BAB I BAB I Pendahuluan Pendahuluan
Pansitopenia adalah suatu keadaan dimana adanya penurunan jumlah komponen darah Pansitopenia adalah suatu keadaan dimana adanya penurunan jumlah komponen darah
yang terdiri dari 3 macam, yaitu yang terdiri dari Eritrosit (sel darah merah), Leukosit (sel darah yang terdiri dari 3 macam, yaitu yang terdiri dari Eritrosit (sel darah merah), Leukosit (sel darah
putih), dan trombosit.
putih), dan trombosit. Ketiga tersebut jika Ketiga tersebut jika mengalami penurunmengalami penurunan akan an akan mengakibatkan terjadinyamengakibatkan terjadinya
anemia, leukopenia dan trombositopenia. anemia, leukopenia dan trombositopenia.
Etiologi terjadinya pansitopenia dapat berupa primer, sekunder, dan infeksi virus. Primer Etiologi terjadinya pansitopenia dapat berupa primer, sekunder, dan infeksi virus. Primer
merupakan yang belum diketahui penyebabnya, bisa berupa idiopatik atau keturunan. Sekunder merupakan yang belum diketahui penyebabnya, bisa berupa idiopatik atau keturunan. Sekunder
yang berasal dari obat-obatan seperti NSAID, Sitotoksik, atau berdasarkan dari obat seperti yang berasal dari obat-obatan seperti NSAID, Sitotoksik, atau berdasarkan dari obat seperti
respon idiosinkrasi. Sedangkan berdasarkan dari infeksi virus yang sering menyebabkan respon idiosinkrasi. Sedangkan berdasarkan dari infeksi virus yang sering menyebabkan
terjadinya pansitopenia adalah virus hepatitis B dan C. terjadinya pansitopenia adalah virus hepatitis B dan C.
Terjadinya penurunan jumlah komponen darah tersebut dapat diketahui melalui Terjadinya penurunan jumlah komponen darah tersebut dapat diketahui melalui
pendekatan
pendekatan dari dari anamnesis, anamnesis, pemeriksaan pemeriksaan fisik fisik dan dan pemeriksaan pemeriksaan penunjang. penunjang. Pada Pada anamnesisanamnesis
biasanya
biasanya didapatkan didapatkan adanya adanya kelainan kelainan seperti seperti anemia anemia aplastic, aplastic, Sindrom Sindrom gagal gagal sumsum sumsum tulangtulang
turunan, adanya r
turunan, adanya riwayat keguguran, riwayat iwayat keguguran, riwayat menderita keganasan, adanya gangguan menderita keganasan, adanya gangguan metabolic,metabolic,
riwayat penyakit hati dan adanya riwayat penggunaan obat sitotoksik dan radioterapi. riwayat penyakit hati dan adanya riwayat penggunaan obat sitotoksik dan radioterapi.
BAB II BAB II PENDEKATAN
PENDEKATAN DIAGNOSIS DIAGNOSIS PANSITOPENIAPANSITOPENIA
Pansitopenia adalah Penurunan jumlah 3 komponen darah Eritrosit, Leukosit dan Trombosit. Pansitopenia adalah Penurunan jumlah 3 komponen darah Eritrosit, Leukosit dan Trombosit. Yang akan mengakibatkan Anemia, leukopenia, dan trombositopenia. Penyebab
Yang akan mengakibatkan Anemia, leukopenia, dan trombositopenia. Penyebab penurunan penurunan produksi
produksi darah darah di di sumsum sumsum tulangtulang,, Bone marrow faillure syndromeBone marrow faillure syndrome,, Immune mediatedImmune mediated destruction
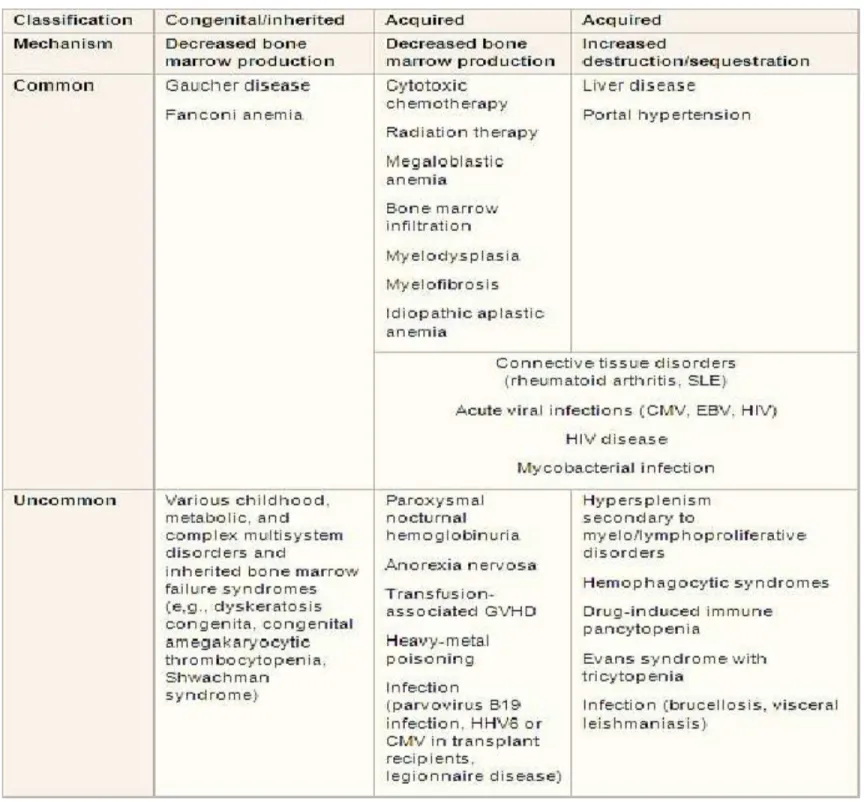
destruction,, Non immune mediated sequestration in perifer Non immune mediated sequestration in perifer.. Etiologi
Etiologi
Table of etiologies
Derajat pansitopenia
Ringan Hemoglobin <8 gr/dL, sel PMN > 2000/mm , trombosit >20.000/mm
Sedang Hemoglobin <7 gr/dL, sel PMN < 500/mm , trombosit <20.000/mm
Pendekatan Diagnosis Anamnesis
• Anemia aplastik
• Sindrom gagal sumsum tulang turunan • Riwayat keguguran
• Riwayat menderita keganasan • Gangguan metabolik
• Riwayat penyakit hati
• Riwayat penggunaan obat sitotoksik dan radio terapi Pemeriksaan fisik
Mata :
• Perdarahan retina (trombositopenia) • Infiltrasi lekemik (leukimia akut)
• Sklera ikhterik (Paroxysmal nocturna hemoglobinuria, hepatitis, sirosis) • Epiphora (dyskeratosis congenital)
Oral :
• Ptekie/ Perdarahan di rongga mulut (trombositopenia) • Stomatitis/chelitis (neutropenia, def. Vit B12)
• Hiperplasia gusi (leukimia )
• Kandidiasis oral/ eksudat faring (neutropenia, infeksi herpes virus) Kardiovaskular:
• Takikardi, edema, CHF
• Bekas pembedahan jantung (sindrom kongenital) Respiratori :
• Clubbing (ca. paru) • Takipnea
Abdomen :
• Nyeri perut kakan atas ( hepatitis )
• Limfadenopati (infeksi, penyakit limfoproliferatif, HIV) • Tanda penyakit hati kronis
• Splenomegali (infeksi, penyakit myeloproliferatif, limfoproliferatif) Kulit :
• Malar rash (SLE)
• Purpura (trombositopenia)
• Pigmentasi retikular, kuku displastik (dyskeratosis congenital) • Area hipopigmentasi
• Hiperpigmentasi, café au lait (anemia fanconi Muskuloskeletal :
• Short stature ( fanconi anemia, kelainan congenital lain) • Artritis, sinovitis (SLE)
• Jari-jari abnormal (anemia fanconi) Tanda yang berhubungan dengan infeksi HIV :
Morbiliform rash
LABORATORIUM Pemeriksaan standar
Hitung darah lengkap Apusan darah tepi Hitung retikulosit darah
Fungsi hati dan serologi hepatitis
Tes koagulasi, bleeding time, fibrinogen, D-dimer Tes direct antiglobulin
Serum B12 dan folat Seru HIV
TES anti nucleid acid Biopsi Sumsum Tulang Selularitas:
↓: gangguan produksi darah: pasca kemoterapi, sepsis/infeksi akut, HIV Stadium lanjut, syndrom myelodisplasi hipoplastik , IBMFS ,anemia aplastik idiopatik,SLE, PNH
N/↑: produksi yang tidak efektif/↑destruksi/sekuestrasi sel-sel darah: myelodisplasia, leukimia akut/kronik,myeloma dengan plasma selnya, infiltrasi keganasan, HIV stadium dini/akut, anemia megaloblastik.
Histologi :
Infiltrasi sel Blast
Gambaran myelodispplasia
Aspirasi Sumsum Tulang
Sitologi (perubahan megaloblastik, perubahan displastik, infiltrasi sel abnormal dan infeksi)
Imunofenotif (leukimia akut dan kronik, penyakit limfoproliferatif)
Temuan laboratorium Common
Differential 1 st test Other test
Chemotherapy • peripheral blood: anisocytosis, poikilocytosis, basophilic
stippling
• bone marrow aspirate: variable hypoplasia
• bone marrow
biopsy:hypoplasia, megaloblastosis
Radiotherapy • peripheral blood: anisocytosis, poikilocytosis, basophilic
stippling
• bone marrow aspirate: variable hypoplasia • bone marrow biopsy:hypoplasia, megaloblastosis Vitamin B12 deficiency
• peripheral blood film: oval macrocytic RBCs, irregular size and shape of RBCs (anisocytosis
and poikilocytosis),
hypersegmented granulocytes (>5 lobes)
• serum reticulocyte
count: usually low
• serum B12: low in B12 deficiency
• bone marrow
megaloblastic erythroblasts, giant metamyelocytes
• serum LDH: moderately raised • serum bilirubin:moderately
raised, mostly indirect
Folic acid deficiency
• peripheral blood film: oval macrocytic RBCs, irregular size and shape of RBCs (anisocytosis and poikilocytosis), hypersegmented granulocytes (>5 lobes)
• serum reticulocyte
count: usually low
• serum RBC folate: low in folate deficiency
• bone marrow
aspirate: hypercellular,
megaloblastic erythroblasts, giant metamyelocytes
• serum LDH: moderately raised • serum bilirubin:moderately
raised, mostly indirect Bone marrow
infiltration by nonhematologic malignancy
• peripheral blood film: leuko-erythroblastic cell forms
• bone marrow aspirate: clumps of tumor cells
• CXR:mass (lung cancer)
CT of abdomen: may reveal abdominal or renal mass
serum prostatic-specific antigen: elevated in prostate cancer
• serum LFTs: elevated ALT and AST ( hepatic metastases)
• serum coagulation
profile: prolonged PT and PTT
• serum fibrinogen and D -dimer: diminished fibrinogen and elevated D-dimer (indicative of chronic disseminated intravascular coagulation)
thyroid ultrasound: irregular mass or nodule
breast imaging: mass or calcifications
Non-Hodgkin lymphoma
• peripheral blood film: variable; may show circulating lymphoma cells
• bone marrow aspirate: increased proportion of lymphoid cells
• immunophenotyping (of peripheral blood or bone marrow):clonal population of lymphoid cells
• lymph node
biopsy:lymphoproliferative disorder
Hepatitis C • peripheral blood
film:macrocytes, target cells, stomatocytes, acanthocytes
• reticulocyte count: elevated or normal
• serum LFTs: elevated
• serum antihepatitis C virus (HCV): presence of HCV antibodies
• bone marrow
aspirate: hypercellular, erythroid hyperplasia
Autoimmune hepatitis
• peripheral blood
film:macrocytes, target cells, stomatocytes, acanthocytes
• reticulocyte count: elevated or normal
• serum LFTs: elevated
• autoantibody screen: positive
• bone marrow
aspirate: hypercellular, erythroid hyperplasia
HIV • peripheral blood film: atypical
lymphocytes (acute
seroconversion), rouleaux, dysplastic neutrophils
• reticulocyte count: reduced • HIV serology: positive
• bone marrow
aspirate: hypercellular (acute seroconversion), hypocellular, dyserythropoiesis • protein electrophoresis: polycl onal hypergammaglobulinem ia
Hepatitis B • peripheral blood
film:macrocytes, target cells, stomatocytes, acanthocytes
• reticulocyte count: elevated or normal
• serum LFTs: elevated • serum HBsAg: positive
• bone marrow aspirate: hypercellular, erythroid hyperplasia Hairy cell leukemia • peripheral blood
film:circulating lymphoma cells
• bone marrow aspirate: increased proportion of lymphoid cells
• immunophenotyping (of peripheral blood or bone marrow):clonal population of
lymphoid cells
Chronic lymphocytic leukemia
• peripheral blood
film:circulating leukemia cells cells
• bone marrow aspirate: increased proportion of lymphoid cells
• immunophenotyping (of peripheral blood or bone marrow):clonal population of lymphoid cells
• lymph node
biopsy: lymphoprolifera tive disorder
Myelodysplasia • peripheral blood film: may have irregular or macrocytic RBCs, dysplastic granulocytes, platelets may be large and hypogranular
• serum reticulocyte
count: usually low, may be normal or raised
• bone marrow aspirate: usually hypercellular, rarely, hypocellular (hypocellular myelodysplasia), dysplastic changes
• cytogenetics: may be abnormal
Cirrhosis • peripheral blood
film:macrocytes, target cells, stomatocytes, acanthocytes
• reticulocyte count: elevated or
• bone marrow
aspirate: hypercellular, erythroid hyperplasia
normal
• serum LFTs: elevated
Cytomegalovirus infection
• peripheral blood film: atypical lymphocytes, spherocytes if coexisting hemolysis
• CMV-specific IgM and IgG: positive
• bone marrow
aspirate: cellularity usually increased, hemophagocytosis may be prominent
• bone marrow trephine biopsy:cellularity usually increased
Mycobacterial infection
• peripheral blood film: rouleaux • reticulocyte count: reduced
• bone marrow aspirate: reduced cellularity, hemophagocytosis
• bone marrow trephine biopsy:reduced cellularity, granulomas, fibrosis
• bone marrow culture: positive for organism
Differential 1st test Other test Acute myeloid
leukemia
• peripheral blood film: blasts on blood film, presence of Auer rods
• serum PT, PTT, fibrinogen, D -dimer: may be abnormal, suspect DIC • bone marrow aspiration: usually
hypercellular with blasts, rarely hypocellular
• bone marrow biopsy: presence of blasts, infiltration, Auer rods
• immunophenotyping: detection of clonal population of blasts
• cytogenetics: identification or nonrandom chromosomal abnormalities • serum PT, PTT, fibrinogen, D -dimer: prolonged PT, PTT; diminished fibrinogen, elevated D-dimer
Acute
lymphocytic leukemia
• peripheral blood film: blasts may or may not be present
• bone marrow aspirate: hypercellular with blasts; occasionally hypocellular (childhood ALL)
immunophenotyping (of peripheral blood or bone marrow): detection of clonal population of blasts cytogenetics: identificatio n of nonrandom chromosomal
Multiple myeloma
• peripheral blood film: rouleaux, circulating plasma cells may rarely be present
• bone marrow aspirate: plasma cell infiltrate, abnormal plasma cells, plasmablasts
• immunophenotyping (of peripheral blood or bone marrow): plasma cells exhibit restriction of kappa or lambda light chain expression
• serum and urine
electrophoresis:monoclonal serum protein and urinary Bence-Jones proteins (light chains) detected
• radiologic skeletal survey: lytic lesions and/or osteopenia
Myelofibrosis • peripheral blood film: leuko-erythroblastic, tear drop RBCs
• bone marrow aspirate: hypercellular and fibrotic, often dry tap and nondiagnostic • serum and RBC folate: usually diminished • serum B12: usually elevated Lysosomal storage disorders • leukocyte glucocerebroside activity:reduced or absent
• peripheral blood film: pancytopenia • reticulocyte count: may be high,
normal, or reduced
• bone marrow aspirate: may reveal Gaucher cells
• bleeding
Anorexia nervosa
• peripheral blood film: red cell acanthocytes, poikilocytosis and basophilic stippling
• reticulocyte count: low
• bone marrow aspirate: hypocellular, reduced hematopoietic cells, may show gelatinous transformation
• bone marrow trephine
biopsy: hypocellular without infiltration or fibrosis
• diepoxybutane test: normal
Graft-versus-host disease
• peripheral blood film: no specific features
• reticulocyte count: low
• bone marrow aspirate: hypocellular, reduced hematopoietic cells, increased macrophages, erythrophagocytosis
• bone marrow trephine
biopsy: hypocellular without infiltration or fibrosis, increased macrophages
• skin, liver, upper GI
biopsy: characteristic appearances of acute GVHD
• HLA typing of peripheral blood
Heavy metal (arsenic)
poisoning
• peripheral blood film: basophilic stippling
• bone marrow aspirate: hypocellular without infiltrate or fibrosis, decreased hematopoietic cells, dyserythropoiesis
• bone marrow trephine
biopsy: hypocellular without infiltration or fibrosis dyserythropoiesis
• diepoxybutane test: normal
• screening for PNH clone: negative • arsenic level (serum, urine, hair,
nails):elevated Parvovirus infection in sickle cell anemia • CBC: drop in hemoglobin concentration of >30 percent secondary to complete arrest of erythropoiesis
• reticulocyte count: decrease or absence of measurable reticulocytes
• bone marrow biopsy: remarkable for severe aplasia
Dyskeratosis congenita
• peripheral blood film: red cells usually macrocytic
• reticulocyte count: low or absent
• bone marrow aspirate: hypocellular, reduced hematopoietic cells, dyserythropoiesis common
• bone marrow trephine
biopsy: hypocellular without infiltration or fibrosis
• diepoxybutane test: normal (peripheral blood lymphocytes)
• screening for PNH clone: may be present
• peripheral blood and/or bone marrow
immunophenotyping: normal
• blood and/or bone marrow cytogenetics:clonal abnormalities present in some patients
• genetic studies: may identify 1 of several genetic mutations • telomere length: abnormally short; length in lymphocytes and granulocytes <1 percentile for age
Paroxysmal nocturnal hemoglobinuri a
• peripheral blood film: polychromasia • reticulocyte count: relative
reticulocytosis
• bone marrow aspirate: hypocellular, reduced hematopoietic cells, mast cells may be increased
• diepoxybutane test: normal
• screening for PNH clone: positive
Idiopathic aplastic anemia
• peripheral blood film: normocytic or mildly macrocytic RBCs, no immature precursors present
• serum reticulocyte count: low or absent
• bone marrow aspirate: hypocellular, mild dyserythropoiesis common
• bone marrow trephine
biopsy: hypocellular without fibrosis or infiltrate
• diepoxybutane test (peripheral blood lymphocytes): normal
• screening for paroxysmal nocturnal hemoglobinuria clone (peripheral blood, bone marrow): detectable in up to 30% of patients
• peripheral blood, bone marrow immunophenotyping: normal
• peripheral blood, bone marrow cytogenetics: abnormal clones present in a minority of patients
Fanconi anemia
• peripheral blood film: RBCs usually macrocytic
• reticulocyte count: low or absent
• bone marrow aspirate: hypocellular dyserythropoiesis
• diepoxybutane test (peripheral blood lymphocytes): increased chromosomal breakage
Idiopathic portal
hypertension
• peripheral blood film: no specific features
• reticulocyte count: elevated or normal • serum LFTs: normal or mildly
elevated • bone marrow aspirate: hypercellular , erythroid hyperplasia • bone marrow trephine biopsy:hypercellular, erythroid hyperplasia Chronic myeloid leukemia
• peripheral blood film: myeloid maturing cells, elevated basophils, eosinophils
• cytogenetics: Philadelphia chromosome positive
• bone marrow biopsy: granulocytic hyperplasia
Brucellosis • peripheral blood film: no specific features
• bone marrow aspirate: trilineage hypercellularity, hematophagocytosis • blood and bone marrow
cultures: positive for organism
Leishmaniasis • peripheral blood film: rouleaux; organisms rarely seen in peripheral blood film
• bone marrow aspirate: trilineage hypercellularity; organisms may be seen within macrophages (Leishman -Donovan bodies)
• bone marrow trephine
biopsy: trilineage hypercellularity,
hematophagocytosis, small
• immunochromatographic or PCR -based tests on peripheral blood or bone marrow aspirate: positive for organism
Hemophagocy tosis
syndromes
• peripheral blood film: no specific
features
• bone marrow aspirate: trilineage
hypercellularity, hematophagocytosis
• blood and bone marrow cultures: positive for organism
autoimmune
screen: positive ANA and anti-ds DNA
serum ferritin: >10,000 mcg/L
molecular genetic testing: specific karyotype present
Drug-induced immune pancytopenia
• platelet-specific antibodies: positive • peripheral blood film: no specific
features
• reticulocyte count: elevated
• bone marrow aspirate: hypercellular • bone marrow trephine
biopsy: hypercellular Evans syndrome with associated neutropenia
• peripheral blood film: polychromasia,
spherocytes
• reticulocyte count: elevated • direct antiglobulin test: positive
antibodies: positive
• bone marrow aspirate: normal or trilineage hypercellularity
• bone marrow trephine
biopsy: normal or trilineage hypercellularity
Systemic lupus
erythematosus
• peripheral blood film: rouleaux
• autoimmune screen: positive ANA and anti-DNA
• ultrasound of the
abdomen: splenomegaly
• bone marrow aspirate: hypocellular, Adysplastic changes, hematophagocytosis
• bone marrow trephine
biopsy: hypocellular, benign lymphoid aggregates
Rheumatoid arthritis
• peripheral blood film: rouleaux
• autoimmune screen: positive rheumatoid factor
• bone marrow aspirate: hypocellular, dysplastic changes, hematophagocytosis
• bone marrow trephine
biopsy: hypocellular, benign lymphoid aggregates
• ultrasound of the
Infectious mononucleosi s
• serum monospot: positive
• peripheral blood film: atypical
lymphocytes
• Epstein-Barr nuclear
antibody: present
• blood serology (specific IgM and IgG
titers) for viral capsid
antigen: positive Felty
syndrome
• bone marrow biopsy: myeloid
hyperplasia with excess of immature forms
• autoimmune screen: positive
rheumatoid factor
• ultrasound of the
BAB III Kesimpulan
Pansitopenia bukanlah suatu gejala melainkan suatu triad yang di sebabkan suatu proses penyakit yang melibatkan sumsum tulang baik primer maupun sekunder. Pansitopenia adalah masalah sering di temui dalam praktek sehari-hari. Untuk menegakan diagnosis pati perlu di lakukan pemeriksaan yang lebih spesifik.
Tinjauan Pustaka
1. Evaluation of pancytopenia Diagnostic approach-Eppocrates online hhtps://online.epocrates.com/u/29211024/evaluation+of+pancytopenia. 2. Makalah lengkap Bandung hematologi oncology meeting 2013, page 7-15