Amniotic Fluid and Umbilical Cord Blood
Concentrations of Antidepressants in Three Women
Amy Hostetter, James C. Ritchie, and Zachary N. Stowe
Background: Pregnancy and the postpartum period are
a time of increased risk for women to develop mood disorders. As such, the reproductive safety data on antidepressant use during pregnancy have rapidly ex-panded over the last decade; however, there is rela-tively sparse information on maternal/fetal exchange of these medications and no data reporting their concen-trations in amniotic fluid.
Methods: We report on three women treated during
pregnancy with fluvoxamine, sertraline, and venlafaxine, respectively. Amniotic fluid at amniocentesis and umbili-cal cord blood and maternal blood at delivery were collected and analyzed for antidepressant concentrations using high performance liquid chromatography with UV detection.
Results: Antidepressant and metabolite concentrations
were detectable in all amniotic fluid samples, though parent compound concentrations were less than maternal serum and umbilical cord blood concentrations. No ad-verse effects of the medication were reported.
Conclusions: The presence of these antidepressants in
amniotic fluid suggests that fetal exposure to these medi-cations is continual and may occur through a variety of paths, thus accounting for increased fetal exposure. These paths include circulatory via placental passage, gastroin-testinal via fetal swallowing, and respiratory secondary to
fetal lung absorption. Biol Psychiatry 2000;48:
1032–1034 © 2000 Society of Biological Psychiatry
Key Words: Amniotic fluid, umbilical cord, placental
passage, antidepressant, pregnancy
Introduction
T
he extant literature on the reproductive safety of antidepressant medications has rapidly expanded over the past decade, though remarkably sparse information on the actual maternal/fetal exchange of these medicationshas been reported. A literature search (Medline 1960 – 1999) failed to identify any publications documenting human amniotic fluid concentrations of antidepressants; however, other studies have quantified human amniotic fluid concentrations of anticonvulsants (Meyer et al 1988; Omtzigt 1992), fentanyl (Shannon et al 1998), nicotine (Luck and Nau 1984), and various antibacterial agents (Pacifici and Nottoli 1995).
The amniotic fluid is produced in part by the amniotic cells, but is derived primarily from maternal blood (Sadler 1985). The composition of amniotic fluid varies with gestational time. In later pregnancy, the fluid includes fetal urine and lung liquid secretion. Drugs excreted by the fetal kidney enter the amniotic fluid and recirculate due to fetal swallowing (Morgan 1997).
This report describes three cases of antidepressant use during pregnancy with collection of both amniotic fluid during amniocentesis and umbilical cord blood at delivery. All women received a comprehensive risk– benefit assess-ment and were treated throughout their pregnancies at the Emory University Pregnancy and Postpartum Mood Dis-orders Program. Amniocentesis was planned as part of their obstetric care secondary to advanced maternal age in all three cases. Additional amniotic fluid (0.5 mL) and umbilical cord blood (3 mL) were collected at the sub-ject’s request to provide some measure of medication exposure.
Case A
Mrs. A is a 34-year-old married, white female treated with fluvoxamine 100 mg once daily for severe anxiety and obsessive thinking. Mrs. A presented at 11 weeks gesta-tion; her pregnancy was planned, and she conceived while taking the medication. An amniocentesis was performed at 16 weeks gestation. At 29 weeks gestation the fluvoxam-ine was increased to 150 mg once daily secondary to increased anxiety. At 40 weeks gestation Mrs. A had an uncomplicated vaginal delivery of a female infant who weighed 3.23 kg and had appearance, pulse, grimace, activity, respiration (APGAR) scores of 8 and 9.
From the Departments of Psychiatry and Behavioral Sciences (AH, JCR, ZNS), Gynecology and Obstetrics (ZNS), and Pathology (JCR), Emory University School of Medicine, Atlanta, Georgia.
Address reprint requests to Zachary N. Stowe, M.D., Emory University School of Medicine, Department of Psychiatry & Behavioral Sciences, 1639 Pierce Drive NE, Suite 4003, Atlanta GA 30322.
Received February 8, 2000; revised June 6, 2000; accepted June 7, 2000.
Case B
Mrs. B is a 40-year-old married, white female treated with sertraline monotherapy 150 mg/day for major depression. Mrs. B conceived on this dose of sertraline, and the pregnancy progressed without complication. At 17 weeks gestation the patient underwent amniocentesis. At 37.6 weeks gestation the patient’s dose was increased to 175 mg once daily secondary to increased depressive symp-toms. At 39 weeks gestation Mrs. B had an uncomplicated vaginal delivery of a female infant who weighed 3.66 kg and had APGAR scores of 9 and 9.
Case C
Mrs. C is a 40-year-old married, white female who presented at 15 weeks gestation with a twin pregnancy. Before becoming pregnant she was being treated with venlafaxine, 100 mg twice daily (b.i.d), for depression and anxiety. It was a planned pregnancy and she had tapered off the venlafaxine before conception. She reported symp-tom recurrence at 6 weeks gestation. At 15 weeks gesta-tion she restarted venlafaxine 100 mg b.i.d. An amniocen-tesis was performed at 17 weeks gestation. At 30 weeks gestation the venlafaxine was increased to 150 mg b.i.d. secondary to increasing symptoms of depression and irritability. Mrs. C delivered male and female infants at 36 weeks gestation by cesarean section secondary to breech presentation. The twins received APGAR scores of 7 and 9 for twin A and 9 and 9 for twin B, with weights of 3.1 kg and 2.7 kg, respectively.
All three amniocenteses were performed without com-plication, and maternal and umbilical cord blood was collected at the time of delivery. All infants had
uncom-plicated deliveries, and no adverse effects of medication exposure were reported.
Methods and Materials
All three subjects were recruited from the Emory Pregnancy and Postpartum Mood Disorders Program for participation in the current case series. Written informed consent was obtained for collection of maternal serum and umbilical cord blood and the use of data obtained from manuscripts on other biological samples (such as amniotic fluid and placental tissue) in submission.
The quantification of parent compound and metabolite con-centrations in the above samples was accomplished, following a solid-phase extraction, by isocratic high performance liquid chromatography (HPLC) with UV detection. High performance liquid chromatography separation was performed using a 1003
2–mm stainless steel Keystone Scientific (Bellefonte, PA) MOS
22 Hypersil (C8) reverse phase column, particle size 3 mm. Analysis was conducted with a Hewlett Packard (Palo Alto, CA) HPLC chemstation equipped with a computer, a series 1100 degasser, quanternary pump, autosampler, and diode array de-tector, as detailed in previous reports (Stowe et al 1997, 2000). The limit of detection of parent compounds and metabolites was 2.0 ng/mL.
Results
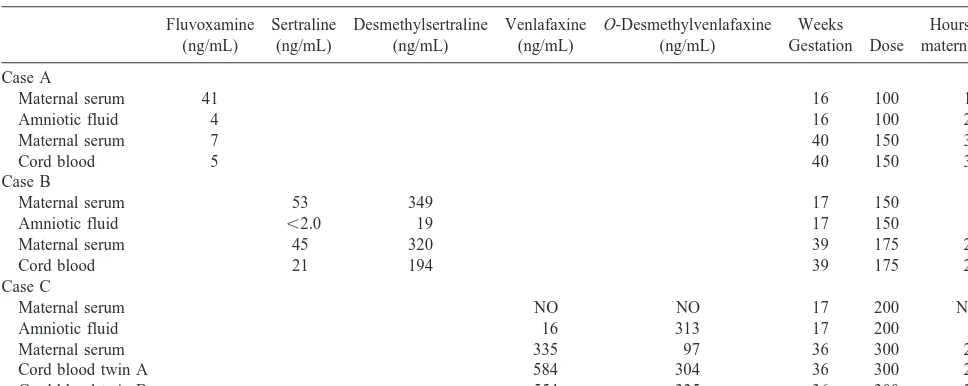
Fluvoxamine and venlafaxine were detectable in amniotic fluid; sertraline was below the limit of detection. All parent compounds were found in umbilical cord samples. Similarly, the metabolites of sertraline and venlafaxine were detectable in both amniotic fluid and umbilical cord blood. The data are shown in Table 1. In all cases, the women had taken a stable dose of antidepressant for
Table 1. Antidepressant Concentrations in Amniotic Fluid, and Maternal and Umbilical Cord Serum
Fluvoxamine (ng/mL)
Sertraline (ng/mL)
Desmethylsertraline (ng/mL)
Venlafaxine (ng/mL)
O-Desmethylvenlafaxine (ng/mL)
Weeks Gestation Dose
Hours after maternal dose
Case A
Maternal serum 41 16 100 18
Amniotic fluid 4 16 100 20
Maternal serum 7 40 150 30
Cord blood 5 40 150 30
Case B
Maternal serum 53 349 17 150 1
Amniotic fluid ,2.0 19 17 150 1
Maternal serum 45 320 39 175 21
Cord blood 21 194 39 175 21
Case C
Maternal serum NO NO 17 200 NO
Amniotic fluid 16 313 17 200 3
Maternal serum 335 97 36 300 20
Cord blood twin A 584 304 36 300 20
Cord blood twin B 554 325 36 300 20
NO, not obtained.
Antidepressants in Amniotic Fluid BIOL PSYCHIATRY 1033
greater than five half-lives of elimination before amnio-centesis and delivery. All samples were collected when serum levels had reached steady state; however, times after maternal dose at sampling varied by case and may influence antidepressant concentrations. Information on the maternal/fetal exchange of venlafaxine (Case C) is limited, as maternal blood was not obtained at the time of amniocentesis, and the amniocentesis was performed after 2 weeks of treatment wit venlafaxine, as opposed to 4 months for Cases A and B.
Discussion
These novel data demonstrate that antidepressants are present in amniotic fluid, though in lower concentrations than maternal serum and umbilical cord blood. The pres-ence of these antidepressants in amniotic fluid provides an additional pathway of continuous fetal exposure. There-fore, exposure via maternal circulation/placental passage may not account for total exposure. These data may explain the results in a preliminary rat study conducted by our group (Owens et al 1998). Briefly, in a series of five pregnant rats treated with selective serotonin reuptake inhibitors (SSRIs) via osmotic minipumps the pups were delivered by cesarean section and had brain concentrations that were 50 –75% of the maternal brain concentration in ng/mg protein. These laboratory results are very prelimi-nary but suggest that “in utero” exposure can result in higher, if not frankly therapeutic, central nervous system exposure to antidepressants. The long-term consequences of such exposure are unknown. In the current case series, it is reassuring that there were no obstetric complications or acute adverse effects noted in the four infants.
For Case A (fluvoxamine), maternal serum at the time of delivery was lower than at the time of amniocentesis, despite an increase in dose. Clearly the maternal serum concentrations 18 hours after dose at amniocentesis (41 ng/mL), while the samples were obtained 30 hours after dose at delivery (7 ng/mL), may reflect a more rapid circulatory clearance of fluvoxamine relative to its appear-ance in amniotic fluid. Another potential contributing factor is the impact of the physiologic changes of later pregnancy on the metabolism of the medications, poten-tially yielding a decreased serum concentration (Redmond 1985). All three women in this case series required an increase of their daily medication dose in the third trimes-ter to maintain symptom control. This is consistent with our report on the dose of SSRIs across pregnancy, which demonstrated that two thirds of subjects require an in-crease in dose during pregnancy to maintain euthymia (Hostetter 2000). The tendency for antidepressant dose
increases during pregnancy underscores the importance of studies designed to determine the amount of fetal exposure to psychotropic medications.
When one considers the expanding data, incidence of psychiatric illness in women of reproductive years, and the broadening use of SSRIs, one realizes there is a need to assess concerns of accumulation in the fetal circulation and, more importantly, in fetal brain tissue. Expansion of such data will provide a method for comparing fetal exposure between medications both for clinical treatment planning and designing long-term infant follow-up studies.
References
Hostetter A, Stowe ZN, Strader JR, McLaughlin E, Llewellyn A (2000): Dose of selective serotonin uptake inhibitors across pregnancy: Clinical implications. Depress Anxiety 11:51–57. Luck W, Nau H (1984): Exposure of the fetus, neonate, and nursed infant to nicotine and cotinine from maternal smoking.
N Engl J Med 311:672.
Meyer FP, Quednow B, Potrafki A, Walther H (1988): Pharma-cokinetics of anticonvulsants in the perinatal period. Zentralb
Gynakol 110:1195–1205.
Morgan DJ (1997): Drug disposition in mother and foetus. Clin
Exp Pharmacol Physiol 24:869 – 873.
Omtzigt JGC, Nau H, Los FJ, Pijpers L, Lindhout D (1992): The disposition of valproate and its metabolites in the late first trimester and early second trimester of pregnancy in maternal serum, urine, and amniotic fluid, effect of dose, co-medica-tion, and the presence of spina bifida. Eur J Clin Pharmacol 43:381–388.
Owens M, Hostetter AL, Knight DL, Ritchie JC, Llewellyn AM, Nemeroff CB, Stowe ZN (1998): Fetal exposure to Sert antagonist antidepressants in rats. Poster session presented at the annual meeting of the Society for Neuroscience, Los Angeles.
Pacifici GM, Nottoli R (1995): Placental transfer of drugs administered to the mother. Clin Pharmacokinet 28:235–269. Redmond GP (1985): Physiological changes during pregnancy and their implications for pharmacological treatment. Clin
Invest Med 8:317–322.
Sadler TW (1985): In: Tracy T, editor. Langman’s Medical
Embryology, 5th ed. Baltimore: Williams & Wilkins, 101–
102.
Shannon C, Jauniaux E, Gulbis B, Tiry P, Sitham M, Bromley L (1998): Placental transfer of fentanyl in early human preg-nancy. Hum Reprod 13:2317–2320.
Stowe ZN, Cohen LS, Hostetter A, Ritchie JC, Owens MJ, Nemeroff CB (2000): Paroxetine in human breast milk and nursing infants. Am J Psychiatry 157:185–189.
Stowe ZN, Owens MJ, Laundry JC, Kilts CD, Ely T, Llewellyn A, Nemeroff CB (1997): Sertraline and desmethylsertraline in human breast milk and nursing infants. Am J Psychiatry 154:1255–1260.
1034 BIOL PSYCHIATRY A. Hostetter et al