1
GI bleeding prevention on long term antiplatelet use
I Dewa Nyoman Wibawa
Div.Gastroentero-hepatology,Dept.of Internal Medicine Udayana Univ.;School of Medicine/Sanglah General Hospital.
Extended abstract
For the purpose of prevention of attacks or cardiovascular events later often used antiplatelet either single or double. The use of antiplatelet to prevent the occurrence of cardiovascular events is often accompanied by the risk of gastrointestinal bleeding. Several approaches can be undertaken for the purpose of preventing the occurrence of gastrointestinal bleeding in the use of long-term antiplatelet therapy. One of the options is by using Proton Pump Inhibitors (PPIs).
As we know that aspirin causes direct damage to the gastric epithelium and inhibits prostaglandin production by the gastric mucosa, leading to ulcerations and an estimated 2-fold increased risk of GI bleeding with low-dose aspirin alone.1,2 The additional use of antiplatelet and antithrombotic
agents with steroidal and no steroidal anti-inflammatory drugs increases the risk.2,3
Use of PPIs in patients taking antiplatelet therapy has been associated with a significant reduction in the risk of GI bleeding, ulcers, and erosions in data from observational and randomized clinical trials.1
Pantoprazole and rabeprazole interfere minimally with the cytochrome P450 system and may potentially not exhibit a similar interaction. 4,5 The use
of prasugrel instead of clopidogrel in acute coronary syndromes patients undergoing percutaneous coronary intervention can be considered and has been shown to cause platelet inhibition even in the face of clopidogrel no responsiveness, albeit at the expense of increased bleeding.1
Newer antiplatelet agents that are not dependent on the cytochrome P450 is enzymes such as ticagrelor could be used in acute coronary syndromes treated invasively or conservatively. Administration of the PPI at a different time than the administration of clopidogrel showed inconsistent results in the studies that evaluated this strategy. It is unclear whether the release pharmacokinetics of the particular omeprazole formulation used in COGENT had any impact on the results of the trial. A different gastro protective drugs such as H2 receptor antagonists can be used, although they have been shown to confer a somewhat more modest protective effect than PPIs.1
In patients with non-variceal upper gastrointestinal bleeding, prophylaxis with anti-secretory drugs such as PPIs reduces the risk of GI bleeding. Early endoscopy is useful for both the diagnosis and the therapeutic management of GI bleeding. Antiplatelet therapy should be resumed immediately after endoscopic hemostasis of GI bleeding, unless the bleeding is life threatening.6
2 from randomized clinical trials because new retrospective studies, no matter how statistically sound, will only add confusion to the matter. Until then, the benefit of PPIs in reducing bleeding events (and treating GI symptoms) must be factored into decision making when faced with patients with high GI bleeding risk requiring antiplatelet therapy.1
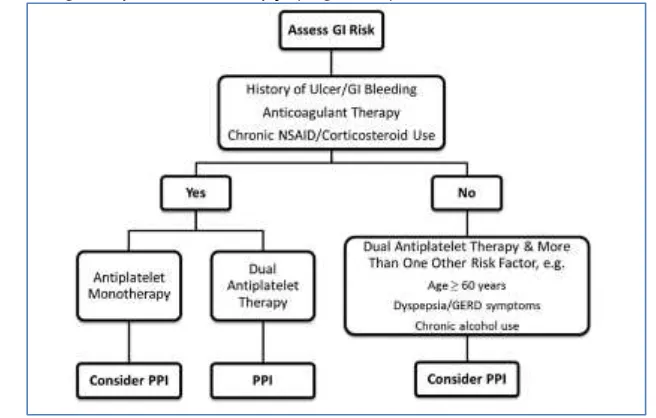
Clinical characteristics can be used to guide the need for PPIs in patients taking antiplatelet therapy (Figure 1).
Figure 1. Proposed algorithm for use of proton pump inhibitors (PPIs) in patients requiring antiplatelet therapy. GI indicates gastrointestinal; NSAID, no steroidal anti-inflammatory drug; and GERD, gastro esophageal reflux disease.1
TABLE 1. Recommendations Available Related to GI Bleeding in Patients Taking Anticoagulant and Antiplatelet Drugs.
A systematic review GI bleeding prevention on long term antiplatelet use stated that gastroenterology guidelines tended to primarily focus on the bleeding-associated risk for patient, and cardiovascular guidelines tended to focus on the risk that is associated with discontinuing anticoagulant or antiplatelet therapy. The specific recommendations of these are summarized in Table 1. 7
[image:2.595.129.457.168.377.2] [image:2.595.113.504.455.555.2]3 percent), as compared with 1 of the 62 patients in the lansoprazole group (1.6 percent), had a recurrence of ulcer complications (adjusted hazard ratio, 9.6; 95 percent; confidence interval, 1.2 to 76.1). Of these 10 patients, 4 had evidence of a recurrence of H. pylori infection and 2 had taken no steroidal anti-inflammatory drugs before the onset of complications. Patients in the lansoprazole group were significantly less likely to have a recurrence of ulcer complications than patients in the placebo group (P=0.008). There was no significant difference in mortality between the two groups. Base on this study the author concluded that in patients who had ulcer complications related to the long-term use of low-dose aspirin, treatment with lansoprazole in addition to the eradication of H. pylori infection significantly reduced the rate of recurrence of ulcer complications.8
Another study of lansoprazole for secondary prevention of gastric or duodenal ulcers associated with long-term low-dose aspirin therapy was completed. The risk of ulcer development was significantly (log-rank test, P<0.001) lower in the lansoprazole group than in the gefarnate group, with the hazard ratio being 0.099 (95% confidence interval [CI] 0.042–0.230). They concluded that lansoprazole was superior to gefarnate in reducing the risk of gastric or duodenal ulcer recurrence in patients with a definite history of gastric or duodenal ulcers who required long-term low dose aspirin (LDA) therapy.9
There are still some controversies regarding the interaction between clopidogrel and PPI use for prevention of gastrointestinal bleeding. In general, the evidence does not suggest a clinically important interaction between PPIs and clopidogrel. However, there is a subset of patients who have reduced conversion of clopidogrel to its active metabolites due to genetic polymorphism of hepatic P-450 (carriers of CYP2C19 loss-of-function alleles). Since PPIs are also metabolized by similar hepatic enzymes, it is uncertain whether patients carrying CY2C19 loss-of-function alleles are susceptible to concomitant PPI use. In the future, management of patients on dual anti-platelet therapy needs to be individualized according to their thrombotic and bleeding risks.10
Further reading
1. Moukarbel GV, Bhatt DL. Antiplatelet Therapy and Proton Pump Inhibition Clinician Update.Circulation. 2012;125:375-380.
2. Garcia Rodriguez LA, Lin KJ, Hernandez-Diaz S, Johansson S. Risk of upper gastrointestinal bleeding with low-dose acetylsalicylic acid alone and in combination with clopidogrel and other medications. Circulation. 2011;123:1108–1115.
3. Moukarbel GV, Signorovitch JE, Pfeffer MA, McMurray JJ, White HD, Maggioni AP, Velazquez EJ, Califf RM, Scheiman JM, Solomon SD. Gastrointestinal bleeding in high risk survivors of myocardial infarction: the VALIANT Trial. Eur Heart J. 2009;30:2226–2232.
4. Juurlink DN, Gomes T, Ko DT, Szmitko PE, Austin PC, Tu JV, Henry DA, Kopp A, Mamdani MM. A population-based study of the drug interaction between proton pump inhibitors and clopidogrel. CMAJ. 2009;180:713–718.
4 Tello-Montoliu A, Charlton RK, Bass TA, Angiolillo DJ. Pharmacodynamic evaluation of pantoprazole therapy on clopidogrel effects: results of a prospective, randomized, crossover study. Circ Cardiovasc Interv. 2011;4:273–279.
6. Yasuda H, Matsuo Y, Sato Y, Ozawa S-I, Ishigooka S, Yamashita M, et al. Treatment and prevention of gastrointestinal bleeding in patients receiving antiplatelet therapy. World J Crit Care Med 2015 February 4; 4(1): 40-46.
7. Gutermann IK, Niggemeier V, Zimmerli LU, Holzer BM, Battegay E, Scharl M. and Gastrointestinal Bleeding and Anticoagulant or Antiplatelet Drugs: Systematic Search for Clinical Practice Guidelines. Medicine 2015; 94(1):e377.
8. Lai KC, Lam SK, Chu KM, Wong BCY, Hui WM, Hu WHC, et al. Lansoprazole for the prevention of recurrences of ulcer complications from long-term low-dose aspirin.N Engl J Med 2002;346:2033-8.
9. Sugano K, Matsumoto Y, Itabashi T, Abe S, Sakaki N, Ashida K, et al. Lansoprazole for secondary prevention of gastric or duodenal ulcers associated with long-term low-dose aspirin therapy: results of a prospective, multicenter, double-blind, randomized, double-dummy, active-controlled trial. J Gastroenterol 2011; 46:724–735.