A comparison of the index of orthodontic treatment need
with the index of
outcome, complexity, and need
Arya Brahmanta, Bambang Sucahyo, and Noengki Prameswari Laboratory of Orthodontics
Dentistry Faculty Hang Tuah University Surabaya-Indonesia
ABSTRACT
The demand of orthodontic treatment for malocclusion is increasing in Indonesia. Malocclusions describe a spectrum of a deviation from the ideal to very severe anomalies. Dentist may have differing views of what should be. The IOTN is a useful tool for those interested in research into epidemiology of malocclusion. IOTN has two parts: the Aesthetic (AC) and Dental Health (DHC) components. The ICON index has been developed recently and claims among other things, to evaluate orthodontic treatment complexity. The index comprises five weighted measurements, and some of its structure to IOTN. The sum of the weighted scores is interpreted using cut-off values and score ranges to indicate the treatment need, complexity and degree of improvement. It is claimed that using ICON to make these assessments is more efficient than IOTN because it requires only a single measurement protocol. This literature study explain that the ICON provides an acceptable alternative to IOTN.
Key words: IOTN, ICON
Correspondence: Arya Brahmanta, Laboratory of Orthodontics, Dentistry Faculty, Hang Tuah
University. Arif Rahman Hakim no 150 Surabaya 60244, Indonesia. Email:
INTRODUCTION
Malocclusion describes a spectrum of deviation from the normal or ideal to very severe anomalies.
Clinicians and potential patients may have differing views of what should be treated and what should
be accepted as a modest and harmless variation. The multifactor nature of malocclusion, which
includes the patient’s expectations and psychological needs, physical characteristics of occlusion,
complexity of treatment and the degree of improvement aimed for by the orthodontist, makes it
difficult to standardize judgements.1
Occlusal indices have been widely used as a method of achieving a more uniform evaluation of
malocclusion into groups according to the level of treatment need such as IOTN and ICON.2 Dentist
may have differing views of what should be. The IOTN is a useful tool for those interested in research
into epidemiology of malocclusion. IOTN has two parts: the Aesthetic (AC) and Dental Health (DHC)
components. The ICON index has been developed recently and claims among other things, to evaluate
orthodontic treatment complexity. The index comprises five weighted measurements, and some of its
structure to IOTN. The sum of the weighted scores is interpreted using cut-off values and score ranges
to indicate the treatment need, complexity and degree of improvement. It is claimed that using ICON to
make these assessments is more efficient than IOTN because it requires only a single measurement
protocol. This literature study will explain that the ICON provides an acceptable alternative to IOTN.
Index of orthodontic treatment need (IOTN) and the function
The IOTN is a useful for those researches into Dental Public Health and the epidemiology of
malocclusion. This index attempts to rank malocclusion in terms of the significance of various occlusal
traits for an individual's dental health and perceived aesthetic impairment. It intends to identify those
individuals who would most likely benefit from orthodontic treatment. The index has two components,
the aesthetic and dental health components, which rank malocclusion in increasing priority according to
aesthetic considerations and dental health implication.3
Index of orthodontic treatment need (IOTN), is consist of two components: dental health component (DHC) and aesthetic component (AC) 4,5 DHC uses a simple ruler to guide the observer to the single worst feature of the malocclusion. There are 5 categories, from 1 representing no need for treatment to 5 representing a great need for treatment. The second component is Aesthetic Component (AC), consist of a ten point scale illustrated by a series of photographs which were rated for
attractiveness by a lay panel and selected as being equidistantly spaced through the range of grades.
Aesthetic Component (AC) of IOTN represent the dental attractiveness of prospective patients
that can be rated with reference to this scale. Grade 1 represents the most and grade 10 the least
attractive arrangement of teeth. The score reflects the aesthetic impairment. Monochrome photographs
are used for dental cast assessment. These have an advantage in that raters are not influenced by oral
hygiene, gingival conditions or poor colour matches in restorations affecting anterior teeth.3 Grade
1 represent the most aesthetic arrangement of the Dentition; grade 10 represent the least aesthetic
arrangement of the Dentition; grade 1-4 represent little or no treatment required; grade 5-7 represent
moderate or borderline treatment required, and grade 8-10 represent treatment required. Dental Health
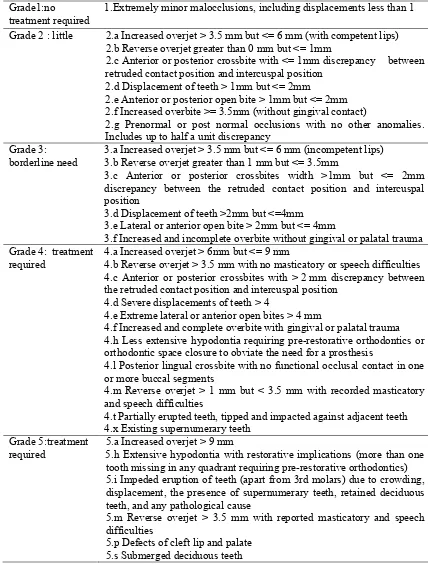
Table 1. (DHC) the dental health component IOTN
Grade1:no
treatment required
1.Extremely minor malocclusions, including displacements less than 1
Grade 2 : little 2.a Increased overjet > 3.5 mm but <= 6 mm (with competent lips) 2.b Reverse overjet greater than 0 mm but <= 1mm
2.c Anterior or posterior crossbite with <= 1mm discrepancy between retruded contact position and intercuspal position
2.d Displacement of teeth > 1mm but <= 2mm
2.e Anterior or posterior open bite > 1mm but <= 2mm 2.f Increased overbite >= 3.5mm (without gingival contact)
2.g Prenormal or post normal occlusions with no other anomalies. Includes up to half a unit discrepancy
Grade 3: borderline need
3.a Increased overjet > 3.5 mm but <= 6 mm (incompetent lips) 3.b Reverse overjet greater than 1 mm but <= 3.5mm
3.c Anterior or posterior crossbites width >1mm but <= 2mm discrepancy between the retruded contact position and intercuspal position
3.d Displacement of teeth >2mm but <=4mm 3.e Lateral or anterior open bite > 2mm but <= 4mm
3.f Increased and incomplete overbite without gingival or palatal trauma Grade 4: treatment
required
4.a Increased overjet > 6mm but <= 9 mm
4.b Reverse overjet > 3.5 mm with no masticatory or speech difficulties 4.c Anterior or posterior crossbites with > 2 mm discrepancy between the retruded contact position and intercuspal position
4.d Severe displacements of teeth > 4
4.e Extreme lateral or anterior open bites > 4 mm
4.f Increased and complete overbite with gingival or palatal trauma 4.h Less extensive hypodontia requiring pre-restorative orthodontics or orthodontic space closure to obviate the need for a prosthesis
4.l Posterior lingual crossbite with no functional occlusal contact in one or more buccal segments
4.m Reverse overjet > 1 mm but < 3.5 mm with recorded masticatory and speech difficulties
4.t Partially erupted teeth, tipped and impacted against adjacent teeth 4.x Existing supernumerary teeth
Grade 5:treatment required
5.a Increased overjet > 9 mm
5.h Extensive hypodontia with restorative implications (more than one tooth missing in any quadrant requiring pre-restorative orthodontics) 5.i Impeded eruption of teeth (apart from 3rd molars) due to crowding, displacement, the presence of supernumerary teeth, retained deciduous teeth, and any pathological cause
5.m Reverse overjet > 3.5 mm with reported masticatory and speech difficulties
Index of complexity outcome and need (ICON) and the function
Index of Complexity, Outcome, and Need (ICON) is claimed can be used to assess treatment need
as well as to assess treatment outcome. The index is based on the perception of treatment need and
outcome by 97 orthodontists from 9 countries (Germany, Greece, Hungary, Italy, Netherlands, Norway,
Spain, UK and USA,) who judged 240 dental casts for the assessment of treatment need and 98 paired
pre- and post treatment cases for assessment of treatment outcome.1
The index is simple to use, requiring only a millimeter ruler and an Aesthetic Component Scale.
The index is intended for use in the late mixed dentition and permanent dentition. Further, the index
may be applied clinically to patients and to casts without any modification. The ICON is unique in
incorporating an aesthetic score as an integral part of the evaluation of treatment need. Because it is
both an index of treatment need and an occlusal index of malocclusion severity, the ICON offers
significant advantages over other indices of treatment need.6
ICON assesses treatment need, treatment outcome acceptability, treatment complexity, and the
degree of improvement. To assess treatment need the pre-treatment study models are examined and
occlusal traits are scored according to the protocol below (Table 5). The five occlusal trait scores are
then multiplied by their respective weightings and summed. If the summary score is greater than 43,
treatment is indicated. Apply the index scoring method to the post-treatment models only. If the
summary score is less than 31 the outcome is acceptable. To assess treatment complexity, a five point
scale is used via the cut points for the 20 percentile intervals, using the ranges given from the
pre-treatment models. The degrees of improvement multiply the post-pre-treatment score by 4, and subtract the
result from the pre-treatment score. Use the ranges in to assign a grade as seen as table 2, 3, 4.7
When the index is used to assess treatment outcomes, it is assumed that an appropriate level of
co-operation was obtained from the patient. The index may require confirmation of the presence of teeth
using radiography. Except for the aesthetic assessment, occlusal traits are not scored to deciduous teeth
unless they are to be retained in the permanent dentition to obviate the need for a prosthetic
replacement, for example when the permanent tooth is absent.7
Table 2. ICON index variables, weightings and cut-off values for treatment need and outcome decisions
Occlusal trait ICON index Weighting
IOTN aesthetic component 7
Overbite 4
Crossbite 5
Treatment need cut-off 43
Treatment outcome cut-off 31
Table 3. ICON index complexity cut-off values
Complexity grade Score range
Table 4. ICON index score ranges, for rating of treatment improvement
Improvement grade Score range
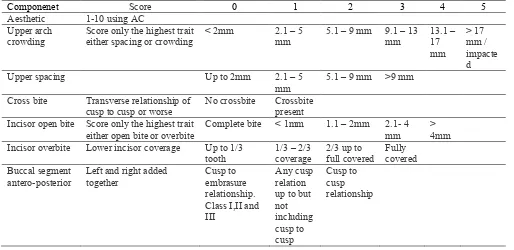
Table 5. Protocol for occlusal trait scoring
Componenet Score 0 1 2 3 4 5
Incisor open bite Score only the highest trait either open bite or overbite
Complete bite < 1mm 1.1 – 2mm 2.1- 4 mm
> 4mm Incisor overbite Lower incisor coverage Up to 1/3
Table above (Table 5) explain about protocol for occlusal trait scoring. The first component of occlusal trait scoring is aesthetic component that consist of ten pictures ranking dental attractiveness.1 The second component that must be scored is upper arch crowding/spacing. In this component, the difference between the sum of the mesio-distal tooth diameters and the available arch circumference in the upper arch reduced to a 5-point score. Impacted teeth in either arch immediately score 5. Impacted teeth must be unerupted. Ectopic or impacted against an adjacent tooth (excluding third molars but
including supernumerary teeth). Possess less than or equal to 4 mm of space between the adjacent
permanent teeth. Use average canine and premolar widths to estimate the potential crowding in the
mixed dentition, namely, 7 mm for pre-molars and lower canine, 8 mm for upper canine. Spacing in
one part of the arch will cancel out crowding elsewhere. Retained deciduous teeth (without permanent
successor) and erupted supernumerary teeth score as space (unless they are to be retained to obviate the
need for prosthesis). Lost teeth caused by trauma or extraction should be counted as space (unless
space is maintained for a prosthetic replacement). The third component is about crossbite anterior and
posterior transverse discrepancies of cusp to cusp or greater intercuspal position. The fourth component is used to score the incisor open bite/overbite. Open bite (except developmental conditions) is measured to the mid-incisal edges. Deep bite is measured to deepest part of overbite. If both traits are present only the highest score is counted. The last component is buccal segment antero-posterior. Quality of buccal segment interdigitation is measured (not Angle's classification). Both sides are scored
then added together.8,9
DISCUSSION
Index of Orthodontic Treatment Need (IOTN) in the General Dental Services is currently being
considered. IOTN were developed in the late 1980s to address the contentious issues of need for
orthodontic treatment and quality of outcome.8 Experience with IOTN has shown that the need for
treatment does not necessarily equate to the complexity of the treatment. It is important to make an
assessment of complexity for the following clinical reasons: 9 to identify the most appropriate setting in
which a patient should receive treatment, to allow meaningful assessment of treatment outcomes, to
identify cases that are likely to take longer to treat, to inform the patient of the likely success. The
factors which may determine the professional perception of orthodontic treatment complexity include:
cost of treatment, number of appointments, length of appointments, age of patient when treatment
commenced.9
protocols had to be learnt. Furthermore, neither index was appropriate for assessment of treatment
complexity, which still relied on clinical judgement.8
Index of Complexity, Outcome, and Need (ICON) promises an answer to some of these problems.
As a unified index of complexity, need and outcome, calibrated against an international panel of
orthodontists from Europe and America, its standards should be more appropriate to modern
orthodontics worldwide. ICON simple to use, requiring only a millimeter ruler and an Aesthetic
Component Scale. The index is intended for use in the late mixed dentition and permanent dentition.
Further, the index may be applied clinically to patients and to casts without any modification. The
ICON is unique in incorporating an aesthetic score as an integral part of the evaluation of treatment
need. Because it is both an index of treatment need and an occlusal index of malocclusion severity, the
ICON offers significant advantages over other indices of treatment need.7,8
The ICON consists of five components, each having been awarded a different weight according to
its relative importance. Component 1 of ICON has been adopted from the Aesthetic Component of the
IOTN. The other components include: upper arch crowding/ spacing, crossbite, incisor open
bite/overbite and buccal segment antero-posterior relationship. Each component can be measured on
patients or study casts. Furthermore, this index can be a useful tool in audit, research and orthodontic
decision-making. The ICON score determines level of need, complexity and degree of improvement as
a result of treatment. The ICON index has been developed recently and claims among other things, to
evaluate orthodontic treatment complexity. The sum of the weighted scores is interpreted using cut-off
values and score ranges to indicate the treatment need, complexity and degree of improvement. The
cut-off values are to give the index meaning and link the numerical ICON score to the original
subjective description of the 97 orthodontists.7
The general performance of the ICON index seems to be largely in agreement with IOTN for
assessing treatment need. Although ICON identified a higher proportion of the sample in need of
treatment compared with IOTN (AC), on which it is heavily based, it did not over score on the
proportion of cases identified for treatment on the grounds of dental health. This suggests that the
aesthetic component (AC) of the IOTN and ICON showed similar levels of sensitivity and ICON could
probably substitute IOTN (DHC) and produce largely similar results. The reliability assessment of the
indices and descriptive statistics are given. When used as an ordinal scale to express treatment
complexity, ICON has marginally lower but acceptable reliability as the use of IOTN to assign
treatment need categories. ICON appears able to substitute IOTN (AC) and IOTN (DHC) as a means of
measuring orthodontic treatment need. A value of greater than 43 for ICON defines a definite need for
The single index (ICON) which is easier to learn and use than IOTN could measure orthodontic
treatment need and treatment standards. The index could be easily incorporated into the orthodontic
assessment of a patient in general dental practice. It is claimed that using ICON to make these
assessments is more efficient than IOTN because it requires only a single measurement protocol. ICON
should prove to be a useful tool for research and audit, but if used alongside IOTN, could be an
additional burden in a busy hospital or practice setting. IOTN have been validated against UK dental
opinion and in an increasingly global environment, perhaps a more internationally recognized standard
should now be sought. ICON reflects the views of 97 orthodontists from eight European countries and
the USA, and may provide an acceptable alternative to IOTN.7,8
Based on research one-hundred-and-thirty cases were identified.7 With respect to residual need it
varied from 0.77 to 20.1% with respect to IOTN depending on the criteria examined. The residual
treatment need with respect to ICON was 17.2%. IOTN as an occlusal indices give differing failure
rates when used on the same patients with ICON being the most critical index. ICON was the most
valid with respect to identifying treatment failure. Its use would enable international comparison of
results. IOTN in the general dental services has been proposed. The conclusion in this review is ICON
would be quicker to learn, apply and more information could be gleaned than just treatment need.
ICON could probably substitute IOTN (DHC) and produce largely similar results.
REFERENCES
1. Koochek RAM, Shue-Te Yeh, Rolfe B, Richmond C. The relationship between index of complexity, outcome and need, and patients' perceptions of malocclusion: a study in general
dental practice. Br Dent J 2001; 191(6):325-29.
2. Fox NA, Daniels C, Gilgrass T. A comparison of the index of complexity outcome and need (ICON) with the peer assessment rating (PAR) and the index of orthodontic treatment need
(IOTN) Br Dent J 2002; 193(4):225-30.
3. Haag U, Colman, Zhang M. Quality of life and orthodontic treatment need related to occlusal indices. Dental Bulletins 2007; 8. (12) :1-5
4. Daniels CP, Richmond S. The development of the index of complexity, outcome and need (ICON). Br Dent J 2000; 27:149-62.
6. Firestone AR, Beck M, Beglin FM, Katherine WL. Validity of the index of complexity, outcome, and need (ICON) in determining orthodontic treatment need. Angle Orthod 2002; 72 (1):15–20.
7. Fox NA. Measuring failure of orthodontic treatment: a comparison outcome indicators. J Orthod 2004; 31:319-22.
8. Turbill. Can ICON replace IOTN and PAR. Br Dent J 2002; 193 (4):218.
9. Richmond S, Shaw WC, O’Brien KD, Buchanan IB, Stephen CD, Andrews M. The relationship between the index of orthodontic treatment need and consensus opinion of a panel of 74 dentist.
Br Dent J 1995; 178 (10):370-4.