, gender and body surface area. Surgery 1993;114:691 – 7. [20] Sonesson B, La¨nne T, Hansen F, Sandgren T. Infrarenal aortic
diameter in the healthy person. Eur J Vasc Surg 1994;8:89 – 95. [21] Losordo DW, Rosenfield K, Kaufman J, Pieczek A, Isner M.
Focal compensatory enlargement of human arteries in response to progressive atherosclerosis. In vivo documentation using in-travascular ultrasound. Circulation 1994;89:2570 – 0.
[22] Steinke W, Els T, Hennerici M. Compensatory carotid artery dilatation in early atherosclerosis. Circulation 1994;89:2578 – 81. [23] Amati G, Silver MD. Atherosclerosis of aorta and its complica-tions. In: Silver MD, editor. Cardiovascular Pathology. New York: Churchill Livingstone, 1991.
[24] Wolf YG, Otis SM, Schwend RB, Bernstein EF. Screening for abdominal aortic aneurysms during lower extremity arterial eval-uation in the vascular laboratory. J Vasc Surg 1995;22:417 – 23. [25] Krohn CD, Kullmann G, Kvernebo K, Rose´n L, Kroese A. Ultrasonographic screening for abdominal aortic aneurysm. Eur J Surg 1992;158:527 – 30.
[26] Scott RAP, Ashton HA, Kay DN. Abdominal aortic aneurysm in 4237 screened patients patients: prevalence, development and management over 6 years. Br J Surg 1991;78:1122 – 5.
[27] Holdsworth JD. Screening for abdominal aortic aneurysm in Northumberland. Br J Surg 1994;81:710 – 2.
[28] Johnston KW, Rutherford RB, Tilson MD, Shah DM, Hollier L, Stanley JC. Suggested standards for reporting on arterial aneurysms. J Vasc Surg 1991;13:452 – 8.
[29] Allardice JT, Allwright GJ, Wafula JMC, Wyatt AP. High prevalence of abdominal aortic aneurysm in men with peripheral vascular disease: screening by ultrasonography. Br J Surg 1988;75:240 – 2.
[30] Shapira OM, Psik S, Wasserman JP, Barzilai N, Mashiah A. Ultrasound screening for abdominal aortic aneurysms in patients with atherosclerotic peripheral vascular disease. J Cardiovasc Surg (Torino) 1990;31:170 – 2.
[31] The UK small aneurysm trial participants. The UK small aneu-rym trial: design, methods and progress. Eur J Vasc Endovasc Surg 1995;9:42 – 8.
[32] Akkersdijk GJM, Puylaert JBCM, deVries AC. Abdominal aor-tic aneurysm as an incidental finding in abdominal ultrasonogra-phy. Br J Surg 1991;78:1261 – 3.
[33] Pleumeekers HJCM, Hoes AW, vaderDoes E, VanUrk H, Grobbee DE. Epidemiology of abdominal aortic aneurysms. Eur J Vasc Surg 1994;8:119 – 28.
[34] Collin J, Araujo L, Walton J. A community detection program for abdominal aortic aneurysm. Angiology 1990;41:53 – 8. [35] MacSweeney STR, O’Meara M, Alexander C, O’Malley MK,
Powell JT, Greenhalg RM. High prevalence of unsuspected abdominal aortic aneurysm in patients with confirmed symp-tomatic peripheral or cerebral arterial disease. Br J Surg 1993;80:582 – 4.
[36] Heitzer T, Just H, Munzel T. Antioxidant vitamin C improves endothelial dysfunction in chronic smokers. Circulation 1996;94:6 – 9.
[37] Woo KS, Robinson JT, Chook P, Adams MR, Yip G, Mai ZJ, Lam CW, Sorensen KE, Deanfield JE, Celermajer DS. Differ-ences in the effect of cigarette smoking on endothelial function in Chinese and white adults. Ann Intern Med 1997;127:372 – 5.