ARTICLE
Human Milk Consumption and Full Enteral Feeding
Among Infants Who Weigh
<
1250 Grams
Paula M. Sisk, PhDa, Cheryl A. Lovelady, PhDb, Kenneth J. Gruber, PhDc, Robert G. Dillard, MDa, T. Michael O’Shea, MD, MPHa
aDepartment of Pediatrics, Wake Forest University School of Medicine, Winston-Salem, North Carolina;bDepartment of Nutrition andcSchool of Environmental Science,
University of North Carolina, Greensboro, North Carolina
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
Feeding intolerance is common and associated with late-onset sepsis in preterm infants. There are limited observational data and anecdotal evidence that human milk feeding is associated with shorter time to full enteral feeding in preterm infants.
What This Study Adds
This study contributes a prospective cohort study of extremely preterm infants in whom the complete composition of enteral feedings is known during enteral feeding advance-ment and indicates that a high proportion of human milk feeding improves after time to full enteral feeding.
ABSTRACT
OBJECTIVE.Establishing enteral feeding is an important goal in the care of very low birth weight infants. In such infants, receipt of ⱖ50 mL/kg per day human milk during hospitalization has been associated with shorter time to full enteral feeding. The objective of this study was to determine whether high proportions (ⱖ50%) of human milk during feeding advancement are associated with shorter time to full enteral feeding and improved feeding tolerance.
METHODS.This was a prospective cohort study of very low birth weight infants (n⫽
127) who were grouped into low (⬍50%;n⫽34) and high (ⱖ50%;n⫽93) human milk consumption groups according to their human milk proportion of enteral feeding during the time of feeding advancement. The primary outcomes of interest were ages at which 100 and 150 mL/kg per day enteral feedings were achieved.
RESULTS.The high human milk group reached 100 mL/kg per day enteral feeding 4.5 days faster than the low human milk group. The high human milk group reached 150 mL/kg per day enteral feeding 5 days faster than the low human milk group. After adjustment for gestational age, gender, and respiratory distress syndrome, times to reach 100 and 150 mL/kg per day were significantly shorter for those in the high human milk group. Infants in the high human milk group had a greater number of stools per day; other indicators of feeding tolerance were not statistically different.
CONCLUSION.In infants who weighedⱕ1250 g, enteral feeding that contained at least 50% maternal human milk was associated with fewer days to full enteral feedings.
Pediatrics2008;121:e1528–e1533
A
TTAINING FULL ENTERALfeeding is an important goal when caring for very lowbirth weight (VLBW) infants because of its association with a lower risk for late-onset sepsis,1–3 hepatic
dysfunction,4,5growth failure,6and poor mineral accretion.7Feeding intolerance occurs frequently in VLBW infants
as a result of medical instability, necrotizing enterocolitis, and immaturity of the gastrointestinal tract.8–11Centers in
the National Institute of Child Health and Human Development Network reported that for extremely low birth weight infants (⬍1000 g), age when full enteral feedings was reached ranged from 17 to 49 days12and the Vermont
Oxford Network “Got Milk” focus group reported that for infants who weighed 750 to 1000 g, the average time to reach full enteral feedings was 26 days.13
Clinicians use a variety of feeding strategies to compensate for gastrointestinal immaturity and to improve feeding tolerance. These include early feeding (ⱕ4 days of age) or late feeding (⬎4 days of age),14minimal enteral feeding (ⱕ105
kJ/kg per day [25 kcal/kg per day] forⱖ5 days versus no feeding,15continuous versus intermittent bolus feeding,16rapid
versus slow advancement,17and gastric versus transpyloric feeding tube placement.18In systematic reviews, early feeding,
minimal enteral feeding, and rapid advancement of feeding have been associated with improved feeding tolerance and/or shorter time to full enteral feeding, but no definitive conclusions have been reached regarding the clinical benefits of each of these methods. Moreover, there are conflicting findings for continuous versus intermittent bolus feeding methods16,19
and no apparent benefit from transpyloric versus gastric feeding18with regard to improved feeding tolerance.
Conse-quently, uncertainty regarding the best feeding methods for VLBW infants remains, and determining optimal feeding
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-2110
doi:10.1542/peds.2007-2110
Key Words
human milk, enteral feeding, prematurity, very low birth weight
Abbreviations
VLBW—very low birth weight HM— human milk GA— gestational age HMF— human milk fortifier NPO—nothing by mouth RDS—respiratory distress syndrome NEC—necrotizing enterocolitis HHM— high human milk LHM—low human milk HR— hazard ratio CI— confidence interval
Accepted for publication Dec 13, 2007
Address correspondence to Paula M. Sisk, PhD, Department of Pediatrics, Wake Forest University School of Medicine, One Medical Center Blvd, Winston-Salem, NC 27157. E-mail: [email protected]
methods presents an important issue because withholding or limiting feedings may contribute to gastrointestinal im-maturity, suboptimal nutrition, and growth restriction in preterm infants.20
Feeding human milk (HM), either the infant’s own mother’s milk or donor milk, may improve feeding tol-erance in preterm infants.21 Schanler et al22 observed
that infants who received at least 50 mL/kg per day HM during hospitalization had fewer episodes of feeding in-tolerance and shorter time to reach full enteral feedings, regardless of other feeding interventions; however, us-ing HM volume as the exposure variable rather than the HM proportion of the total enteral feeding volume may have confounded these findings, because compared with more unstable infants, healthier infants are usually fed sooner and the feedings advanced more rapidly.
The purpose of this study was to analyze the associ-ation between HM proportion of enteral feeding and time to full feedings and feeding tolerance. We catego-rized exposure to HM on the basis of the proportion received during the time of feeding advancement. We hypothesized that the infants who received at least 50% of enteral feedings as HM would reach full enteral feed-ing at an earlier age and experience less feedfeed-ing intoler-ance than those who received⬍50%.
METHODS
Sample and Setting
The study was conducted in Winston-Salem, NC, at For-syth Medical Center, a referral center for women at high risk for obstetric complications. The study participants were infants who were delivered with birth weights between 700 and 1500 g between May 2001 and August 2003 and whose mothers agreed to participate in a study comparing anxiety levels before and after lactation counseling.23A prospective sample of 200 mother–infant
pairs was targeted to provide a basis for detecting a preintervention/postintervention difference in State Trait Anxiety Scores. Exclusion criteria for this study were maternal illicit drug use during pregnancy, HIV infection, age⬍18 years, and non-English speaking. Of 208 eligible mother–infant pairs, 94% (n⫽196) agreed to participate in the study. For this analysis, we excluded infants with birth weight ⬎1250 g (the 50th percentile for 28 weeks’ gestation),24who are at very low risk for
delayed enteral feeding, thereby reducing the sample to 134 infants. The institutional review boards of Wake Forest University School of Medicine, Forsyth Medical Center, and the University of North Carolina at Greens-boro approved the study, and all mothers signed a writ-ten informed consent.
Research Design
The study used a prospective cohort design in which the infants and mothers were enrolled within 72 hours of birth. Parenteral nutrition was begun on the first or second day of life when the infant’s gestational age (GA) wasⱕ30 weeks or when enteral feedings were not tol-erated for⬎24 hours. Enteral feedings were begun when the infant was regarded as stable by the attending
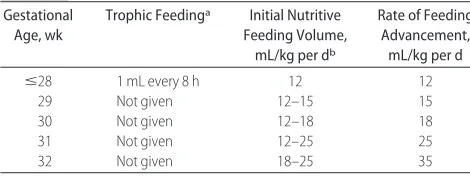
neo-natologist and advanced according to the established feeding guidelines for this NICU (Table 1). When⬃100 to 120 mL/kg per day feeding was achieved, parenteral nutrition was discontinued. Decisions to withhold feed-ings were made by the attending neonatologist accord-ing to the enteral feedaccord-ing guidelines stated in Table 1 or when the neonatologist determined that the infant’s medical condition was unstable.
All mothers in the study were encouraged to express milk for their infants regardless of their feeding plan before preterm delivery and were counseled by an in-ternational board-certified lactation consultant regard-ing the procedure for collection and storage of HM.25
Mothers were asked to bring their milk whenever they were able to visit their infants. Infants received HM only from their own mother. Maternal milk was used (when the mother chose to express milk) in the sequence it was expressed, either fresh or frozen to⫺20°C. Preterm for-mula (Enfamil Premature Forfor-mula 24 calories/ounce [Mead Johnson, Evansville, IN]) was given when the mother chose to formula feed or when there was insuf-ficient maternal milk to meet the infant’s nutritional needs. When feeding of 100 mL/kg per day was achieved and when HM was available, HM fortifier (HMF) was added, 1 packet to 25 mL of HM (Enfamil Human Milk Fortifier or Similac Human Milk Fortifer [Abbott Labo-ratories, Columbus, OH]). HMF was continued until the infant’s weight reached 2500 g or until hospital dis-charge.
Outcome Measures
The primary outcome was age at which full feedings for hydration (100 mL/kg per day) and full feedings for growth (150 mL/kg per day) were consumed. Secondary outcomes of interest were indicators of feeding toler-ance, caloric intake from enteral sources during feeding advancement, time to regain birth weight, and average
TABLE 1 Enteral Feeding Guidelines Used During the Study Period
Gestational Age, wk
Trophic Feedinga Initial Nutritive
Feeding Volume, mL/kg per db
Rate of Feeding Advancement, mL/kg per d
ⱕ28 1 mL every 8 h 12 12
29 Not given 12–15 15
30 Not given 12–18 18
31 Not given 12–25 25
32 Not given 18–25 35
Use HM or 24-cal/oz preterm infant formula. Add HM fortifier when 100 mL/kg per day enteral feeding is achieved.
aTrophic feeding given to infants with a GA ofⱕ28 weeks when abdomen is nontender and
nondistended on physical examination and abdominal radiograph appears normal or nonspe-cific. Trophic feedings are given for at least 24 hours before the initiation of nutritive feeding.
bNutritive feedings are given when the patent ductus arteriosus is closed or clinically
daily weight gain during the hospitalization. Indicators of feeding tolerance were gastric residual volumes (mL/ day), episodes of emesis per day, days of nothing by mouth (NPO), stools per day, glycerin suppositories given per week, days parenteral nutrition was given, and days central line access was maintained.
Caloric intake (kJ/kg per day [kcal/kg per day]) from enteral sources was calculated from the enteral feedings during the period of feeding advancement (from the first day enteral feedings were given until 150 mL/kg per day enteral feedings was consumed). HM was assumed to be 83.68 J/oz (20 cal/oz).26 HMF contained 14.644 J per
packet (3.5 cal per packet). Average weight gain (g/kg per day) during the hospitalization was calculated from the day birth weight was regained until hospital dis-charge. Infants were studied throughout hospitalization, and data were collected from the infant’s medical chart by research study assistants at the same time the study was conducted.
Respiratory distress syndrome (RDS) was defined as supplemental oxygen requirement for ⬎24 hours. Ne-crotizing enterocolitis (NEC) was defined as pneumatosis on radiograph. Patent ductus arteriosus was diagnosed by cardiac echocardiogram, and all cases were included regardless of the treatment received.
Data Analysis
Data were analyzed with SPSS computer software (SPSS Inc, Chicago, IL). The characteristics of the groups were compared with Mann-Whitney U test for continuous variables and2for categorical variables. GA and birth
weight were highly correlated; therefore, all statistical analyses were conducted adjusting for GA and then again for birth weight. Results were reported for both analyses when the results were significantly different. Cox proportion hazards regression analysis was used to test time-to-event data: age when 100 mL/kg per day and 150 mL/kg per day enteral feeding were achieved, number of days parenteral nutrition was given, and
number of days central line access was maintained.
P⬍.05 was considered statistically significant.
RESULTS
Characteristics of Patients
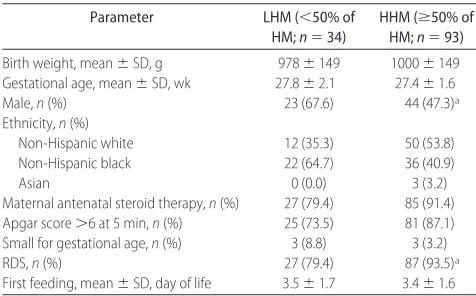
The findings of this study are based on the results ob-tained on 127 infants. From the initial sample of 134 infants, 7 were not included in the analysis because they did not achieve 150 mL/kg per day enteral feeding dur-ing the hospitalization as a result of death (n ⫽ 3) or transfer to a hospital closer to home (n⫽4). There were 11 sets of twins and 1 set of triplets. No differences in conclusions were noted when multiples were excluded; therefore, they were included in the sample. Ninety-eight percent of the mothers initiated milk expression in the hospital. Table 2 provides demographic and clinical features of the 34 infants who during the time of feeding advancement (ie, from the first feeding until 150 mL/kg per day enteral feeding was received) received⬍50% of enteral feeding as HM (low HM [LHM]) and the 93 infants who receivedⱖ50% HM (high HM [HHM]). The HHM group had a higher incidence of male gender and RDS after birth. There were no significant differences in other clinical features before initiation of enteral feed-ings.
Primary Outcome
The HHM group reached 100 mL/kg per day enteral feeding 4.5 days faster than the LHM group (median [interquartile range]: 15.0 days [13.0 –20.0] vs 19.5 days [11.8 –29.3]; Table 3). The HHM group reached 150 mL/kg per day enteral feeding 5 days faster than the LHM group (median [interquartile range]: 22.0 [19.0 – 29.5] vs 27.0 [18.7–39.3]). Time to reach 100 mL/kg per day (hazard ratio [HR]: 1.53 [95% confidence interval (CI): 1.02–2.31];P⫽.04) and 150 mL/kg per day (HR: 1.80 [95% CI: 1.16 –2.78]; P ⫽.008) was significantly shorter for the HHM group. After adjustment for GA, gender, and RDS, the results were similar (100 mL/kg per day HR: 1.86 [95% CI: 1.19 –2.89]; P ⫽.006) and 150 mL/kg per day HR: 2.13 [95% CI: 1.34 –3.38];P⫽
.001). (HRs of⬎1 indicate that the factor was associated with a shorter time to the event of interest, eg, attain-ment of 100 mL/kg per day.) The difference in time to 150 mL/kg per day is illustrated in the Kaplan-Meier curve (Fig 1).
TABLE 2 Demographic and Clinical Features Among Infants, Grouped According to the HM Proportion of Enteral Feedings During the Period of Feeding Advancement to 150 mL/kg per Day
Parameter LHM (⬍50% of
HM;n⫽34)
HHM (ⱖ50% of HM;n⫽93)
Birth weight, mean⫾SD, g 978⫾149 1000⫾149
Gestational age, mean⫾SD, wk 27.8⫾2.1 27.4⫾1.6
Male,n(%) 23 (67.6) 44 (47.3)a
Ethnicity,n(%)
Non-Hispanic white 12 (35.3) 50 (53.8)
Non-Hispanic black 22 (64.7) 36 (40.9)
Asian 0 (0.0) 3 (3.2)
Maternal antenatal steroid therapy,n(%) 27 (79.4) 85 (91.4)
Apgar score⬎6 at 5 min,n(%) 25 (73.5) 81 (87.1)
Small for gestational age,n(%) 3 (8.8) 3 (3.2)
RDS,n(%) 27 (79.4) 87 (93.5)a
First feeding, mean⫾SD, day of life 3.5⫾1.7 3.4⫾1.6
aSignificantly different (P
⬍.05).
TABLE 3 Age When Enteral Feeding Goals Were Achieved and the Crude and Adjusted Cox Regression HR for Infants With HHM Compared With Infants With LHM
Parameter HHM LHM Crude HR Adjusted HRa
100 mL/kg per day
15.0 (13.0–22.0) 19.0 (12.0–29.0) 1.53 (1.02–2.31)b 1.86 (1.19–2.89)c
150 mL/kg per day
22.0 (19.0–29.5) 27.0 (18.8–39.3) 1.80 (1.16–2.78)c 2.13 (1.34–3.38)c
HHM:n⫽93; LHM:n⫽34.
aAdjusted for GA, male gender, and RDS. bP
⫽.04.
Nutritional Outcomes
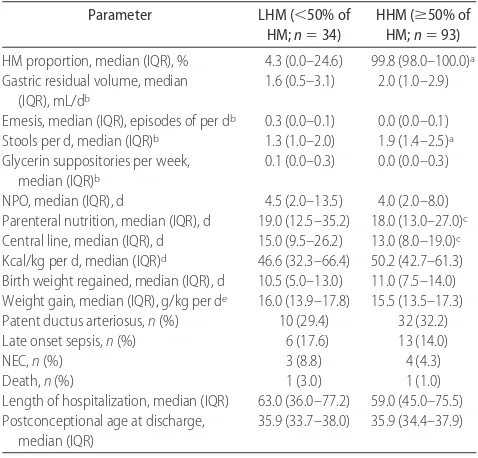
The HHM group had a significantly greater number of stools per day than the LHM group (Table 4). There were no differences in other variables related to feeding tol-erance. The HHM group received parenteral nutrition and required central line access significantly fewer days compared with the LHM group. Enteral caloric intake during the feeding advancement period (kJ/kg per day [kcal/kg per day]), age when birth weight was regained, and weight gain (g/kg per day) during the hospitaliza-tion were similar between groups.
Clinical Diagnoses and Medical Outcomes
There was no difference in incidence of patent ductus arteriosus, late-onset sepsis, or death (Table 4). There was a lower incidence of NEC; however, the number of cases was too small to determine statistical significance. To determine whether NPO status after diagnosis of NEC contributed to differences in age of achieving 100 and 150 mL/kg per day, we conducted analyses with NEC cases excluded. With these cases excluded, the results were similar to the results with the cases of NEC in-cluded for both time to reach 100 mL/kg per day (HR: 1.76 [95% CI: 1.10 –2.81];P⫽.02) and 150 mL/kg per day (HR: 2.21 [95% CI: 1.34 –3.62]; P ⫽ .002). There were no statistically significant differences in length of hospital stay or postconceptional age at discharge.
DISCUSSION
Enteral feeding that consisted of a high proportion (ⱖ50%) of HM during the time of feeding advancement was associated with an earlier age that full feedings for hydration (100 mL/kg per day) and for growth (150 mL/kg per day) were achieved among infants with birth weight ⱕ1250 g. In addition, HM was associated with shorter duration of parenteral nutrition and central line access; however, we found no significant differences in gastric residual volume, number of emesis episodes, or NPO days. HM feeding was associated with more fre-quent stool output, and this is consistent with previously
observed differences in stooling patterns of infants who were fed predominately HM compared with infant for-mula.27
HM contains bioactive agents (hormones, growth fac-tors, and antiinflammatory agents) that may contribute to the maturation of gastrointestinal function and pro-tect against inflammation. In vitro28and animal studies29
indicated that polyamines and growth factors in HM stimulate intestinal cell proliferation and intestinal villi growth by increasing epithelial cell proliferation and lactase, maltase, and sucrase activity.30 In preterm
in-fants, studies indicated that HM promotes adaptation of the gastrointestinal tract from an intrauterine physio-logic state to an extrauterine physiophysio-logic state as evi-denced by decreased intestinal permeability,31 higher
lactase activity,32and shorter time to achieve full enteral
feeding.32The presence of milk lipases in HM also may be
a factor contributing to better digestion and absorption of lipid and better tolerance of feeding.33,34 One
addi-tional possibility is that gastric emptying, an important clinical indicator of feeding tolerance, is faster with HM feeding.35
Our results are consistent with those of Schanler et al,22 who observed that VLBW infants who received at
least 50 mL/kg per day HM during their hospital course compared with infants who received 100% preterm for-mula reached full tube feedings 8 days sooner and had shorter duration of parenteral nutrition. We also ob-served significantly shorter duration of parenteral
nutri-TABLE 4 Nutritional Outcomes and Clinical Diagnoses Among Infants, Grouped According to the HM Proportion of Enteral Feedings During the Period of Feeding Advancement to 150 mL/kg per Day
Parameter LHM (⬍50% of
HM;n⫽34)
HHM (ⱖ50% of HM;n⫽93)
HM proportion, median (IQR), % 4.3 (0.0–24.6) 99.8 (98.0–100.0)a
Gastric residual volume, median (IQR), mL/db
1.6 (0.5–3.1) 2.0 (1.0–2.9)
Emesis, median (IQR), episodes of per db 0.3 (0.0–0.1) 0.0 (0.0–0.1)
Stools per d, median (IQR)b 1.3 (1.0–2.0) 1.9 (1.4–2.5)a
Glycerin suppositories per week, median (IQR)b
0.1 (0.0–0.3) 0.0 (0.0–0.3)
NPO, median (IQR), d 4.5 (2.0–13.5) 4.0 (2.0–8.0)
Parenteral nutrition, median (IQR), d 19.0 (12.5–35.2) 18.0 (13.0–27.0)c
Central line, median (IQR), d 15.0 (9.5–26.2) 13.0 (8.0–19.0)c
Kcal/kg per d, median (IQR)d 46.6 (32.3–66.4) 50.2 (42.7–61.3)
Birth weight regained, median (IQR), d 10.5 (5.0–13.0) 11.0 (7.5–14.0) Weight gain, median (IQR), g/kg per de 16.0 (13.9–17.8) 15.5 (13.5–17.3)
Patent ductus arteriosus,n(%) 10 (29.4) 32 (32.2)
Late onset sepsis,n(%) 6 (17.6) 13 (14.0)
NEC,n(%) 3 (8.8) 4 (4.3)
Death,n(%) 1 (3.0) 1 (1.0)
Length of hospitalization, median (IQR) 63.0 (36.0–77.2) 59.0 (45.0–75.5) Postconceptional age at discharge,
median (IQR)
35.9 (33.7–38.0) 35.9 (34.4–37.9)
IQR indicates interquartile range.
aSignificantly different,P⫽.001. bData collected during the first 28 days of life. cCox regression analysis: significantly different,P⬍.01.
dKilocalories from enteral sources only during the feeding advancement period. eCalculated from the day birth weight was regained until hospital discharge. HHM groupa
Age, d
80 60
40 20
0 Cumulative rate of achieving full feedings for growth, %
1.0
0.8
0.6
0.4
0.2
0.0
LHM group
FIGURE 1
tion and central line access. Although this might be expected to decrease the risk for late-onset sepsis, we previously reported finding no difference between the 2 groups,36 perhaps because the incidence for the entire
sample was somewhat lower than previously reported rates.1,37
It is important to note that HM feeding was associated with an earlier age at which full enteral feeding was achieved and, as previously reported,36a lower incidence
of NEC. Our analysis in this study suggests that shorter time to full enteral feeding in the HHM group was not related solely to a lower incidence of NEC. Also, these results are consistent with the observation by Lucas and Cole38that rate of feeding advancement was associated
with NEC in formula-fed infants only. Reducing the time required to achieve full enteral feeding without an in-crease in NEC by increasing proportion of HM intake has important clinical and economic implications. NEC and late-onset sepsis are associated with significantly longer lengths of stay and higher hospital costs compared with VLBW infants without these complications.1,39
In contrast to the findings of Schanler et al,22we did
not observe a slower rate of growth in the predominately HM-fed infants. This difference in study findings may be attributable to a similar caloric intake during feeding advancement, use of 24-cal/oz formula, addition of HMF to HM (1 packet to 25 mL of HM) when 100 mL/kg per day feeding was achieved, and continuation of HMF until a weight of 2500 g was reached or the infant was discharged from the hospital. Also, in contrast to the findings of Schanler et al, we did not observe a difference in incidence of late-onset sepsis or length of stay; how-ever, our study had adequate power to detect only rel-atively large differences in these outcomes.
Certain limitations of our study should be noted. First, the data were collected and the sample size was chosen for another purpose; thus, the sample size did not provide sufficient power to detect clinically impor-tant differences in some of the outcomes that we stud-ied. A second limitation is that infants were not ran-domly assigned to HM feeding groups, so unmeasured confounders might explain the differences that we ob-served. A third limitation is that we did not measure the macronutrient content of HM in this study. The energy and protein content of HM is variable, and differences could have influenced growth; however, for calculations of energy intake from HM, we used an average caloric content of 280.328 J/dL (67 cal/dL [range: 267.776 – 301.248 J/dL (64 –72 cal/dL)]).26 A fourth limitation is
that our study did not measure time to full oral feeding; therefore, it is unknown if HHM intake has an impact on this important milestone. A fifth limitation is that this study was conducted at a single site. It is possible that our results were substantially affected by the particular feeding practices followed by the hospital and that alter-native feeding regimens might substantially affect the time to full enteral feeding. Also, feedings were initiated or withheld by the clinicians who cared for the infants according to the nursery enteral feeding guidelines rather than a research protocol, and the clinicians were not blinded to type of enteral feeding. This could be a
source of bias if clinicians had a preconceived assump-tion regarding the safety of HM in cases in which the physical examination was not clearly normal; however, nearly all mothers in this study initiated breast pumping, so clinicians rarely knew the exact composition of the enteral feedings. As a result of these limitations, the generalizability of our findings is limited and the repli-cation of this study with a larger data set is needed.
Strengths of this study include the prospective and complete data on feeding composition, which enabled us to report on HM proportion of enteral feeding and the use of a standardized feeding regimen. For clinicians, the finding that feedings that consist of at least 50% HM and are given during feeding advancement are associated with an earlier age at which full enteral feeding is achieved highlights the importance of intensive lactation support to mothers in the early postpartum period. We found, as part of the larger project, that providing lacta-tion educalacta-tion and lactalacta-tion support is effective at achieving high lactation initiation and duration of milk expression among mothers of VLBW infants.23 For
mothers of VLBW infants who do not plan to breastfeed, these findings may provide the impetus needed to ex-press milk during their infant’s hospitalization.
ACKNOWLEDGMENTS
This study was funded in part by a grant from the Inter-national Lactation Consultant Association.
We thank the mothers and infants who participated in the study. We also thank Mary Showalter, IBCLC, for recruitment and lactation counseling and the research assistants from the Department of Nutrition at the Uni-versity of North Carolina at Greensboro for data collec-tion.
REFERENCES
1. Stoll BJ, Hansen N, Fanaroff AA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD neo-natal research network.Pediatrics.2002;110(2 pt 1):285–291 2. Flidel-Rimon O, Friedman S, Juster-Reicher A, Amitay M,
Shinwell E. Early enteral feeding and nosocomial sepsis in very low birth weight infants.Arch Dis Child Fetal Neonatal Ed.2004; 89(4):F289 –F292
3. Ronnestad A, Abrahamsen TG, Medbo S, et al. Late-onset septicemia in a Norwegian national cohort of extremely pre-mature infants receiving very early full human milk feeding.
Pediatrics. 2005;115(3). Available at: www.pediatrics.org/cgi/ content/full/115/3/e269
4. Kumpf VJ. Parenteral nutrition associated liver disease in adult and pediatric patients.Nutr Clin Pract.2006;21(3):279 –290 5. Schanler RJ, Shulman RJ, Lau C, O’Brian Smith E, Heitkemper
MM. Feeding strategies for premature infants: randomized trial of gastrointestinal priming and tube-feeding method.Pediatrics.
1999;103(2):434 – 439
6. Dusick AM, Poindexter BB, Ehrenkrantz RA, Lemons JA. Growth failure in the preterm infant: can we catch up?Semin Perinatol.2003;27(4):302–310
7. Rohana J, Hasmawati J, Zulkifli SZ. Risk factors associated with low bone mineral content in very low birth weight infants.
Singapore Med J.2007;48(3):191–194
9. Berseth CL. Neonatal small intestinal motility: motor responses to feeding in term and preterm infants.J Pediatr.1990;117(5): 777–782
10. Carlos MA, Babyn PS, Marcon MA, Moore AM. Changes in gastric emptying in early postnatal life.J Pediatr.1997;130(6): 931–937
11. Al-Tawil Y, Klee G, Berseth CL. Extrinsic neural regulation of antroduodenal motor activity in preterm infants.Dig Dis Sci.
2002;47(12):2657–2663
12. Vohr BR, Wright LL, Dusick AM, et al. Center differences and outcomes of extremely low birth weight infants. Pediatrics.
2004;113(4):781–789
13. Kuzma-O’Reilly B, Duenas ML, Greecher C, et al. Evaluation, development, and implementation of potentially better practices in neonatal intensive care nutrition.Pediatrics.2003;111(4 suppl 1). Available at: www.pediatrics.org/cgi/content/full/111/4/SE1/ e461
14. Kennedy KA, Tyson JE, Chamnanvanakifj S. Early versus de-layed initiation of progressive enteral feedings for parenterally fed low birth weight or preterm infants.Cochrane Database Syst Rev.2000;(2):CD001970
15. Tyson JE, Kennedy KA. Trophic feedings for parenterally fed infants.Cochrane Database Syst Rev.2005;(3):CD000504 16. Premji S, Chessel L. Continuous nasogastric milk feeding
ver-sus intermittent bolus feeding for premature infants less than 1500 grams.Cochrane Database Syst Rev.2003;(1):CD001819 17. Kennedy KA, Tyson JE, Chamnanvanakifj S. Rapid versus slow
rate of advancement of feedings for promoting growth and preventing necrotizing enterocolitis in parenterally fed low-birth-weight infants. Cochrane Database Syst Rev. 2000;(2): CD001241
18. McGuire W, McEwan P. Transpyloric versus gastric tube feed-ing for preterm infants.Cochrane Database Syst Rev.2002;(3): CD003487
19. Dsilna A, Christensson K, Alfredsson L, Lagercrantz H, Blen-now M. Continuous feeding promotes gastrointestinal toler-ance and growth in very low birth weight infants.J Pediatr.
2005;147(1):43– 49
20. Clark RH, Thomas P, Peabody J. Extrauterine growth restric-tion remains a serious problem in prematurely born neonates.
Pediatrics.2003;111(5 pt 1):986 –990
21. Boyd CA, Quigley MA, Brocklehurst P. Donor breast milk versus infant formula for preterm infants: a systematic review and meta-analysis.Arch Dis Child Fetal Neonatal. 2007;92(3): F169 –F175
22. Schanler RJ, Shulman RJ, Lau C. Feeding strategies for prema-ture infants: beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics. 1999;103(6pt 1): 1150 –1157
23. Sisk PM, Lovelady CA, Dillard RG, Gruber KJ. Lactation coun-seling for mothers of very low birth weight infants: effect on maternal anxiety and infant intake of human milk.Pediatrics.
2006;117(1). Available at: www.pediatrics.org/cgi/content/ full/117/1/e67
24. Fenton TR. A new growth chart for preterm babies: Babson and Benda’s chart updated with recent data and a new format.
BMC Pediatr.2003;3(1):13–23
25. Arnold LD.Recommendations for Collection, Storage, and Handling of a Mother’s Milk for Her Own Infant in the Hospital Setting. 3rd ed. Denver, CO: Human Milk Banking Association of North America, Inc; 1999
26. Saarela T, Kokkonen J, Koivisto M. Macronutrient and energy contents of human milk fractions during the first six months of lactation.Acta Paediatr.2005;94(9):1176 –1181
27. Weaver LT, Lucas A. Development of bowel habits in preterm infants.Arch Dis Child.1993;68(3 Spec No):317–320
28. Capano G, Bloch KJ, Carter EA, Dascoli JA, Schoenfeld D, Harmatz PR. Polyamines in human and rat milk influence intestinal cell growth in vivo.J Pediatr Gastroenterol Nutr.1998; 27(3):281–286
29. Dvorak B, Fituch CC, Williams CS, Hurst NM, Schanler RJ. In-creased epidermal growth factor levels in human milk of moth-ers with extremely premature infants.Pediatr Res.2003;54(1): 15–19
30. Ma L, Xu RJ. Oral insulin like growth factor-1 stimulates intestinal enzyme maturation in newborn rats.Life Sci.1997; 61(1):51–58
31. Shulman RJ, Schanler RJ, Lau C, Heitkemper M, Ou CN, Smith EO. Early feeding, antenatal glucocorticoids, and human milk decrease intestinal permeability in preterm infants.Pediatr Res.
1998;44(4):519 –523
32. Shulman RJ, Schanler RJ, Lau C, Heitkemper M, Smith EO. Early feeding, feeding tolerance, and lactase activity in preterm infants.J Pediatr.1998;133(5):645– 649
33. Armand M, Hamosh M, Mehta NR, et al. Effect of human milk or formula on gastric function and fat digestion in the prema-ture infant.Pediatr Res.1996;40(3):429 – 437
34. Alemi B, Hamosh M, Scanlon JW, Salzman-Mann C, Hamosh P. Fat digestion in very low-birth-weight infants: effect of addition of human milk to low-birth-weight formula.Pediatrics.
1981;68(4):484 – 489
35. Ewer AK, Durbin GM, Morgan ME, Booth IW. Gastric empty-ing in preterm infants.Arch Dis Child.1994;71(1):F24 –F27 36. Sisk PM, Lovelady CA, Gruber KJ, Dillard RG, O’Shea TM.
Early human milk feeding is associated with a lower risk of necrotizing enterocolitis in very low birth weight infants.J Perinatol.2007;27(7):428 – 433
37. Fanaroff AA, Stoll BJ, Wright LL, et al. Trends in neonatal morbidity and mortality for very low birthweight infants.Am J Obstet Gynecol.2007;196(2):147.e1–147.e8
38. Lucas A, Cole TJ. Breast milk and neonatal necrotising entero-colitis.Lancet.1990;336(8730):1519 –1523