EFFECT OF PRANAYAMA BREATHING TOWARD PEAK EXPIRATORY FLOW RATE (PEFR) AND THE FREQUENCY OF RECURRENCE OF
PATIENTS WITH ASTHMA BRONCHIALE BASED ON ADAPTATION NURSING THEORY
Nian Afrian Nuari, Didit Damayanti STIKES Karya Husada Kediri E-Mail : [email protected]
ABSTRACT
Breathing Exercise have been widely used as complementary therapy people with asthma bronchiale. The goal this research is to analize effect of pranayama breathing Peak expiratory flow rate (PEFR) and the frequency of recurrence in patients with asthma bronkiale. This study used a design draft Pre Experimental Design with One Group Pre-Post Test. The samples in this study used purposive sampling technique with 10 respondents, while the instrument measured the value of PEFR used a flow meter and the frequency of recurrence in patients with asthma bronchiale checklist sheet and analyzed using the dependent sample t test (paired t test) with α 5%. The results showed that most respondents (90%) showed PEFR values increased and 70% of respondents experienced a decrease in the frequency of recurrence of Bronchial Asthma after intervening pranayama breathing. From the analysis of Paired T Test on PEFR values obtained p = 0.001 and the frequency of recurrence of asthma obtained p = 0.003 so it can be concluded that there is the effect of pranayama breathing with PEFR values and the frequency of recurrence of Asthma Bronchiale. There is a significant influenced on pranayama breathing with PEFR values and the frequency of recurrence of patient AsthmaBronchiale. Based on adaptation nursing theory, Pranayama relates to the process of adaptive coping mechanisms to minimized the frequency of recurrence and maximize lung function, the nurse helps strengthen coping regulator is to provide Pranayanama exercises and cognator aspects, by providing information to avoid the trigger factor for asthma bronchiale.
Keywords: Pranayama, Breathing, PEFR, recurrence, Asthma , Adaptation, Nursing
INTRODUCTION
Asthma is one of the problems for the people who were raised in various ages. Asthma is a chronic inflammatory disease of respiratory tract disorder characterized by episodes of wheezing, difficulty breathing, chest tightness and coughing. According to WHO, about 100 to 150 million people worldwide are people with Asthma. This number continues to grow as many as 180,000 people annually. In Indonesia, the prevalence of asthma is not known for certain, but estimated 2-5% of Indonesia's
population suffer from asthma (MOH, 2006).
with asthma in East Java in 2003 as many as 21 925 people.
To assess the severity of the disturbance can be assessed by lung function tests, namely the examination spirometridan examination Peak expiratory flow (APE). In addition to using spirometry, APE values can be obtained through a simple examination using meter peak expiratory flow (PEF meter). The results of pulmonary function tests in patients with asthma, it is known the existence of airway obstruction when FEV1 (forced expiration volume first second) / FVC (forced vital capacity) <75% or FEV1 <80% predicted values. Monitoring Peak Ekspiratory Flow Rate (PEFR) is important to assess severe asthma, the degree of diurnal variation, the treatment response time of an acute attack, detection of deterioration asymptomatic before it becomes serious, the identification of the originator for example exposure to the working environment and the frequency of recurrence of asthma (Guidelines for the diagnosis and management of asthma in Indonesia, 2003). In the study Ambareesha, Kondam et al (2012) reported on a study on medical students showed pranayama breathing can improve pulmonary function (Vital Capacity, Forced Vital Capacity and Peak expiratory Flow Rate). Proper asthma management among others are making near-normal lung function, prevent recurrence, control regularly and improve your fitness with exercise or exercise that is recommended (Yunus, 2006). Train the respiratory muscles is one of the interventions on Bronchial asthma patients. Many theories that explain how to train respiratory muscles are expected nati can improve lung function is the one that Pranayama breathing techniques.
Pranayama breathing exercises of yoga is more concentrated on breathing and can be applied in patients with asthma. Pranayama breathing beneficial to increase oxygen intake to the maximum, and the circulation of blood to and from the lungs
that can improve lung function (Nadera, Reyna, 2009). Research Pramanik, et al. (2009) in adult patients found that respiratory bhastrika pranayamic in adults able to stimulate the frequency and duration of nerve impulses that activate the receptor pulmonary during tidal volume. It was able to increase vasodilation in blood vessels to lower peripheral resistance in the blood vessels so that it can lower blood pressure. , The results of the study Bhargava R (1998), shows Pranayama affected by changes in the autonomic nervous associated with breathing and increasing vagal rhythm and reduce sympathetic changes. The novelty of this study is the implementation of Pranayama breathing is rarely applied by asthmatics and have not done much research in Indonesia on pranayama breathing with asthma sufferers in Indonesia. Therefore, it was necessary to examine the influence this pranayama breathing lung function in asthma patients and the frequency of recurrence of the disease.
PURPOSE
The purpose of this research was to determine the effectiveness of the methods of Pranayama Breathing in lowering the value of Peak expiratory flow rate (PEFR) and the frequency of recurrence in patients with Bronchial asthma. Experiment Design One Group Pre-Post Test.
Place and Time Research
In this study, researchers set a number of samples of 10 people with a sampling technique by using purposive sampling. Criteria for inclusion in this study is 1. Patients Asthma bronchiale are willing to become respondents and 18-70 years old
2. Patient has no status asthmaticus 3. Patients Asthma bronchiale is not dependent bronchodilator drugs Exclusion criteria in this study are patients with asthma who experience complications tract infections penafasan others (Pneumonia, COPD)
Research Instruments 1) Value PEFR
Measuring instruments used in the form of tools and the Peakflow meter sheet check list
2) Frequency of Recurrence of Asthma
The instrument used was the observation sheet
Data collection
The study begins with FGD (Focus Group Discussion) accompanied by experts together with the women and pranayama breathing explanation of the procedure to the respondent. Once that is done pre-test to measure the value of PEFR and asthma relapse frequency experienced by respondents. Respondents to intervene for 1 month and monitored by researchers. Within a period of one month later, researchers conducted a post test to measure the return value of PEFR and asthma relapse frequency.
Data analysis
Bivariate analysis was conducted to determine differences in PEFR value and frequency of recurrence of asthma at the time of pre-test and post-test with statistical test dependent sample t test (Paired t test) with α (standard error) of 5%.
RESULTS
Characteristics of Respondents a.Age
The frequency distribution of Bronchial Asthma patients based on age, can be seen below:
Source: Primary Data
Figure 1. Frequency Distribution Based on Age asthma patients in Puskesmas Bendo Kediri June 2014
Based on Figure 1 indicates as many as five respondents (50%) had 61-70 years of age, 3 respondents (30%) were aged 51-60 years, 10% aged 31-40 years and 10% of respondents aged 41-50 years.
b. Gender
Bronchial asthma patients the frequency distribution by sex can be seen below:
Source: Primary Data
Figure 2. Diagram Frequency Distribution by Sex asthma patients in Puskesmas Bendo Kediri June 2014
c.Length of Suffering from Bronchial Asthma
The frequency distribution of Bronchial Asthma patients by long suffering from asthma can be seen below:
60% 40%
1-5 Tahun 6-10 Tahun
Source: Primary Data
Figure 3. Frequency Distribution Based on Old Suffers Asthma in Puskesmas Bendo Kediri June 2014
Based on Figure 3 show as much as 6 respondents (60%) suffered from asthma for 6-10 years and 4 respondents (40%) suffered from asthma for 1-5 years.
d.Height
The frequency distribution of Bronchial Asthma patients based on height can be seenbelow:
Source: Primary Data
Figure 4. Diagram Frequency Distribution Based on Height Respondents in Puskesmas Bendo Kediri June 2014
Based on Figure 4 shows as many as eight respondents (80%) have a height of
141-150 cm, 1 respondents (10%) have a height of 131-140 cm and 1 respondent (10%) have a height of 151-160 cm.
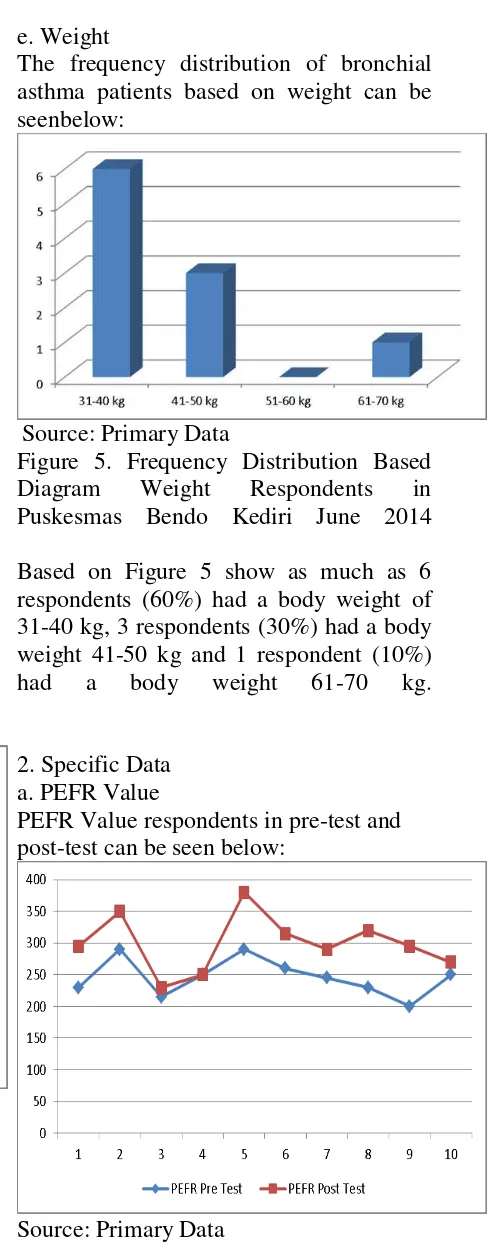
e. Weight
The frequency distribution of bronchial asthma patients based on weight can be seenbelow:
Source: Primary Data
Figure 5. Frequency Distribution Based Diagram Weight Respondents in Puskesmas Bendo Kediri June 2014
Based on Figure 5 show as much as 6 respondents (60%) had a body weight of 31-40 kg, 3 respondents (30%) had a body weight 41-50 kg and 1 respondent (10%) had a body weight 61-70 kg.
2. Specific Data a. PEFR Value
PEFR Value respondents in pre-test and post-test can be seen below:
Source: Primary Data
Test in Puskesmas Bendo Kediri June 2014
Based on Figure 6. show as much as 9 respondents (90%) experienced an increase in the value of Pranayama Breathing PEFR after intervention and 1 respondent (10%) did not experience an increase in the value of PEFR after the intervention.
b. Recurrence frequency Bronchial Asthma
Frequency of recurrence of bronchial asthma in pre-test and post-test can be seen below:
Source: Primary Data
Figure 7. Diagram Frequency of Recurrence Respondents When Pre Test and Post Test in Puskesmas Bendo Kediri June 2014
Based on Figure 7. shows before the intervention as much as 6 respondents (60%) experienced a recurrence frequency 3-4x / month, a total of three respondents (30%) experienced a recurrence frequency 1-2x / month, and as many as 1 respondents (10%) experienced a frequency recurrence 5-6x / month. After the intervention of Pranayama Breathing many as three respondents (30%) to not relapse, 3 respondents (30%) had experienced a recurrence frequency 1-2x / month and 3 respondents (30%) experienced a recurrence frequency 3-4x / month.
DATA ANALYSIS
Normality Test using Kolmogorov Smirnov test data analysis with statistical tests Paired t test showed that the obtained PEFR p value of 0.001 (p <0.05), which means there are differences PEFR values before and after the intervention pranayama breathing. While the frequency of recurrence of asthma was obtained p 0.003 (p <0.05), which means that there are differences in the frequency of asthma relapse before and after intervention pranayama breathing.
DISCUSSION
1. Value Analysis PEFR Before Intervention Guide Pranayama Breathing
The result showed that prior to dintervensi Pranayama Breathing by 5 respondents (50%) have value PEFR below 250 l / sec and as one of the respondents (10%) have value PEFR 250 l / sec, and as many as four respondents (40%) have PEFR values above 250 l / sec. This suggests that in patients with asthma tend to have below normal PEFR value in accordance with the count age and height.
To assess the severity of a disorder that occurs in asthma can be assessed by lung function tests, namely the examination of spirometry and peak expiratory flow inspection (APE). In addition to using spirometry, APE values can be obtained through a simple examination using meter peak expiratory flow (PEF meter). The results of pulmonary function tests in patients with asthma, it is known the existence of airway obstruction when FEV1 (forced expiration volume first second) / FVC (forced vital capacity) <75% or FEV1 <80% predicted values.
the identification of the originator for asthma tend to decrease and male gender also tends to decrease due to the influence of smoking history PEFR and others. While the value of PEFR in adults who suffer lung disease also experienced the largest decrease in the value of 50-80%. This is consistent with research that people who suffer from respiratory problems such as asthma bronchiale impaired PEFR.
The results showed that as many as 8 respondents (80%) have a height of 141-150 cm and as much as 6 respondents (60%) had a body weight of 31-40 kg. PEFR value of the respondents varies according to height dimilki respondents. This is according to research Mulyadi (2011) states that the normal PEFR values associated with the individual's height and weight of individuals and PEFR values are also affected by age, gender, history of respiratory problems and lung disease. It can be concluded that the normal value is affected PEFR weight and height.
2. Value Analysis PEFR After Intervention Guide Pranayama Breathing
The result showed that after intervention Breathing Pranayama as much as 2 respondents (20%) had PEFR values below 250 l / sec and 8 respondents (80%) had PEFR values above 250 l / sec. This is consistent with research Ambareesha, Kondam et al (2012) reported on a study on medical students showed pranayama breathing can improve pulmonary function (Vital Capacity, Forced Vital Capacity and Peak expiratory Flow Rate).
Proper asthma management among others are making near-normal lung function, prevent recurrence, control regularly and improve your fitness with exercise or exercise that is recommended (Yunus, 2006). Train the respiratory muscles is one of the interventions on Bronchial asthma patients. Many theories that explain how to train respiratory muscles which are expected later can improve lung function is the one that Pranayama breathing techniques.
Pranayama breathing exercises of yoga is more concentrated on breathing and can be applied in patients with asthma. Pranayama breathing beneficial to increase oxygen intake to the maximum, and the circulation of blood to and from the lungs that can improve lung function (Nadera, Reyna, 2009).
In normal conditions we use 10-15% of our ability to breathe every day. Pranayama exercises will increase the amount of blood that are exchanged in the lungs. In normal conditions the amount of air entering the lungs in one minute keparu is as much as 16 x adult patients found that respiratory bhastrika pranayamic in adults able to stimulate the frequency and duration of nerve impulses that activate the receptor pulmonary during tidal volume. It was able to increase vasodilation in blood vessels to lower peripheral resistance in the blood vessels so that it can lower blood pressure. Given that stimulus will be an increase in lung function and affect the value of PEFR patients.
(focal, contextual and residual) to perform process control using coping mechanisms regulator and kognator that will provide a response adaptive or maladaptive to the stimulus (Tomey & ALIGOOD, 2006) , This occurs in asthma patients physiological changes in his body so that the need for coping to overcome it and to manage stress so it does not become a factor triggers that can cause an attack and increase the risk of recurrence.
To achieve adaptive coping thus minimizing the frequency of recurrence and maximize lung function, the nurse helps strengthen coping regulator is to give Pranayanama Breathing exercises and kognator aspects, by providing information to avoid the trigger factor to prevent recurrence Bronchial asthma. Pranayama Breathing is an attempt to regulate and control the breath consciously that include setting the length and duration of inhalation and exhalation as well as efforts to hold his breath. With the implementation of pranayama breathing regulator happen coping mechanisms capable of inhibiting the release of CO2 that stimulate Bohr effect that will increase the amount of catalyst in chemical reactions release of oxygen from hemoglobin, which will accelerate the distribution of oxygen to the tissues. Besides, the breathing exercises are also able to increase the use of NO (Nitric Oxcide) that stimulate Guanylil cyclase that activates cGMP and GTP which activates cGMP dependet that stimulates myosin light-chain phospatase activity which causes relaxation of the respiratory tract, causing dilation that can improve lung exhalation breathing can also improve muscle flexibility intercostalis,
pectoralis and trapezius resulting in increased levels of O2 in the lung that will improve lung function. With their coping mechanisms regulator must also be balanced with kognator by providing knowledge on the client to avoid the trigger factor of recurrence in clients with Bronchial asthma using cognitive-emotional path of perception (the information), the process of learning, judgment and emotional boost. With 4 components will occur kognator adaptive coping.
3. Analysis Of Recurrence Frequency Bronchial Asthma Before Pranayama Breathing Intervention
The result showed that before intervention Breathing Pranayama as 6 respondents (60%) experienced a recurrence frequency 3-4x / month, a total of three respondents (30%) experienced a recurrence frequency 1-2x / month, and as many as 1 respondents (10%) experienced a recurrence frequency 5-6x / month.
Based on the characteristics of respondents by age is obtained as much as 50% of asthma patients aged 61-70 years. Most who develop asthma in adulthood. Based on the Report of the Basic Health Research (RISKESDAS) in 2007 found that the tendency of the prevalence of asthma has a tendency prevalence increases with age. Airways of asthmatics have distinctive properties that is very sensitive to various stimuli. Asthma attacks can occur at any age from children to adults (Sandaru, 2007).
cause allergic reactions. This is consistent with the findings that most of the respondents have more than 30 years of age to the age where individuals experience hypersensitivity thus higher relapse frequency becomes higher.
Based on the characteristics of the sexes is obtained mostly female. This is consistent with the results of RISKESDAS 2007, which states that the prevalence of asthma is no distinction based on sex.
The results showed that as many as 8 respondents (80%) have a height of 141-150 cm and as much as 6 respondents (60%) had a body weight of 31-40 kg. Weight and height affect the respiratory muscle strength and lung function, these results related to the theory that someone who has a high body large it will have the function of pulmonary ventilation is higher than the smallish. Inspiratory and expiratory function is affected by the height and weight as the ability to inflate the chest will berbedapada every height and weight (Guyton & Hall, 2001).
4. Analysis Of Frequency Recurrence Bronchial Asthma After Intervention Guide Pranayama Breathing
The result showed that after intervention Breathing Pranayama as many as three respondents (30%) to not relapse, 3 respondents (30%) had experienced a recurrence frequency 1-2x / month and 3 respondents (30%) experienced a recurrence frequency 3-4x / month ,
The results of the study Bhargava R (1998), also showed Pranayama affected by changes in the autonomic nervous associated with breathing and increasing vagal rhythm and reduce sympathetic changes. Results were in line with this research that changes in the autonomic nervous which will improve the lung function of patients.
Pranayama Breathing reduce sympathetic activity and provide relaxation response. Relaxation of
skeletal muscles also increase lung expansion. During pranayama will increase the breathing pattern bronchiale which further inflates the blood perfusion to alveoli. It is capable of supporting a controlled breathing patterns and help reduce allergen sensitivity that comes from the environment. This mechanism can affect the allergic reactions that decrease the frequency of asthma relapse can be decreased.
Pranayama breathing in the lungs causing get plenty of oxygen and oxygen will flow throughout the body. If breathing is done regularly and concentrate, then the wave amplitude frequency bioelectrical energy fields in the body will take place slowly and steadily. This supports the activity of the cells and organs of the body become synchronized and stimulate spending antibodies that work against various sources of disease and stimulate spending hormones like melatonin, endorphins which calms the nerves and the mind. This is what causes asthma patients bronhiale can avoid recurring asthma attacks because the mind is relaxed and not stress cause the patient could avoid the stressor or allergens trigger asthma attacks.
CONCLUSION
REFERENCES
Ambareesha, kondam et al . 2012. A study to evaluate the effect of vital capacity (vc), forced vital capacity (fvc) and peak expiratory flow rate (pefr) in subjects practicing pranayama . Inter J Cur Res Rev. Vol 04 issue 19
Bhavanani AB , Sanjay Z , Madanmohan. 2011. Immediate effect of sukha pranayama on cardiovascular
variables in patients of
hypertension. International Journal Of Yoga Therapy [Int J Yoga Therap] . (21), pp. 73-6.
Bhargava R , Gogate MG , Mascarenhas JF. 1998. Autonomic responses to breath holding and its variations following pranayama. Indian Journal Of Physiology And Pharmacology [Indian J Physiol Pharmacol] 1998 Oct-Dec; Vol. 32 (4), pp. 257-64.
Black, Joyce & Hawk, Jane. 2005.
Medical Surgical Nursing; Clinical
Management For Positive
Outcome. St.Louis: Elsvier.Inc. Camalia, S.Sahat.2008. Pengaruh senam
asma terhadap kekuatan otot pernafasan dan fungsi paru pasien
asma di RSU Tangerang.
Thesis.Universitas Indonesia Dabhade AM ,Pawar BH , Ghunage MS ,
Ghunage VM. 2012. Effect of pranayama (breathing exercise) on arrhythmias in the human heart. Elsevier Country of Publication:
United States NLM ID: 101233160 Depkes RI. 2003. Pedoman diagnosis dan
penatalaksanaan asma di Indonesia Guyton & Hall . 2001. Buku Ajar Fisiologi
Kedokteran. Jakarta : EGC, hal 14, 119, 120, 122, 124, 126
Hidayat, Azis Alimul. 2007. Metode penelitian keperawatan dan tehnik analisis data. Jakarta: Salemba Medika
Khanam, AA, Sachdeva U & Gulleria R. 1996. Study Of Pulmonary and
Autonomic Functions Of Ashma Patients After Yoga Training. The Journal Physiology Pharmacology Volume 40 (4). 1996. Pp. 318-324 Mulyadi, Zulfiitri, & Nafsiah, Siti. 2011.
Analis Hasil PEFR Pada Pasien Gangguan Pernafasan Di Pesisir
Kota Banda Aceh. Jurnal
Respirology Indonesia Volume 31, No.2, 2011.
Nadera, Reyna, 2009. Menyembuhkan penyakit asma secara alami.
Jakarta: Gramedia
Nugroho, sigit. 2009.Terapi pernafasan pada penderita asma. Yogyakarta Nursalam. 2003. Konsep & Penerapan
Metodologi Penelitian Ilmu
Keperawatan: Pedoman Skipsi, Tesis, dan Instrumen Penelitian. Jakarta: Salemba Medika, hal 16-21
Notoatmodjo, Soekidjo. 2005. Metodologi penelitian kesehatan. Jakarta: Rineka Cipta.
Potter, Patricia A. 2005. Buku Ajar Fundamental Keperawatan Vol. 2.
Jakarta: EGC.
Prasetya, Arief Widya.. 2011. Pengaruh Latihan Nafas Metode Butekyo Terhadap Peak Expiratory Flow Rate (PEFR) dan Derajat Kontrol
Penderita Ashma. Thesis.
Universitas Airlangga
Pramanik, Tapas, Sharma, Hari Om,et al. (2009). Immediate Effect of
Slow Pace Bhastrika
Pranayama on Blood Pressure