Vol 5, No 4, October - December 1996 IgM Anti Phenolic Glycolipid
I
203Schoolchildren Survey and Community Survey
for
The
Determination
of
Seroprevalence Against
IgM Anti
Phenolic
Glycolipid-I Antibody
in
Leprosy
Endemic Areas, South Sulawesi, Indonesia
A
Comparative Study
Mochammad Hatta
Abstrak
Padapenelitian ini dilaporkan tentang kegunaan IgM antiphenolic glycolipid-l (PGL-I) denganmenggunakan tes Mycobacterium leprae particle agglutination (MLPA) pada survei anak sekotahyang dibandingkan dengan survei penduduk pada daerah endemik lepra di Indonesia. Dua desa dengan jumlnh keseluruhan registrasi penduduk masing-masing 1729 dan 3077 orang dipilih untuk menentukan seroprevalensi pada tiap desa tersebut.
Dari
510 dan 1496 orang yang diperil<sa, ditemulan 18.4 Vo dan 40.4 7o seropositif antibodi IgM terhadap PGL-|. Delapan puluh dan 44 anak sekolah dari dua desa yang sama diperilcsa dan ditemukan masing-1naslng 17.6 Vodan 40.9 Vo seropositif. Tidak ada perbedaan yang bermakna dalam seroprevalensi antara anak selcolah dan jumlah kes)luruhan penduduk yang diperiksa
dari
masing-masing desa. Sebagai kesimpulan ialah survei anak sekolah berguna untuk menentukan seroprevalensi terhadap infeksi lepra dan menggambarkan besarnya seroprevalensi populasi penduduk pada tingkat desa.Abstract
This study rePorts on the usefulness of IgM anti phenolic glycolipid-l (PGL-I) antibody detection using Mycobacterium leprae particle agglutination (MLPA) test in a schoolchildren survey comparedwith a community surtey
in
leprosy endemic areas, Indonesia. Two villages with total registered persons 1729 and 3077 respectively were chosen to determine the seroprevalence ofeach village. Among 510 and 1496 examined persons in a population survey it tumed ou[ that ]8.4 Vo and 40.4 Vo respectively were seropositive to IgM anti PGL-l antibody. In 80 and44 examined schoolchildrenof the same respective areas 17.6 Vo and 40.9 Vo werefound seropositive.No significant
dffirence
on seroprevalence was found between schoolchildren and community surtey in each village. In conclusion, schoolchildren survey may be useful in determining the seroprevalence of leprosy infection and reflect the magnitude of seroprevalence among a population in a leprosy endemic area at village level.Keyworils : IgM anti phenolic glycolipid-L, MLPA, Seroprevalence, Izprosy
Leprosy is
achronic infectious
diseaseby
Mycobac-terium leprae and
afflict
an estimated 5.5 million
peoplein
theworld.r M. l"pro"can
beidentified by the
presenceof
a
sppcific
polymerase chain
reacrion(PCR;Z3'a
and
y"oitpiO-t (PGL-I)
asspecific
antigenepitope.
antigens havebeendeveloped
as aserological
tool for leprosy
andMyco-bacteriumleprae
particle agglutination
(MLPA)
test is anew test using
sensitizfd
gelatin
particle
to detect
Ig
M
anti
PGL-I
antibody.o
Among
the
major infectious
diseases,
leprosy
isprobably
the leastwell
understood asto its
epidemiol-ogy7. Our knowledge
of
the natural history
of
thedisease is also
very
limited.
Previously,
theMLpA
testhas been evaluated as a
tool
in
the
epidemiology
of
leprosy
in
high prevalence villages
in
SouthSulawesi,
lndonesia. Our results revealed that most of thepopula-M. leprae
was3l
.9 Vo,i.e.positive
antibodies.oIt
is
commonly believed that most individuals
will
becomeinfected
byM. leprae
after
sufficient
duration
of
contact
with leprosy
patients,
but
it
seems thatin
most casesof infection,
symptoms
fail
to develop.g
Furthermore,
we examined thedistribution
andpersist-ence
of antibody to
PGL-I
amongindividuals
in an area
in which
leprosy is endemic,
and nosignificantly
dif-ferent results were
found in seropositivity
rates using204 Hatta
MLPA
testor ELISA
method
durine
onevear
obser-vation of
the sameindividuals.lo
Recently, we conducted
anepidemiological
survey
in
South Sulawesi, Indonesia,
a well known
hyperen-demic
areaof leprosy, to estimate the rate of
M.
leprae
infection and
to
ascertain
the possible non
human sources ofbacilli.
The seropositive rates
of
antiPGL-I
antibody
in
the
general inhabitants
were
about35
Voand 47 % in males and females, respectively. I I' 12
Con-trol of
the disease
would
befacilitated
if it
were
pos-sible
to
detect
individuals
with
subclinical
diseasewithin
the next
years
becauseof the lack of
an
ap-propriate cell-mediated
response.Much
of the interest
in
the developmentof
serological
testsfor
leprosy
hasbeen
carried
out with two
objectives
in mind,
and,in
particular,
attempts have been made
to
evaluate
the usefulnessof school
children
survey compared tocom-munity
survey
in
the
same area.The present
study
is
to examine
IgM
anti
PGL-I from
school
children which is useful for
the determination
of
seroprevalence
andreflection
of
the magnitude
of
seroprevalence
among
apopulation
in
a
leprosy
en-demic
area arvillage
level.
METHODS
Population study.
In
1994,two
isolated
adjacentvil-lages
(Jenetaesaand Tukamasea)
in
a
rural
area
of
South Sulawesi, Indonesia, with 7729
and
3077
in-habitants
respectively,
were selected
for
the survey.
Persons who hadlived in
these villagesfor
at least the three months preceding andincluding
the studyperiod
were defined
as residents.Before
the study was under-taken, theindividuals
of the villages
were informedof
the purpose
of
the study,
and consent
were
obtained
from all
participants.
Three elementary
schools
in
Jenetaesa
with
87registered schoolchildren
of
gradeV
andfive
elemen-tary
schools
in
Tukamaseawith
65 registered
school-children of
gradeV
were included
in
the study.
As
it
'wasnot feasible to examine all registered persons, we
randomized to
collect
seraof both the
community
andschool children.
We
clinically
examined
1540 personsin
Jenetaesa and2357
persons
in
Tukamasea
during the
community
survey.
Serafor
MLPA
were collected
from
510
per-sons in Jenetaesa and 1496 persons in Tukamasea. Sera
were collected not of all
of
clinically
examined
per-sons,
but
only from
those who consented tothis study.
Sera
were collected
from
80
schoolchildren in
Jenetaesa andM
schoolchildren
in
Tukamaseafor
thedetection
of
antibody to
PGL- I
using
MLPA
test.Med J Indones
Clinical
examination was
carried out
by
experienced
leprosy workers
and diagnosis was^basedon the
clas-sification
of
Ridley and
Jopling."
Slit skin
smearswere taken
from
earlobes and a samplefrom
onelesion
at
least,
from
all
patients
for the
determination
of
bacterial index
(BI).
Blood
collection. Blood
samples
were collected
by
venapuncture
(
1.0ml i.v).
Sampleswere centrifuged
at 3000
rpm for 5
minutes
to
separatethe
serum and
transferred to 500pl
vials
(Sarsted, Assist Trading Co.,Ltd,
Japan)on
the
same day.All
serawere
stored
at-20o C
for futher
analysis.The
samplescollected from individuals were
coded,and
MLPA
test
was
performed
without
prior
knowledge
asto its the classification.
MLPA
test.
The
Serodia-leprae
microtitre particle
agglutination test
kit
for the detection
of Ig\4
anti
PGL-I antibody was
purchased
from Fujirebio
Inc.,
-6
J apan.
Serum samples were diluted to I : 1
6
and I :32in
96well
U
bottom microplates.
Twenty five
pl
of
unsensitized
gelatinparticle
and25pl
particle
sensitizedwith
trisac-charide
of PGL-I (NT-P-BSA)
were
mixed with
25pl
of
1:16 and25 ytl1:32 diluted
samples,respectively.
After
being incubatedfor
2 hours atroom temperature,
the plate was read for
agglutination using a mirror
reader. Serum samples showing agglutination at atitre
of 2
7:32 were
considered
positive.
When
sampleswere found
to
agglutinate
at
I:32, they were
thenserially
diluted
to
aconcentration
of
l:7024
for
quan-titative
tests.Data analysis.
All
data were recorded on special forms andanylized using
a database andstatistical software
package
(Epi-Info,
version
6)in
appropriatehardware.
Analysis
of
variance methods
were applied
as
indi-catedin
the
text.
All
probabilities
presented aretwo-tailed.
RESULTS
Sample
size andIncidence
rate.
At
the beginningof
the
survey
1729 peoplein
Jenetaesaand3077
people
in
Tukamasea
were
registered.
A
total
of
1540
in-habitants
(89.0
Voof
registered
population) in
a
-204 Hana
MLPA
test
or ELISA
method
durins
oneyear
obser-vation of
the sameindividuals.lo
Recently, we conducted
anepidemiological
survey
in
South Sulawesi, Indonesia,
a
well known
hyperen-demic
areaof leprosy,
to estimate the rateof
M.
Iepraeinfection and
to
ascertain
the
possible
non
human sources ofbacilli.
The seropositive rates
of
antiPGL-I
antibody
in
the
general inhabitants
were abott 35
Voand 47 %
in males
and females, respectively. 1 1' 12
Con-trol of
the disease
would
be
facilitated
if
it
were
pos-sible
to
detect
individuals
with
subclinical
diseasewithin
the
next
years
becauseof the lack of an
ap-propriate cell-mediated
response.Much of
the interestin
the developmentof
serological
testsfor
leprosy
hasbeen
carried
out with two
objectives
in mind,
and,in
particular,
attempts
have
been made
to
evaluate
theusefulness
of school
children
survey compared tocom-munity
survey
in
the
same area.The present
study is to examine
IgM
anti
PGL-I from
school
children which is useful for
the determination
of
seroprevalence and
reflection
of
the magnitude
of
seroprevalence
among
apopulation
in
a
leprosy
en-demic
area aIvillage
level.
MBTHODS
Population study. In
1994,two
isolated
adjacentvil-lages
(Jenetaesaand Tukamasea)
in
a
rural
areaof
South Sulawesi, Indonesia,
with
1729
and
3077
in-habitants
respectively,
were selected
for
the survey. Personswho had
lived in
these villagesfor
at least thethree months preceding and
including
the studyperiod
weredefined
as residents.Before
the study was under-taken, theindividuals
of the villages
were informedof
the purpose
of
the study,
and consent were obtained
from
all participants.
Three elementary
schools
in
Jenetaesa
with
87registered schoolchildren
of
gradeV
andfive
elemen-tary
schools
in
Tukamasea
with
65registered
school-children
of
gradeV
were included
in
the study.
As
it
was not feasible to examineall
registered persons, werandomized to
collect
seraof
both the
community
andschool children.
We
clinically
examined
1540 persons in Jenetaesa and2357
persons
in
Tukamasea
during the
community
survey.
Serafor
MLPA
were collected
from
510
per-sons in Jenetaesa and 1496 persons in Tukamasea. Sera
were collected
not of all
of
clinically
examined
per-sons,
but only
from
those who consented to this study.Sera
were collected
from
80
schoolchildren in
Jenetaesa and
44 schoolchildren
in
Tukamaseafor
thedetection
of
antibody to
PGL- I
using
MLPA
test.Med J Indones
Clinical
examination was carried
out by
experienced
leprosy workers
and diagnosis was^based onthe
clas-si{ioation
of Rrù\ey and
lop\ing."
S\it
skïn
smears were takenfrom
earlobes and a samplefrom
onelesion
at
least,
from
all
patients
for
the
determination
of
bacterial index
(BI).
Blood
collection. Blood
samples
were collected
by
venapuncture
(
1.0ml i.v).
Sampleswere centrifuged
at 3000
rpm for 5
minutes
to
separatethe
serum and
transferred to 500pl
vials
(Sarsted, Assist Trading Co.,Ltd,
Japan)on the
sameday.
All
serawere
stored at
-20o
C
for
futher
analysis.The
samplescollected from individuals were
coded,and
MLPA test
was
performed
without
prior
knowledge
asto its the classification.
MLPA test.
The
Serodia-leprae
microtitre
particle
agglutination test
kit
for the detection
of Ig\4
anti
PGL-I antibody was
purchased
from Fujirebio
Inc.,
Japan.6
Serum samples were diluted to I : 16 and
1:32in
96well
U
bottom microplates.
Twenty five
pl
of
unsensitized
gelatinparticle
and25pl
particle
sensitizedwith
trisac-charide of
PGL-I (NT-P-BSA)
were mixed
with
25pl
of 1:16 and251tl
l:32
diluted
samples,respectively.
After
being incubated
for
2 hours atroom temperature,
the plate was read for agglutination
using a mirror
reader. Serum samples showing agglutination at atitre
of >
l:32 were
considered
positive. When
sampleswere found
to
agglutinate
at
l:32,
they were
thenserially
diluted
to
aconcentration
of
I:1024
for
quan-titative
tests.Data analysis.
All
datawere recorded on special forms
and anylized using a database andstatistical software
package(Epi-Info,
version 6) in appropriate hardware.
Analysis
of
variance methods
were applied
as indi-catedin
the
text.
All
probabilities
presented aretwo-tailed.
RESULTS
Sample
size andIncidence
rate.
At
the beginningof
the
survey
1729 peoplein
Jenetaesaand3077
peoplein
Tukamasea
were
registered.
A
total
of
1540
in-habitants
(89.0
Vo ofregistered
population)
in
VoI 5, No 4, October - December 1996
There
wasno
statistically
difference
in
agegroup
and sex amongthe registered
andexamined population
in
the
two villages
(chi-
square testwith yate
correction,
p >
0.05).During
the survey 20 newleprosy
patientsin
Jenetaesaand29 new leprosy patients
in
Tukamasea werefound
and
8
treated patients
( 3 LL,
I BT
and
4
TT)
in
Jenetaesa
and2treated
patients
(2LL)
in
Tukamaseahad been
identified
years
before by the local
healthservice.
The type
of
leprosy
according
to Ridley
andJopling classification were
19tuberculoid
type(
1ZTT
and2BT, with BI=0)
and
I
lepromatous type
(
l
BL,
with
BI
=3)
in
Jenetaesa.Twenty
seven patients
in
Tukamasea were
classified
astuberculoid (
3BT
and24TT
with BI =0)
and2
aslepromarous (1
LL
and
1BL,
with
BI = 4
and
3,
respectively). Our
resultsshowed that
the
incidence rate
of
leprosy
in
the
sur-veyed
areaswere 12.9/I.000 population
in
Jenetaesa and 12.311.000population
in
Tukamasea.Schoolchildren survey.
In
the schoolchildren
survey 80from
87registered schoolchildren
in
gradeV
(91.9 Vo)inJenetaesa
(
Fig 3
)
and44 from
65
registeredschoolchildren
in
grade
V
(
67.8
Vo)
in
Tukamasea wereexamined (Fig.4).
There
wasno
statistically
difference
in
agegroup
and sex among the registered and examinedschoolchildren
in the two villages
(chi-square test
with yate
correc-tion,
p >0.05). No
clinical
signsof leprosy
werefound
from
schoolchildren
in
the
two
villages during
the survey.Distribution
of
IgM antiPGL-I
antibody
titer
in
schoolchild.".t
"trâ
community survey.
As
shownin
Table 1, using the
MLPA
test on
sera
from
80
ex-amined
schoolchildren
in
Jenetaesaturned out to
beNegative *) 32 64
t28
256 512 t024IgM Anti Phenolic Glycolipid
I
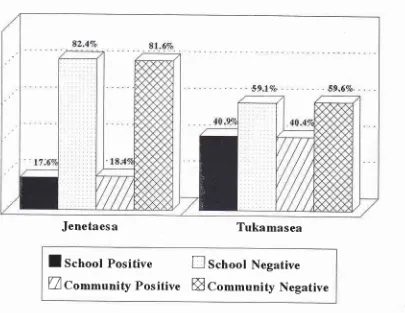
20517.6
Vopositive
and
82.4
Voweta
negative. Among
those
positive
MLPA
results, thetiters of
MLpA
were
32
(11.3
Vo) and 64(6.3 Vo).In
thecommuniry
survey
out of
510 examined persons
:
18.4
7owere
positive
and
81.6
Vowere negative. Among those positive
MLPA
results,
the titers
of MLpA
test were
32(l4.7%o),
64
(3.1 Vo),
128(0.2 Vo) and
256(0.4
Vo)respectively.
In
the
Tukamasea
schoolchildren survey
out
of
44examined
schoolchildren
:
40.9
Eowerc
positive
and59.1
Vowere negative.
Among
those
positive MLPA
results, the titers of
MLPA
were32
(Z9.5Eo),64(9.tVo)
and256 (2.3 Eo).In
thecommuniry survey out
of
1496examined persons
:
40.4 Vo werepositive
and 59.6 Vowere negative.
Among
those
positive
MLpA
results, thetiter of
MLPA
were 32
(21.9), 64 (15.7 Vo),
128(2.3 Vo),256 (0.2
Eo), 512(0.1
Eo) and 1024(O.l
Eo).Comparing
the seroprevalence between
the
school-children
survey
and the
community
survey.
Theseroprevalence
of
schoolchildren
in
Jenetaesa
wasfound
tobe
17 .6 Vo(
15out
of
80schoolchildren were
MLPA
positive). As
it
is notfeasible
tocollect
serafor
MLPA
test
from
all
examined population,
we
ran-domized to
collect
serain
thecommunity
survey. The
seroprevalence
of
the population
in
Jenetaesa
wasfoundtobe
18.4 Vo(94 outof 5l0persons wereMLpA
positive).
No significantly
difference
in
seroprevalence betweenthe schoolchildren survey
andthe
community
survey
(Fischer
exact test, p>0.01)
werefound.
alence
of
schoolchildren
a were found to be
signi
aesa
(Fischer
exact test, ptically
(Fig.5).
Tukamasea Village MLPA
Titer
Schoolchildren
Survey CommunitySurvey
26
l3
4 0I
0 059.
I
29.5 9.1 0.0 2.3 0.0 0.0 892 328 235 35 J 2I
59.6 21.9 15.7 2.3 0.2 0.1 0.1 Table I ' Distribution ofIgM-
PGL-I antibody titer using MLPA test in schoolchildren andcommunity survey
in
1994Jenetaesa Village
Schoolchildren
Vo
Community
VoSurvey
Suwey66 9 5 0 0 0 0
82.4
4t6
81.6I 1.3
75
14.76.3
16
3.10.0
I
0.20.0
2
0.40.0
0
0.00.0
0
0.0*)
[image:4.595.49.546.583.716.2]Èô
a 9l'
206 Hatta
The
seroprevalence
of
the schoolchildren survey in
Tukamasea
was
found
to
be 40.9
Vo(I8
out
of
44schoolchildren were
MLPA
positive),
while
in
theMed J Indones
community
surveyit
wasfound to
be40.4
Vo(604
our
of
1496 persons wereMLPA
positive).
>60
5 1.60
4 r-50
3l-40
2 l-J0 ro-zol
*
s00 400
.100200
100 0
100200 300 400
500Mnles
FcnralesZfixanrirrcrl
[-Jllcgisr"r".t
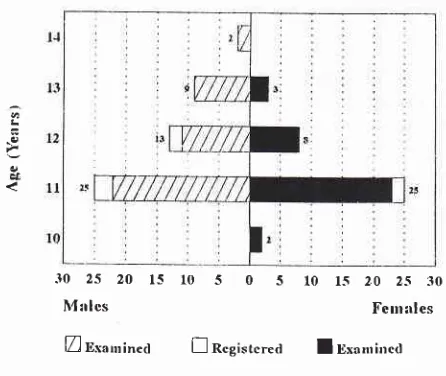
lUxanrirred [image:5.595.313.547.151.332.2] [image:5.595.51.284.154.331.2] [image:5.595.55.278.461.649.2] [image:5.595.327.549.464.652.2]Difference in sex group among registered population and examined population is not significant (chi square test, p > 0.05)
Figure 2. Distribution ofregistered and examined population according to age and sex in Tuknmasea village, 1994
2.s 20 l.s l0 .5 0
.s l0
l-s
20 I\4:rlcs
li'c nr a I csZ [xanrirr..r'l
['.lRcgistcr"a I
DxanrirrcdDifference in sex group among registered population and examined schoolchildren is not significant (chi square test, p > 0.05)
Figure 4. Distribution ofregistered and examined schoolchildren according to age and sex
in
Tukamaseavillage, 1994>60
5t-60
4 l-50 3 I -,10
2l-30
l0
250 200
l-{0 100 s0 0 50
100 l-50200
250Malcs
fcnralesZlExanrirretl nRegistered
ElExanrinedDifference in sex group among registered population and examined
population is not significant (chi square test, p > 0.05)
Figure
I.
Distiburton of registered and examined populaionaccording to age and sex in Jenetaesa village, 1994
.10
25 20 l-r 10 5 0 5 l0 15 20
2-5 30I\'l:rlcs
FernalesZ Iisaurined ! Rcgistcreil I
BxanrinedDifference in sex group among registered population and examined schoolchilren is not significant (chi square test, p > 0.05)
Figure 3.
Distibution
of registered and emmined schoolchildren according to age and sex in Jenetaesa village, 1994L
e&
l'r
t2
-g
;u
c&Vol 5, No 4, October - December 1996 IgM Anti Phenolic Glycolipid
I
Jenetaesa
Tukamasea
I
School
Positive
E
School Negative
[image:6.595.109.514.79.392.2]Uco^^unity
Positive ffi
Co--unity
Negative
Figure 5. Seroprevalence of schoolchildren survqt and community survey in Jenetaesa and Tukamasea village, 1994
DISCUSSION
The pattern
of leprosy transmission
among thepopula-tion is currently
unclear. Evidence
suggeststhat most
of
thenew
casesof
leprosy
found
arenot
dueto
closecontact
with
leprosy patients. However,
it
wasproved
that the
chanceof
developing
this
diseaseis far
morebigger
in
the
households where patients
with
multi-bacillary (MB)
leprosy
is present.We
haveincreasing
evidence
to
show that a
considerable number
of
in-habitants have been
infected
with
leprosy.s
Most of
them have
no
history
of
being
subjected
to
direct
contact
with
leprosy patients, suggesting
that the
sourceof infection of
leprosy
bacilli
is
not limited
to untreatedleprosy
patients.Using
polymerase chainreaction
(PCR) todetectDNA
M.
leprae from
nasal swab
specimens, demonstratedthat
about 8.0 7oof
the generalinhabitants
in
endemicvillages
in
SouthSulawesi, Indonesia, cany
M.
leprae
on the surfaceof their
nasal mucosa.a Theseepidemio-Iogical
observation
suggest thepossibility
that rather
strong
infectivity
of
leprosy
bacilli
and
widely
dis-tribution of
M.
leprae
in
the environment
of
the
en-demic areasplay an important
role in thecontinual high
incidence
of
leprosy
in
an area.Several
serological
tests have been developedover
thepast years
to
detect
leprosy
infection.14
The
results,however,
arestill
not satisfying.
Currently,
interest
in
serodiagnosis has been
revived by
the
invention
of
aserological test based
on a
supp_osedlyM.
Ieprae
specific antigenic
determinants.r)'to
IgM
anti PGL-I
antibodies,
specifically
directed
against
tope, have
been
demon-strated
i
pâtients.lT
aswell
asits
7
208 Hatta
Furthermore,
aseroepidemiological
study ofM. Iepraeinfection
using
MLPA
and ELISA to detectIgM
anti
PGL-I antibodies
in inhabitants
of
aleprosy
endemicvillage
in South Sulawesi, Indonesia has also
beenreported.ll
Th"
validity
of
this
suggestion,
unfor-tunately,
has never been testedin schoolchildren which
may be representative
in a population
for
the
deter-mination
of the magnitudeof seroprevalence in leprosy
endemic
areas.In this study, to determine the magnitude
of infection
among a population, we examined schoolchildren
in
two villages, which
differ
in seroprevalence and we
compared thefindings by examining
the populationin
the
sameleprosy endemic village.
We propose
to validate this
approachof
assessmentof
the leprosy problem through extrapolation
of
sero-positivity
ratesin
schoolchildren
in other
areas, bothin Indonesia
and beyond.Although,
the seropositivity
rates in children is repre-sentativeof seropositivity rates in populations,
further
information
is
needed
to determine
the
sources
of
transmission
in human.
The detection
of
DNA
M.
leprae by PCR from nasal swabs specimens
in
school-children and populations is still in progress.
Acknowledgements
The author
would like to thank
Drs. Paul
R. Kiatser,
Stella van Beers and Shinzo Izumi for critical
reading
of the manuscript.
The author
would
also like to express
his gratitute to
the Head
of
the Regional Office
of
the
Ministry of
Health, Republic of Indonesia
in
South Sulawesi
andthe Leprosy officer
of
the
Ministry of
Health
in
theprovince of South Sulawesi
for their cooperation. He
is indebted to all peoplein the villages who voluntarily
cooperatedin this study.
The
financial
support
of The Netherlands Leprosy
Relief Association
(NSL)
and PfeizerHealth
ResearchFoundation
of Japan is greatly
appreciated.Also,
thanks
to Dr.
Takafumi
Hayashi, Director
General of Toyama
YUAI
Hospital,
for
his financial
supportthrough
the Japan IndonesiaMedical
Associa-rion of
YUAI
Hospital (JIMA).
REFERENCES
l. Noorden
SK, Lopez BravoL,
SundaresanTK.
Estimatednumber of leprosy cases in the world. WHO
Bull
1992;70:707-lo.
Med J Indones
2. Hartskeerl RA, De Wit MYL, Klatser PR. Polymerase chain reaction
for
the detectionof M.
Ieprae. J Gen Microbiol 1989; 135:2357-64.3. Hatta M. Application of polymerase chain reaction for
detec-tionof Mycobacterium leprae DNA in nasal swab specimens from untreated leprosy patients. Proceed. 2nd Asian Pacific Conference on Medical Genetics and Eijkman Symposium on the Molecular Biol Dis. 1995; Iakarta:. 127 .
4.Hatta
M,
van
BeersSM,
MadjidB, Achmad D, deWit
MYL, Klatser PR. Distribution and persistence of Mycobac-terium leprae nasal carriage among a population in which leprosy is endemic in Indonesia. Trans R Soc Trop Med Hyg1995; 89: 381-5.
5. Izumi
S,
SugiyamaK,
FujiwaraT, Hunter SW, Brennan
PJ. Isolation of Mycobacterium leprae specific glycolipidantigen, phenolic glycolipid-I from formalin fixed human lepromatous liver. J Clin Microbiol 1985;22: 680-2. 6. Izumi S, Fujiwara T, Ikeda M, Nishimura
Y,
Sugiyama K,Kawat
su K. Novel gelatin particle agglutination test forserodiagnosis of leprosy in the field. J Clin Microbiol 1990;
28:525-9.
7. FinePEM. Problems in the collection and analysis
of
data in leprosy study. Lep Revl98l;
52:197-206.8. Hatta M, Izumi S, Klatser PR. Evaluation
of
the Mycobac-terium leprae particle agglutination (MLPA) test as tool in the epidemiology of leprosyin
high
prevalence village in South Sulawesi, Indonesia. Southeast Asian J Trop Med Pub Health 1995; 26: 631-5.9. Godal T, Negassi S. Subclinical infection in leprosy. Br Med
I
1973; 3: 557 -9.10. Hatta M, Izumi S, Kawatsu K, van Beers SM, Klatser PR.
Distribution
and persistenceof
antibody to
phenolicglycolipid-I among individuals in an area in which leprosy is endemic. Am J Trop Med Hyg 1996; submitted for publi-cation.
ll.
Izumi
S,
Hatta M, Kawatsu K, Matsuoka M. Sero-epidemiological study of M. Ieprae infection in inhabitants of leprosy endemic village in South Sulawesi, Indonesia. IntJ Leprosy 1995; 63: 650
12. lzumi S, Hatta M, Matsuoka M, Kawatsu
K.
Identificationof
leprosy infection using PGL-I antibodyin
population which leprosy endemic area, Indonesia (in Japanese). Jap J Leprosy 1996; 65: 50.13. Ridley DS, Jopling WH. Classification of leprosy according
to immunity :
a five-group system.Int
JLepr
1966; 34: 255-73.14. Melsom
R.
Serodiagnosis of leprosy : the past, the present,and
some prospectfor
the future.Int J Lepr
1983;5l:
235-52.
t5. Brett SJ, Drapper P, Payne SN, Rees RJW. Serological activity of a characteristic phenolic glycolipid from
Myco-bacterium leprae
ln
sera from patients with leprosy and tuberculosis. Clin Exp Immunol 1983; 52: 27 I -9.16. KlatserPR,
deWitMYL, KolkAH.
An EllSA-inhibition
test using monoclonal antibody for serology ofleprosy. Clin
Exp
Immunol 1985; 62: 468-73.Vol 5, No 4, October - December 1996
18.
Levis
WR, Meeker HC,
Schuller-LevisG,
Sersen E, Schwerer B. IgM and IgG antibodies to phenolic glycolipidlfrom
Mycobacterium Leprae tnleprosy; insight into patient monitoring, erythema nodosum leprosum, and bacillary per-sistence. J Invest Dermatol 1986; 86: 529-34.IgM Anti Phenolic Glycolipid
I
20919. Schewerer
B,
Meeker HC, SersenE,
LevisWR.
Ig
M
antibodies against phenolic glycolipid
I
from Mycobac-terium lepraein
leprosy sera: relationshipto
bacterialindex
and erythema nodosum leprosum.Acta
Leprol