THE RECONSTRUCTION OF THE GLOBE PROLAPSE IN ORBITAL TRAUMA
Shanti BOESOIRIE, Lakshmi Thaufiq
Cicendo Eye Hospital/Padjdajran University Bandung
Objective : To report a reconstruction of the globe prolapse caused by superior orbital bone fracture.
Case Report : A patient with globe prolapse due to orbital trauma were reported. The bone fragment of superior orbital bone pushed the globe anteriorly. This case is one of the emergency case in ophthalmology to preserved the function of the eye. The bone fragment was repositioned and fixated using screw and miniplate.
Conclusion : A good management and an immeduate reconstruction gave a good result in an orbital trauma
Orbital trauma can damage the facial bones and adjacent soft tissues. Orbital fractures may be associated with injuries to orbital contents, intracranial structures, nasal and paranasal sinuses. Orbital hemorrhage and embedded foreign bodies may also be present and have secondary effects upon the orbital soft tissues. Intraocular injuries, decrease visual acuity, strabismus, and ptosis may occur.1
Because of the high incidence of concomitant intraocular injury, an ocular examination must always be performed on patients who have sustained orbital trauma. Ocular damage accompanying orbital trauma may include hyphema, cornea scleral laceration, retinal tear, vitreous hemorrhage, and can caused displacement of the globe.1
Orbital roof fractures are usually caused by blunt trauma and are more common in young children. Frontal trauma in older patients tends to be absorbed by the frontal sinus. which act as a crumple zone. The entrapment of extraocular muscles is extremely rare, but development of a subperiosteal hematoma and secondary mass effect impinging on the superior rectus is not uncommon. The bone fragment and hematoma can push the globe anteriorly. In severely communited fractures, pulsating exophthalmos may occur as a delayed complication.1
The most common clinical findings in a patients with a supraorbital fractures is periorbital edema and ecchymosis. There is oftern a forehead or brow laceration present. Periorbital and in particular, upper eyelid hematoma is seen frequently, and this may be a delayed onset hematoma, seen several hours after injury.2
The CT scan has become the standard of care for evaluating supraorbital trauma. Axial and coronal views should be obtained to evaluate optimally the extent of injury. High definition 3-dimensional Ct Scans can serve as an elegant teaching tool and can be helpful in complex injuries.2
The orbit’s primary role is to protect the eyeball. The basic principles of primary repair in orbital trauma are explore the injury, remove foreign material, conserve as much tissue as possible, debride only that tissue which is frankly necrotic and non viable, approximate the normal sclerocorneal anatomy, give adequate endophthalmitis prohylaxis3,4
laceration around the face and orbit should be cleansed and properly sutured as early as possible to minimize the possibility of infection and scarring.5
The most common indications for surgical intervention are as follows: 1. Displacement of bone fragments disfiguring the normal facial contours
2. Interference with normal binocular single vision caused by extraocular muscle entrapment
3. Obstruction of the nasolacrimal duct.5
Following supraorbital fracture, the patients is usually admitted to neurosurgical service because of accompanying intracranial injury. Lacerations of the brow and upper eyelid often accompany with fractures of the superior orbital margin, which anatomically protects the eye superiorly.5
Supraorbital fractures may be arbitrarily subdivided into two types. The first types, a Chip fracture of the supraorbital rim, may occur without involving the inner table. (Figure 1-A). This type of fracture most often occurs when a blunt or sharp instrument such a hammer hits the rim from above in a downward direction. The second type of supraorbital fracture involves the orbital rim and roof (figure 1.B). The blow producing this type of fracture is usually more direct than the blow that cause the chip fracture.5
Figure 1 A. Chip fracture, B. Supraorbital fracture involves orbital rim5
Figure 2. Patients with supraorbital chip fragment
reduction may be all that is indicated. If associated with a laceration, the fracture
fragment may be reduced through the laceration and sutured or wired in place before the wound is closed.5
Figure 3. Management of supraorbital fracture
Above is one of a management of supraorbital fracture associated with globe prolapse. The approach done through the laceration, and find the bone fracture and fragment and reposition the bone fragment with miniplate and screw.
Figure 4. Patient after surgery
Conclusion : A good management and an immeduate reconstruction gave a good result in an orbital trauma
Reference:
1. American Academy of Ophthalmology. Orbit, Eye Lid and Lacrimal system, Basic and Clinical Science course, section 7. American Academy of
2. Hardy SP, Morales L. Orbital roof and supraorbital ridge fractures. In. Evaluation and treatment of orbital fractures. Pennsylvania; Saunders Elsevier. 2006. p. 193-9
3. Foss. AJE. Essential ophthalmic surgery. Oxford . Buuterworth-Heinemann. 2001. p. 301-303
4. Long JA, Tann TM. Orbital trauma. In. Ocular Trauma. Kunn F, Pieramici DJ. Ed. New York; Thieme. 2002.p.383-90
FRONTAL SLING AND Y TO V PLASTY FOR BLEPHAROPHYMOSIS SYNDROME RECONSTRUCTION
Shanti BOESOIRIE, Lakshmi Thaufiq
Cicendo Eye Hospital/Padjdajran University Bandung
Objective: To report the succesful of a reconstruction using frontal sling and Y to V plasty technique in patients with Blepharophymosis syndrome
Case report: . Blepharophymosis syndrome has been known as a hereditary anomaly. The symptoms were ptosis, epicanthus inversus, and telecanthus. The successful reconstruction using frontal sling with mersilene mesh and Y to V plasty technique to repair ptosis, epicanthus inversus, and telecanthus in Blepharophymosis Syndrome were reported. There were 17 patients underwent this procedure with good result. .
Conclusion: A reconstruction surgery using frontal sling and Y to V plasty gave good result in Blepharophymosis Syndrome.
Blepharophimosis syndrome is an autosomal dominant–inherited anomaly. Patients with this syndrome presenting bilateral severe ptosis (usually with no levator function), epicanthus inversus, and ectropion of the lateral portions of the lower lids.1
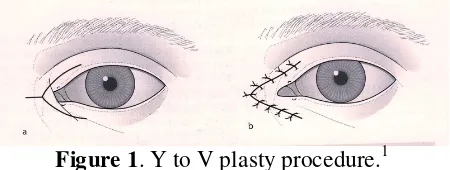
A horizontal Y-shaped is made over the medial canthal tendon which can be shortened to correct any telecanthus.
Figure 1. Y to V plasty procedure.1
1. Mark a Y on the medial canthal skin with the base of the stem in the desired new position of the medial canthus
2. Undermined
3. Excise excess skin and subcutaneous tissue
4. Use buried 6’0 long acting absorbable sutures to fix the subcutaneous tissues to the medial canthal tendon. Close the skin as a V with fine absorbable sutures which can be removed in as adult.1
Treatment of the ptosis depends on the levator muscle function. In blepharophimosis bilateral brow suspension or frontalis sling procedure is needed, and the epichantus corrected using Y to V plasty.1,2,3
Evaluation of the ptosis depends on the measurement of:
The indication for frontalis sling procedure is a ptosis with less than 4 mm of levator function The frontalis muscle normally lifts the eyebrow and contributes to eyelid elevation. This action of lifting the eyelid is enhanced by connecting the frontalis muscle and eyebrow to the eyelid with a subcutaneous sling for which various material can be used. There are some materials that can be use as a sling in frontalis sling :
- autogenous : fascia lata, temporalis fascia
- nonautogenus : - integrateable e.g mersilene mesh. Gortex - nonintegrateable e.g supramid, prolene suture, silicone rod 1,4
Figure 2. Mersilene mesh using modification of the Wright needle
Autogenous fascia lata is the best material for a sling but needs to be harvested, which limits its use in very young children and in the old. There is little risk of infection, absorption and breakage such as occur with foreign materials. An integrateable material such as a 3 mm strip of Mersilene mesh is valuable for a more permanent ptosis correction, cheap and easy to get.1
The author technique of frontal sling is a midified of Crawdord and fox pentagon Technique. The procedure is as follow :
Figure 3. Frontal sling procedure
Frontal Sling Procedure :
the mark must be raised, but this will reduce the sling’s mechanical advantage in raising the lid. Make three marks just above the eyebrow , one vertically above and a little medial to the medial eye mark.
2. Make a stab incision through all the marks, widening the three forehead incisions a little.
3. Use a modification of Wright’s facial needle to pass each strip of mersilene mesh as shown in the picture above.
4. Pull up the strip of mersilene mesh to give a symmetrical lid curve. 5. Tie the strip together, and reinforce the knot with a 6’0 absorbable suture 6. Close the incisions with 6’0’ nylon or silk sutures.
7. Make a frost suture to lift the lower lid up and taped it on the forehead for 48 hours postoperatively
8. Use lubricant and antibiotic ointment
Figure 4. Patients before and after frontal sling and Y to V plasty
Conclusions : A reconstruction surgery using frontal sling and Y to V plasty gave good result in Blepharophymosis Syndrome.
Reference:
1. Collin JRO, A Manual of Systemic Eyelid Surgery. 3RD edition. Churchill Livingstone, Edinburgh, 2006. p. 85-113, 155-156
2. American Academy of Ophthalmology. Orbit, Eye Lid and Lacrimal system,
Basic and Clinical Science course, section 7. American Academy of
3. Bashour M. Blepharoplasty, ptosis surgery. E medicine 2005. Available from :
http://www.emedicine.com/ent/topic97.htm