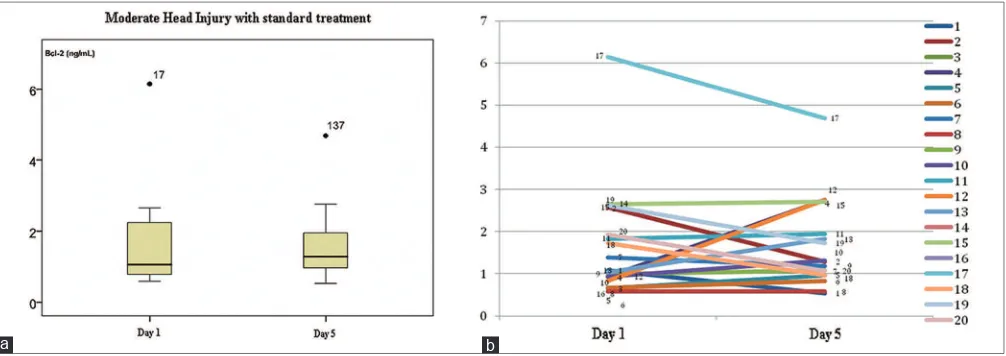
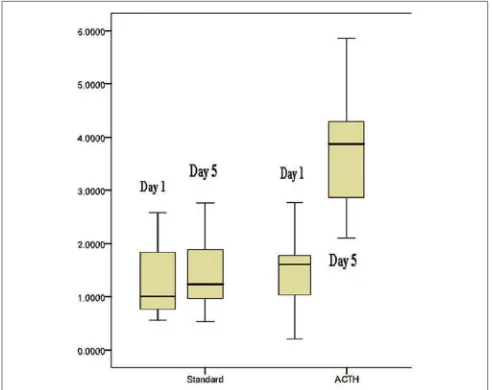
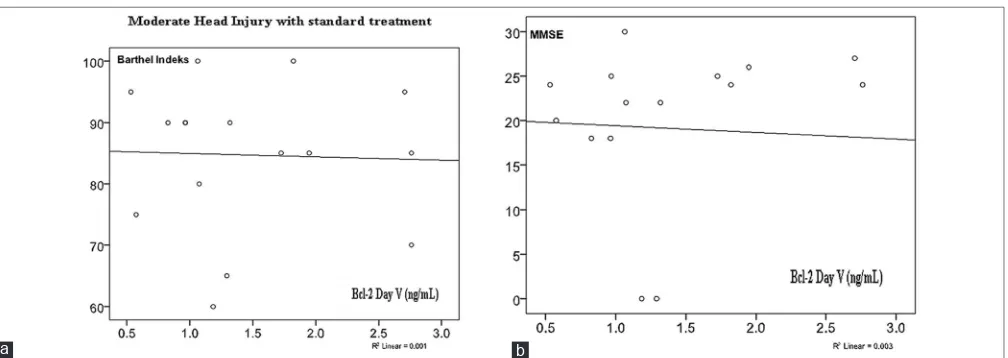
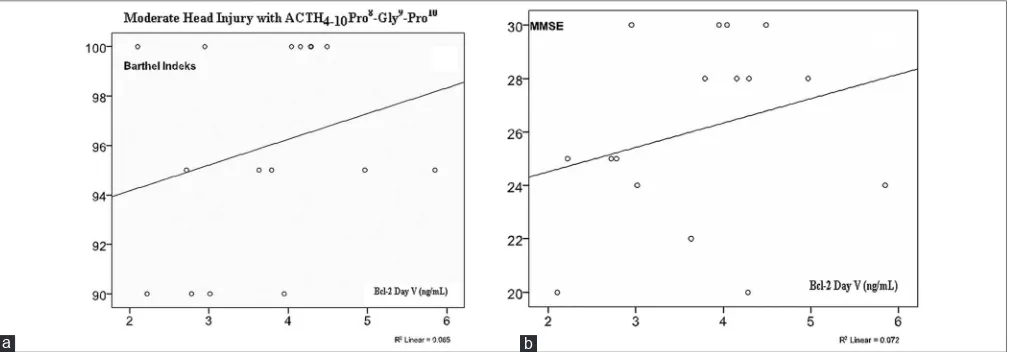
The increase of serum Bcl‑2 concentration in moderate head injury outcome: The role of ACTH4‑10Pro8‑Gly9‑Pro10
Teks penuh
Gambar
Dokumen terkait
Berdasarkan hasil dari pengolahan dan analisis data yang telah dilaksanakan, maka dapat ditarik kesimpulan bahwa terdapat pengaruh yang signifikan antara layanan
Anomali akan berpotensi menghambat kinerja jaringan pada sebuah trafik jaringan tertentu. Karena sifatnya menimbulkan aktivitas yang tidak wajar dalam trafik
Pada pelaksanaan layanan penguasaan konten dilakukan wawancara antara guru bimbingan dan konseling, adapun deskripsi hasil wawancara; (1) Persiapan yang dilakukan
Pentingnya komunikasi bagi manusia tidaklah dapat dipungkiri begitu juga halnya bagi suatu organisasi. Dengan adanya komunikasi yang baik suatu organisasi dapat berjalan
Pada level ini staff Kementerian Agamamengrim kan idberita, isi berita, url, tanggal berita untuk melakukan proses tambah berita, setelah data berita sudah di proses maka akan di
pokja pekaiaan Konstuksiunit Layanar Pergadaan (utP) tGhpabn Lebong derFr ininen$rnsnl6tJtasr. nenhngan Umum Oeng; pasdudifkasi -p.d, ry pelrer *rixld
Deuouring time blunt thou the Lyons pawes, And make the earth deuoure her owne sweet brood, Plucke the keene teeth from the fierce Tygers yawes, And burne the long liu’d Phaenix
Berdasarkan Surat Penetapan Pemenang Lelang Nomor : 08/TAP/DPU/BM-10/POKJA/2014 tanggal 19 Mei 2014 tentang Penetapan Pemenang Lelang Paket Pekerjaan Bantuan Peningkatan
