Regular Article
Prothrombotic factors and the risk of acute onset non-cardioembolic stroke in young
Asian Indians
Arijit Biswas
a, Ravi Ranjan
a, Arvind Meena
a, Suhail Akhter
a, Vinita Sharma
a, Birendra Kumar Yadav
a,
Madhuri Behari
b, Renu Saxena
a,⁎
aDepartment of Hematology bDepartment of Neurology
a b s t r a c t
a r t i c l e
i n f o
Article history:
Received 29 September 2008
Received in revised form 25 February 2009 Accepted 25 February 2009
Available online 27 June 2009
Keywords:
Factor V Leiden mutation Factor V HR2 Haplotype Coagulation Inhibitors Factor VIII levels Acute phase Asian-Indians
Introduction:Several prothrombotic factors–both hereditary and acquired–are known to cause stroke. Commonly investigated causes are activated protein C resistance, factor V Leiden mutation, factor VIII levels, prothrombin 20210 G-to-A mutation, coagulation inhibitors such as proteins C and S, and antiphospholipid antibodies such asβ2-glycoprotein.
Objective:The literature on the prevalence of hematological defects pertaining to these variables in the Asian Indian stroke population is limited to a few isolated reports. In the current study we investigate the above-mentioned variables in 120 stroke patients (non-cardioembolic acute-onset stroke) and compare their status with the hematological profile of an equal number of healthy age- and sex-matched controls.
Material and Methods: Plasma and blood leukocytes were collected from all patients and controls for performing hematological assays and molecular tests respectively. The mutations were detected using standard polymerase chain reaction/restriction fragment length polymorphism (PCR/RFLP) procedures. Statistical analysis was done using SPSS version 12.0.
Results:Factor V Leiden (prevalence 8.3% in patients) and activated protein C resistance (prevalence 19.6% in patients) both showed a high degree of association (Pb0.01) with the disease condition. However, contrary to common expectations, factor V Leiden was observed much less frequently in patients showing activated protein C resistance (10 out of 23; 43.4%) than is commonly observed in the Caucasian population (almost 90%). Post-acute-phase factor VIII levels were also found to be significantly associated with stroke: 125.6 + 21.1% number of profitable positions (NPP) for controls and 136.2 + 28.8% NPP for patients (P= 0.001).
Conclusion:factor V mutations, such as factor V Leiden, may be important risk factors for stroke in an Asian Indian population. Activated protein C resistance has a stronger association with stroke than factor V Leiden and may be caused by other factors such as elevated factor VIII levels in the Asian Indian population apart from factor V Leiden itself.
© 2009 Elsevier Ltd. All rights reserved.
Introduction
Prothrombotic risk factors often work together to give rise to thrombosis, which in turn may lead to stroke. These risk factors may be inherited, like the factor V Leiden mutation, or acquired –e.g. resistance to activated protein C (APCr) or antiphospholipid anti-bodies–in origin. The detection of these defects could lead to relevant modifications in clinical treatment and patient management. APCr is one of the defects of the hemostatic system which has been commonly
observed in stroke conditions. A meta-analysis has shown that the prevalence of APCr can vary from 0 to 38% in stroke conditions[1]. A majority of APCr-positive Caucasian patients (more than 95%) carry the factor V Leiden mutation. This mutation is an Arg506Gln change, which decreases the susceptibility of factor Va to inactivation by activated protein C[2,3]and impairs the ability of factor V to stimulate the inactivation of factor VIIIa mediated by activated protein-C[4,5]. However, these studies are primarily limited to the Caucasian population. APCr can also be seen in the absence of factor V Leiden
[6]. It is now a well-documented fact that factor V Leiden prevalence rates vary from population to population.
The other factor V mutations which are commonly screened, some of which have also been known to contribute towards APCr, are factor V Hong Kong/Cambridge and factor V HR2 haplotype. Factor V Hong Kong/Cambridge are two mutations occurring at the Arg306 activated protein C cleavage site of factor V. Thefirst mutation is a G-to-C
⁎Corresponding author. Department of Hematology, I.R.C.H. Building (1stfloor), All India Institute of Medical Sciences, Ansari Nagar, New Delhi–110 029, India. Tel.: +91 011 26593642; fax: +91 011 26588663.
E-mail address:[email protected](R. Saxena).
0049-3848/$–see front matter © 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2009.02.015
Contents lists available atScienceDirect
Thrombosis Research
transversion at nucleotide position 1091 resulting in an Arg306Thr replacement; this mutation is known as the factor V Cambridge mutation[7]. The second mutation (called the factor V Hong Kong mutation) is caused by an A-to-G transition at nucleotide position 1090 resulting in an Arg306Gly replacement[8]. The third genetic variant is the factor V HR2 haplotype, also referred to as A4070G mutation, and is another genetic cause for mild APCr[9]. The A4070G mutation is present in exon 13 of human clotting factor V gene (A4070G; His1299Arg; mutant genotype named R2R2)[10–12]. It is found to be in tight association with more than 12 polymorphisms of the factor V gene, the combination collectively known as the HR2 haplotype. Factor V mutation studies on the Asian Indian population are slightly under-represented, especially in stroke conditions. Most of them originate from US or European studies where the investigator has dealt with small groups of Asian Indians residing in the places where the studies were conducted. It is therefore likely that frequent
mixing with the local population might have given a diluted result in these studies and may not have been truly representative of the genetic character of the Asian Indian population.
More recently, factor VIII levels in prothrombotic conditions have been under investigation. Factor VIII has unique characteristics as a risk factor. It is well established as an acute-phase reactant[13], and therefore one could argue that high levels of factor VIII following a thrombotic event may be more a result of the acute phase rather than the cause of the event. However, there have been reports which do establish it to be predictive for thrombosis and not just the result of an acute-phase event[14]. The dichotomy therefore still remains. While most of these studies have looked at venous thrombosis[14,15], stroke (which can have both arterial and venous origins) has been less thoroughly investigated in this regard, especially when it comes to investigations conducted after the acute phase. Abnormalities in natural anticoagulants such as protein C and protein S, and elevated
Table 1
Primer and polymerase chain reaction (PCR) details for prothrombotic mutations.
Polymorphism/mutation Primer sequence (5′→3′) Tm (°C)
Restriciton enzyme PCR product size before digest
PCR product size after digest
Factor V Leiden or 1691 G→A or 506 Arg→Gly (= rs6025)
F: CATGAGAGAACATCGCCTCTG 58 MnlI 147 bp Normal: 85, 37, 25 bp
R: GACCTAACATGTTCTAGCCAGAAG Heterozygous: 122, 85, 37,25 bp
Mutant: 122, 25 bp Factor V HR2 haplotype
or 4070 A→G
F: CAAGTCCTTCCCCACAGATATA 58 RsaI 703 bp Normal (R1R1): 703 bp
R: AGATCTGCAAAGAGGGGCAT Heterozygous (R1R2): 703, 492, 211 bp
Mutant (R2R2): 492, 211 bp Factor V Hong Kong/Cambridge or
306 Arg→Gly/ 306 Arg→Thr
F:TCCCACCTCTTCATGTGCCGCCTCTG 56 For Cambridge:MvaI 252 bp For Cambridge: Normal: 173, 53 bp R:CCAAACTAAAATGTTCAAAAATTGCCTGGGCATTA For Hong Kong: HpaII Heterozygous: 226, 173, 53 bp
Mutant: 226 bp
For Hong Kong: Normal: 252 bp Heterozygous: 252,198, 54 bp Mutant: 198, 54 bp Prothrombin mutation
or 20210 GNA
F: TCTAGAAACAGTTGCCTGGC 58 HindIII 345 Normal GG: 345 bp
R: ATAGCACTGGGAGCATTGAAGC Heterozygous GA: 345, 322 and 23 bp
Mutant AA: 322 and 23 bp
F, forward primer; R, reverse primer; bp, base pair.
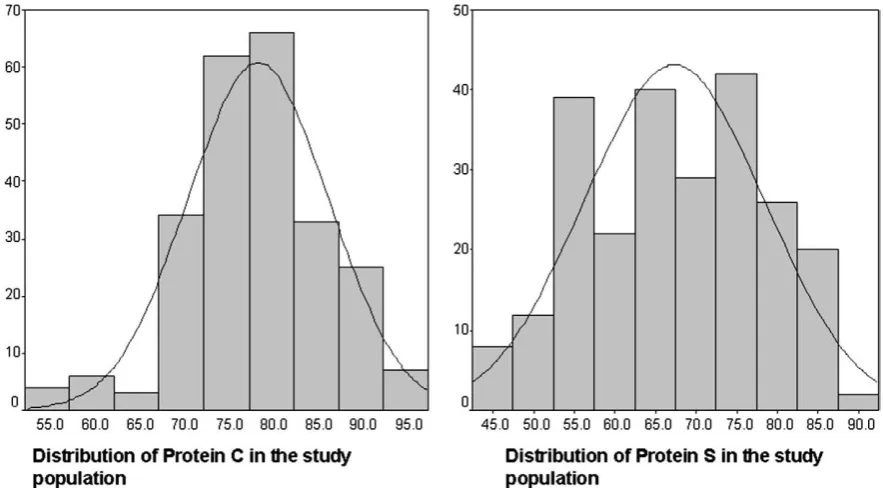
Fig. 1.A histogram showing the distribution of Protein C and S in Patients and Controls.
levels of antiphospholipid antibodies, have also been shown to be associated with ischemic stroke.
In the present study we look at the impact of the mutants of factor V (factor V Leiden, factor V Hong Kong/Cambridge and HR2 haplotype) and prothrombin gene (factor II G20210A mutation) on the Asian Indian stroke population. Our prevalence study has been done against the background of other hematological assays such as the levels of natural anticoagulants (proteins C and S), factor VIII, andβ2-glycoprotein IgG
levels in order to obtain a more comprehensive picture. This kind of study is limited in the Asian Indian population, which has a very diverse genetic background which is different from that of Caucasian and other Asian populations (i.e. oriental populations), and should give a fair idea to clinicians and future investigators as to the hematological status of Asian Indian stroke patients.
Material and Methods
Place of study
Patient collection was done from the Outpatient Departments and Wards of the Departments of Neurosciences and Hematology at the All India Institute of Medical Sciences. Control sample collection was done from Hospital staffers and their relatives or from unrelated attendants of the patients.
Ethical Clearance
The local ethics committee of All India Institute of Medical Sciences approved this study, and written informed consent for the study was obtained.
Sample size
Patients matching the requisite inclusion and exclusion criteria were asked to report for a 3–6-month follow-up. Only patients who
reported for at least a single follow-up were chosen as the subjects for the study. Initially 231 patients matching the inclusion and exclusion criteria reported for the study. However, only 120 patients returned for a follow-up, and these were the subjects of study. The remaining 111 patients were either lost to follow-up or refused consent during the study period. For controls, 120 age- and sex-matched healthy subjects were collected from hospital staff members or attendants of patients not related to them.
Patients
Inclusion Criteria
All patients below 40 years of age presenting with a diagnosis of acute-onset stroke (cerebrovascular event) and showing evidence of ischemic infarct were included in the study. The diagnosis of stroke was confirmed by a combination of objective imaging methods such as computed tomography/magnetic resonance imaging (CT/MRI) brain/ Doppler studies. Patients with stroke of non-cardioembolic origin were included in the study. Patients who presented within 4 weeks of onset of illness were included in the study. Only patients of northern Indian origin (Jammu and Kashmir, Uttar Pradesh, Haryana, Himachal Pradesh, Bihar, West Bengal) were included in the study.
Exclusion Criteria
Patients with cardioembolic strokes or having past history of cardiovascular disease were excluded from the study. Patients on oral anticoagulants during thefirst sample collection were excluded from the study. Patients suffering from diabetes mellitus, hyperlipoprotei-nemias, cancer, sickle-cell anemia, and liver disease were excluded from the study.
Controls
Inclusion Criteria
Apparently healthy men and women were selected as controls. All controls were of northern Indian origin.
Exclusion Criteria
Controls taking any form of medication or having had surgery or suffered trauma in the past 30 days were excluded from the study. Controls with a history of bleeding, thrombotic, or cardiac disorders were also excluded from the study, as were pregnant women.
Method
Fasting blood samples were collected in siliconized glass contain-ers containing 1 part sodium citrate solution (0.11 mol/l) with 9 parts venous blood; care was taken to avoid foam formation during collection. Platelet-poor plasma was prepared from citrated blood by
Table 2
Comparative protein C and protein S levels in patients and controls.
Patients Number of subjects with deficiency
(as per the kit definition i.e.b65%)
8 0 0.003
Protein S
Median levels in % (range) 67 (43–89) 67.5 (51–89) 0.578 Number of subjects with deficiency
(as per the kit definition i.e.b50%)
10 0 b0.001
*Pvalues were determined using the Mann–Whitney test for comparison of median levels of proteins C and S, and Chi-square for number of subjects in patient and control groups showing protein C and S deficiency.
Table 3
Genotype and resistance to activated protein C (APCr) details of patients and controls.
Controls (%) Patients (%) Chi-square,Pvalue* OR (range)
Total number 120 120 –
Factor V Leiden 1 (0.8) 10 (8.3) 7.72, 0.005 10.8 (1.3–229.5)
Factor V Leiden homozygous mutant form 0 (0) 4 (3.3) 0.121
Factor V Leiden heterozygous form 1 (0.8) 6 (8.3) 0.059
Factor V HR2 haplotype 16 (13.3) 18 (17.5) 0.034, 0.853 1.14 (0.61–2.01)
Factor V HR2 haplotype mutant form (R2R2) 0 (0) 2 (1.2) 0.248
Factor V HR2 haplotype heterozygous form (R1R2) 16 (13.3) 16 (13.3) 1.00
Factor V Hong Kong/Cambridge 0 (0) 0 (0) –
APCr 1 (0.83) 23 (20) 22.47,b0.001 28.21 (3.74–212.7)
centrifugation at 1500g for 10 min. The supernatant plasma was frozen rapidly in a well closed plastic container, at–70 °C. Genomic DNA was extracted from peripheral-blood leukocytes. Thrombin-activatablefibrinolysis inhibitor (TAFI) antigen assay was performed using the TAFI antigen assay kit (STAGO diagnostica). Total homo-cysteine concentration was evaluated using enzyme immunoassay (EIA) (Axis shield kit). Normal levels for homocysteine were 5– 16μmol/L (as per kit instructions). Fibrinogen levels were measured using the Clauss method (Kit from STAGO Diagnostica). Normal levels forfibrinogen were 200–450 mg/dl (as per kit instructions). Protein C and S antigen levels were measured using enzyme-linked immuno-sorbent assay (ELISA; DADE Behring kit). Activated protein C resistance assays were performed using kits from STAGO diagnostica. Normal levels for proteins C and S were 65–140% and 70–130% respectively (as per kit instructions). Factor V Leiden, factor V Hong
Kong/Cambridge, prothrombin 20210 G→A and HR2 haplotype were
detected using a PCR/RFLP procedure using the primer and restriction enzymes listed in theTable 1.
Statistical Analysis
Descriptive and frequency statistical analyses were obtained, and comparisons were performed by use of the SPSS statistical package, version 12.0. A difference of Pb0.05 was considered statistically significant. A non-parametric Mann–Whitney test was used for comparison of variables which were skewed. Variables which were normally distributed were compared using the Student t-test.
Result
Coagulation Inhibitors
Since the distribution of proteins C and S in the entire study population was negatively skewed (Fig. 1), the median levels in patients and controls were compared using the Mann–Whitney test. No significant difference was observed in the median levels of proteins C and S (Table 2) between the patient and control populations. No difference in median levels was seen between arterial (origin) and venous (origin) strokes (P=0.3556 and 0.665 for proteins C and S respectively) or between recurrent and non-recurrent strokes (P= 0.770 and 0.502 for proteins C and S respectively). No difference in median levels of proteins C and S was observed between males and females (P=0.389 and 0.647 respectively). When the cut-offs (protein Cb65% and protein Sb50%) defined by the kit were used as reference, eight (6.6%) and ten (8.3%) patients were seen to be carrying proteins C and S deficiency respectively (Table 2). Four of these patients carried combined protein C and S deficiency; however, this may be explained by the fact that all these four were on anticoagulants when their sample was taken (since both protein C and protein S were evaluated after the acute phase of stroke, i.e., when the second sample was taken). Therefore effectively only four (3.3%) and six patients (3.3% and 5% respectively) carried protein C and protein S deficiency for non-acquired reasons. None of the controls were carrying either protein C or protein S deficiency.
Fig. 2.Illustration depicting the observed relationship between Activated Protein C resistance and Factor V mutations in Patients. The shaded region represents Activated Protein C resistance. The number of subjects in individual groups can be calculated by counting the respective bars.
Table 4
Resistance to activated protein C (APCr) results for patients in the presence and absence of factor V Leiden and HR2 haplotype.
S. No. Genotype APCr Non-APCr Total
1 Patients carrying only factor V Leiden homozygous mutant form
4 0 4
2 Patients carrying only factor V HR2 haplotype mutant form (R2R2)
2 0 2
3 Patients carrying only factor V Leiden heterozygous form
3 0 3
4 Patients carrying only factor V HR2 haplotype heterozygous form (R1R2)
10 3 13
5 Patients carrying both factor V Leiden homozygous mutant and HR2 haplotype homozygous mutant forms(R2R2)
0 0 0
6 Patients carrying both factor V Leiden heterozygous and HR2 haplotype homozygous mutant forms (R2R2)
0 0 0
7 Patients carrying both factor V Leiden homozygous mutant and HR2 haplotype heterozygous form (R1R2)
0 0 0
8 Patients carrying the factor V Leiden heterozygous form and HR2 haplotype heterozygous form (R1R2)
3 0 3
9 Patients carrying neither factor V Leiden nor HR2 haplotype mutant or heterozygous forms
1 94 95
10 Total number of patients 23 97 120
Activated Protein C resistance
APCr was seen in 23 out of 120 of patients (19.16%) (Table 3). Of these, 43.4% (10 out of 23) were seen to carry factor V Leiden mutation (Table 4; see alsoFig. 2for a better understanding of the relationship between APCr and factor V mutations in this study). Eighteen out of 23 (78.2%) were seen to carry factor V HR2 haplotype. Three patients showed both factor V Leiden and factor V HR2 haplotype. All patients positive for factor V Leiden were APCr-positive. Three patients positive for HR2 haplotype (all heterozygous) did not show APCr. In the patient's positive for APCr and factor V HR2 (n = 12), but not carrying factor V Leiden, elevated factor VIII, β2-glycoprotein IgG and
homocysteine levels were seen in three, three and three patients respectively. Only one sample showing APCr was not positive for either factor V Leiden or factor V HR2 haplotype. Sixteen control samples (13.3%) showed factor V HR2 haplotype (although only in heterozygous form) APCr, but only one control sample was found to be carrying factor V Leiden (in heterozygous state).
Factor V and other prothrombotic mutations
Factor V Leiden mutation was seen in 8.3% (10 out of 120) of patients and 0.83% (1 out of 120) of controls. Factor V Leiden mutation was seen to be strongly associated with the disease phenotype (P=0.005). Carriers of the factor V Leiden mutation were ~10 times more likely to develop stroke (Table 3). Factor V HR2 haplotype on the other hand was not independently associated with stroke (P=0.371) (Table 3). Factor V HR2 haplotype was seen in 17.5% (21 out of 120) of patients and 13.3% (16 out of 120) of controls. None of the patients or controls carried the factor V Hong Kong or Cambridge mutations. None of the patient or controls carried the prothrombin 20210 G→A mutation either.
Factor VIII levels
The distribution of factor VIII levels in the control population was seen to be normal (Kolmogorov–Smirnov test,P= 0.283). Post-acute-phase mean factor VIII levels (125.6 + 21.1% NPP for controls and 136.2 + 28.8% NPP for patients) were significantly raised in patients compared with controls (P= 0.001;Fig. 3). When the numbers of patients and controls–eight (6.6%) and two (1.6%) respectively–with high factor VIII levels (i.e. 177% orN95th percentile of the studied population) in our study were compared, the difference was only
modestly significant (Fisher exact test,P= 0.041). There isn't much of a change in risk in thefirst three quartiles of factor VIII levels, nor is there a definitive increasing or decreasing trend; however, there is an awkward jump in odds ratio (OR) to 4.05 as we enter the fourth and last quartile of the factor VIII level (Fig. 4).
Antiphospholipid antibodies
A significantly higher number of patients–nine of 120 patients (7.5%)–were seen to have raised levels of IgG (i.e. N15 U/ml, kit instructions, which incidentally was also the 90th percentile of the studied population) compared with controls (one in 120, 0.83%;
P= 0.009). Median IgG levels in patients were also significantly raised compared with those in controls (median levels: patients 8.2 U/ml, range 2.2–21.2; controls 7 U/ml, range: 2–18;Pb0.001).
Discussion and Conclusions
Our study showed only 3.3 and 5% (after accounting for the number of patients on anticoagulants when the second sample was taken) of the patient population to be carrying type-I protein C and S deficiency respectively. This, coupled with the fact that antigenic levels of proteins C and S did not vary significantly in our stroke population (from the healthy control population;PN0.05), led us to conclude that inherited type-I protein C and S deficiencies per se may not be independent risk factors for stroke in our study population. APCr, on the other hand, showed a strong association with stroke in our population (Pb0.001). However, unlike the Caucasian population, in which almost 90% of patients positive for APCr carry the factor V Leiden mutation, only 43.4% of the patients in our study population who were positive for APCr carried the factor V Leiden mutation (Table 4,Fig. 2). Rather the factor V HR2 haplotype was seen at higher frequency (78.2%) in patients showing APCr. Earlier, our group had reported somewhat similar results in patients with deep vein thrombosis[16]. However, there were three patients as well as all controls (except one) who carried factor V HR2 haplotype (and not factor V Leiden mutation) but did not show APCr, indicating that the mere presence of factor V HR2 haplotype alone may not cause APCr. It would require the simultaneous presence of other defects in the background. Earlier reports have shown raised homocysteine and factor VIII levels as well asβ2-glycoprotein to contribute to activated
protein C resistance[17,18]. Also the fact that factor V HR2 haplotype is
Fig. 4.Rise and Odds Ratio in the 4hQuartile of Factor VIII levels. Q refers to Quartile.
not independently associated with stroke in our study is supported by previous similar reports from the Caucasian population[19]. Therefore one of the importantfinding of our study was that APCr (with or without factor V Leiden mutation) might be an important risk factor for stroke in our population.
Post-acute-phase mean factor VIII levels were significantly raised in patients compared with controls (P= 0.001) in our study. This was also true for the number of patients and controls–12 (10%) and 4 (3.3%) respectively–with high factor VIII (N177%), although theP
value was only modestly significant (P= 0.041). BorderlinePvalues do indicate that a bigger population size might reflect a different result. One recent study conducted on pediatric stroke showed no difference in levels of factor VIII post acute phase[20]. The ARIC Study had earlier shown that, per SD increase in factor VIII and in von Willebrand factor (vWF), the risk for stroke increased 1.34-fold (95% CI 1.2–1.5) and 1.36-fold (95% CI 1.2–1.5), respectively[21]. In our study there isn't much of a change in risk in thefirst three quartiles of factor VIII levels, nor is there a definitive increasing or decreasing trend; however, there is an awkward jump in OR to 4.05 as we enter the fourth and last quartile of the factor VIII level (Fig. 4.). This trend may be explained by the fact that there is a great deal of heterogeneity in factor VIII levels in the general population, and a significant difference in patients and controls is observed only in the topmost quartile of the factor VIII level. The presence of high factor VIII levels post acute phase is also an interestingfinding, as this has previously been reported in deep vein thrombosis patients also [22]. Earlier studies have shown that high factor VIII levels may prevent cleavage of factor V by protein C, thereby creating conditions of activated protein C resistance[23]or may even lead to exaggerated levels of thrombin. Therefore, from the preliminary results, we conclude that factor VIII would be a worthwhile variable to investigate in a typically Asian Indian prothrombotic condition.
Limitations
Despite some interesting results, our study does have serious limitations. One of the major limitations of this entire exercise is that, in spite of selecting patients of north Indian origin, we might not have selected a genetically homogenous population. India is a huge country, and even within the same geographical location the marriage patterns of different ethnic groups is a complicated affair which gives rise to incredible genetic diversity. Future investigators may look to identify population subgroups (using genetic, phenotypic, behavorial or lifestyle markers) for such studies. Also a larger population size may be more informative as to the exact role of some of the mutations studied. Apart from providing more informative genetic content, a larger population size would also be helpful in statistically analyzing clinical subgroups (with respect to symptoms or the presence or absence of other covariates such as smoking, hypertension etc) which we felt could not be adequately adjusted for while performing the statistical analyses owing to the smaller sample size of the study. Such adjustments and more might give better information on the gene– environment interaction, and may also help in establishing important clinical correlations. All in all, future studies might consider a large cross-sectional multicentric study that is more detailed in the clinical aspects.
Conflict of interest statement
No conflict of interest declared.
References
[1] Bushnell CD, Goldstein LB. Diagnostic testing for coagulopathies in patients with ischemic stroke. Stroke 2000;31:3067–78.
[2] Kalafatis M, Bertina RM, Rand MD, Mann KG. Characterization of the molecular defect in factor VR506Q. J Biol Chem 1995;270:4053–7.
[3] Nicolaes GA, Tans G, Thomassen MC, Hemker HC, Pabinger I, Varadi K, Schwarz HP, et al. Peptide bond cleavages and loss of functional activity during inactivation of factor Va and factorVaR506Q by activated protein C. J Biol Chem 1995;270:21158–66. [4] Varadi K, Rosing J, Tans G, Pabinger I, Keil B, Schwarz HP. Factor V enhances the cofactor function of protein S in the APC-mediated inactivation of factor VIII: influence of the factor VR506Q mutation. Thromb Haemost 1996;76:208–14. [5] Thorelli E, Kaufman RJ, Dahlback B. Cleavage of Factor V at Arg 506 by activated
protein C and the expression of anticoagulant activity of factor V. Blood 1999;93: 2552–8.
[6] Rosendaal FR, Koster T, Vandenbroucke JP, Reitsma PH. High risk of thrombosis in patients homozygous for factor V Leiden (activated protein C resistance). Blood 1995;85:1504–8.
[7] Williamson D, Brown K, Luddington R, Baglin C. Factor V Cambridge. A new mutation (Arg306 to Thr) associated with resistance to activated protein C. Blood 1998;91:1140.
[8] Chan WP, Lee CK, Kwong YL, Lam CK, Liang R. A novel mutation of Arg306 of factor V gene in Hong Kong Chinese. Blood 1998;91:1135.
[9] Bernardi F, Faioni EM, Castoldi E, Lunghi B, Castaman G, Sacchi E, Mannucci PM, et al. A factor V genetic component differing from factor V R506Q contributes to the activated protein C resistance phenotype. Blood 1997;90: 1552–7.
[10] Lunghi B, Iacoviello L, Gemmati D, Dilasio MG, Castoldi E, Pinotti M, Castaman G, et al. Detection of new polymorphic markers in the factor V gene: association with factor V levels in plasma. Thromb Haemost 1996;75:45–8.
[11] Pepe G, Rickards O, Vanegas OC, Brunelli T, Gori AM, Giusti B, Attanasio M, et al. Prevalence of factor V Leiden mutation in non-European populations. Thromb Haemost 1997;77:329–31.
[12] Cushman M. Inherited risk factors for venous thrombosis. Hematol Am Soc Hematol Educ Program 2005:452–7.
[13] Noe DA, Murphy PA, Bell WR, Siegel JN. Acute-phase behavior of factor VIII procoagulant and other acute-phase reactants in rabbits. Am J Physiol 1989;257: R49–56.
[14] Tsai AW, Cushman M, Rosamond WD, Heckbert SR, Tracy RP, Aleksic N, Folsom AR. Coagulation factors, inflammation markers, and venous thromboembolism: the longitudinal investigation of thromboembolism etiology (LITE). Am J Med 2002;113:636–42.
[15] Christiansen SC, Cannegieter SC, Koster T, Vandenbroucke JP, Rosendaal FR. Thrombophilia, clinical factors, and recurrent venous thrombotic events. JAMA May 18 2005;293:2352–61.
[16] Biswas A, Bajaj J, Ranjan R, Meena A, Akhter MS, Yadav BK, Sharma V, et al. Factor V Leiden: Is it the chief contributor to activated protein C resistance in Asian-Indian patients with deep vein thrombosis? Clin Chim Acta 2008;392:21–4.
[17] Undas A, Williams EB, Butenas S, Orfeo T, Mann KG. Homocysteine inhibits inactivation of factor Va by activated protein C. J Biol Chem 2001;276:4389–97. [18] Graf LL, Welsh CH, Qamar Z, Marlar RA. Activated protein C resistance assay detects
thrombotic risk factors other than factor V Leidenq. Am J Clin Pathol 2003;119:52–60.
[19] Lecumberri R, Ceberio I, Montes R, López ML, Alberca I, Rocha E, et al.qEvaluation of the factor V HR2 haplotype as a risk factor for ischemic cerebrovascular diseaseq. Haematologica 2003;88:236–7.
[20] Duran R, Biner B, Demir M, Celtik C, Karasalihoğlu S. Factor V Leiden mutation and other thrombophilia markers in childhood ischemic stroke. Clin Appl Thromb Hemost 2005;11:83–8.
[21] Folsom AR, Rosamond WD, Shahar E, Cooper LS, Aleksic N, Nieto FJ, Rasmussen ML, et al. Prospective study of markers of hemostatic function with risk of ischemic stroke. The Atherosclerosis Risk in Communities (ARIC) Study Investigators. Circulation 1999;100:736–42.
[22] O'Donnell J, Mumford AD, Manning RA, Laffan M. Elevation of FVIII: C in venous thromboembolism is persistent and independent of the acute phase response. Thromb Haemost 2000;83: 10–3.
[23] Henkens CM, Bom VJ, van der Meer J. Lowered APC-sensitivity ratio related to increased factor VIII-clotting activity. Thromb Haemost 1995;74:1198–9.