A brief description of the background that led to the study (current results and conclusions should not be included). Individuals who directly participated in the creation of the manuscript but are not involved in the authorship may be acknowledged.
Discussion
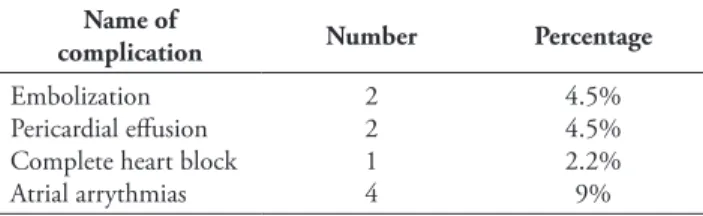
There is no incidence of erosion or air embolism in our study.. less than half of systemic arterial pressure). There was one occurrence of complete heart block in our study, but rhythm returned to sinus after four minutes. The risk of bundle branch block in patients with large ASD, especially patients with rim defects, may be increased. A retrospective study of six hundred and ten device closure patients showed that clinically significant AV block occurs in 0.3% of patients.10.
In our study, we did not experience any cases of erosion at one year follow-up, although many of our patients had very large devices with inadequate retro-lips of the aorta. Two cases of atrial fibrillation and two cases of atrial fibrillation were seen in our study. FDA analysis of MAUDE medical device reports (MDR) showed a 0.8% incidence of infection or endocarditis.14 There were no cases of nitinol allergy, infection, or hemoglobinuria in our patients who closed the device.
Conclusion
We succeeded in all cases except one where we had to come from the right superior pulmonary vein. In the BAT technique, the inflated Tyshac balloon can be placed in either the contralateral pulmonary vein or the ipsilateral pulmonary vein, which will prevent prolapse of the left atrial disc into the right atrium. A few of them are even kept in the left atrium itself to prevent prolapse of the left atrial disc. (14) The Greek maneuver is applied when there is protrusion of the left atrial disc into the right atrium from the bottom of the aorta.
Then the left atrial disk and the 2/3 of the right atrial disk are simultaneously released into the left atrium and positioned appropriately. The left atrial disc becomes parallel to the septum, preventing protrusion of the device into the right atrium.15 We did not use any maneuver for device placement. Our conclusion is the key to success: the correct sizing of the defect and the rims by TEE.
Limitations
These may be due to guidewire, sheath, or device-induced irritation of the atrial wall. There is concern that closure of ASD could preclude future electrophysiological procedures requiring transseptal access.13. In the setting of a very large ASD, it is difficult to maintain the posterior orientation of the LA disc.
Often the LA disc tilts tangentially across the defect and prolapses back into the RA. There are mainly two maneuvers that enable successful placement of the device a) BAT (balloon-assisted technique) b) Greek maneuver. To avoid this, the left disc is recaptured and the entire delivery system is pushed inward and left into the left atrium.
Financial disclosure
Balloon size has been used by many operators in these cases, but we have never used it.
Conflict of interest
Morphologic variations of secundum-type atrial septal defects: feasibility of percutaneous closure using Amplatzer septal occluders. Early and late complications associated with transcatheter occlusion of secundum atrial septal defect Journal of American College of Cardiology. Food and Drug Administration Manufacturer and user facility device experience database for adverse events involving Amplatzer septal occluder devices and comparison with the Society of Thoracic Surgery congenital heart surgery database.
Electrocardiographic changes and arrhythmias after percutaneous atrial septal defect and patent closure of the foramen ovale apparatus. Transcatheter closure of large secundum atrial septal defects using the 40 mm Amplatzer septal occluder: results from an international registry. Thanopoulos BD, Dardas P, Ninios V, Nicholaos Eleftherakis N, Evangelos Karanasios E. Transcatheter closure of large atrial septal defects with defective aortic or posterior margins using the "Greek maneuver".
Correlation Of Left Ventricular Ejection Fraction and Spatial Qrs-T Angle In Old Myocardial Infarct Patient
Introdution
42, Issue II ● April - June 2021 43 LVEF and QRS-T wave spatial angle using Pearson correlation analysis if the data were linear or using Spearman correlation if the data were non-linear.
Results
This finding is consistent with previous studies that the larger the LVMI is, the wider the spatial angle will be. This result shows that after adjusting the LVMI, the correlation with spatial angle is moderated, indicating the contribution of LVMI to the correlation between spatial angles and LVEF. The correlation between sQRST angle and LVEF is not perfect, meaning that not all patients with LVEF ≤35% have high spatial angles.
Based on these findings, the spatial angle of the QRS-T wave can identify patients with a low risk of developing arrhythmias so that it can complement LVEF in SCD risk stratification. This study also cannot exclude left ventricular hypertrophy by LVMI criteria in order to influence the relationship between sQRST angle and LVEF. In conclusion, there is a moderate negative correlation between QRS-T wave spatial angle and LVEF in patients with OMI after multivariate analysis with LVMI.
Publication Approval
The Cortez study had similar baseline sample characteristics with a mean age of years and 72% male gender. The difference was that the patient in Cortez's study had a recent myocardial infarction, but the average onset of the attacks that occurred was not mentioned. In this study 50% of patients had an attack onset of 5 months, while the other 50% had no information about the onset of previous attacks, however this indicates a longer mean time after attack in this study.5 Together with the continuous remodeling process, the sQRST angle will also widen.12.
This study has several limitations that include echocardiography and sQRST angle was only performed by one operator so interobserver variability could not be assessed. Increase in the sQRST angle can be used as an indicator of a decrease in LVEF in patients with OMI.
Conflict of Interest
Sources of funding
Ethical Clearance
Copyright/Permission for Figures
List of Abbreviations
Emerging Role of Coronary CT in Non-ST Elevation Acute Coronary Syndrome (NSTE-ACS)
Introduction
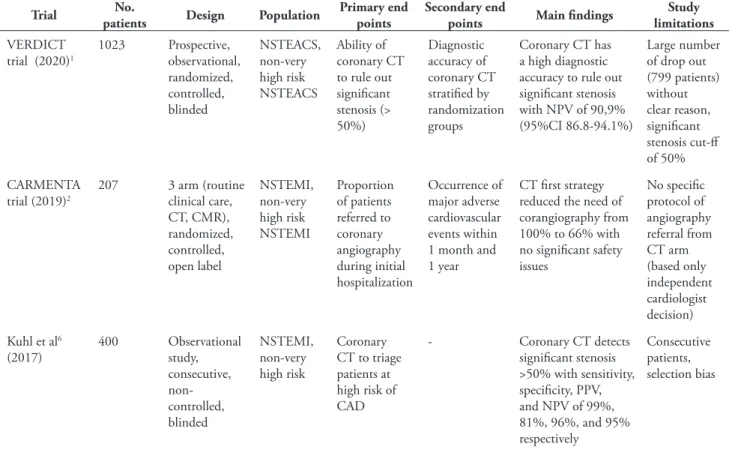
At least three studies have been published to date regarding the role of coronary CT in NSTEACS: CARMENTA, VERDICT study, and Kuhl et al. CARMENTA study was a three-arm, prospective, open-label, single-center, randomized, controlled, comparative study using CMR and coronary CT as a gatekeeper for coronary angiography in patients with NSTEACS. The study also found that coronary CT patients were correctly classified as PCI or CABG in 86% of cases.
Despite some limitations, the findings from the 3 studies indicated that there may be a role for coronary CT in NSTEACS. The present study showed that coronary CT can be useful in diagnosing significant coronary disease in NSTEACS and appears to be safe to obtain. Several studies such as the FFR-CT and CT-NSTEMI trials are being conducted regarding its issues and may provide a better understanding of the role of coronary CT in NSTEACS.
Heart Failure with Preserved Ejection Fraction (HFpEF): A Case Report
Background
Case Illustrations 1
Based on history, physical examination, and supportive examination, the patient was diagnosed with acute decompensated heart failure in HFpEF due to hypertensive heart disease with hyperglycemia, stage 1 hypertension, and renal insufficiency. The patient was initially treated with furosemide 20 mg iv, continued with 2 x 40 mg iv, ramipril 1 x 2.5 mg and insulin drip 2 units/hour. Furosemide was titrated to oral 1x40 mg, ramipril was increased to 1x10 mg and bisoprolol was started at 1x1.25 mg.
The patient was trained to limit fluid intake up to 1500 ml/day and to return for follow-up at the outpatient clinic one week later. The patient was initially treated with furosemide 20 mg IV and continued with 2x40 mg IV, ramipril 1x2.5 mg and insulin drip 2 units/hour. The patient was trained to limit fluid intake up to 1500 ml/day and to return for follow-up at the outpatient clinic one week later.
Case Illustrations 2
Based on the history taking, physical examination, and supportive examination, the patient was diagnosed with acute decompensated heart failure in HFpEF due to hypertensive heart disease, hypertension with controlled blood pressure, hypokalemia, and obesity. In 2019, the Heart Failure Association of the European Society of Cardiology (HFA ESC) published the HFA-PEFF algorithm for diagnosing HFpEF. Heart failure was treated with ACE inhibitors, beta blockers and diuretics according to ESC recommendations.
Several studies have been conducted to investigate effective treatments in reducing mortality and hospitalizations due to heart failure in HFpEF. 42, Issue II ● April - June 2021 57 with preserved ejection fraction: The HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Novel strategies for heart failure with preserved ejection fraction: the importance of targeted therapies for heart failure phenotypes.
The de Winter Pattern as Pre-Anterior ST-Elevation-Myocardial-Infarction
An Evolution Sequence”: A Case Report
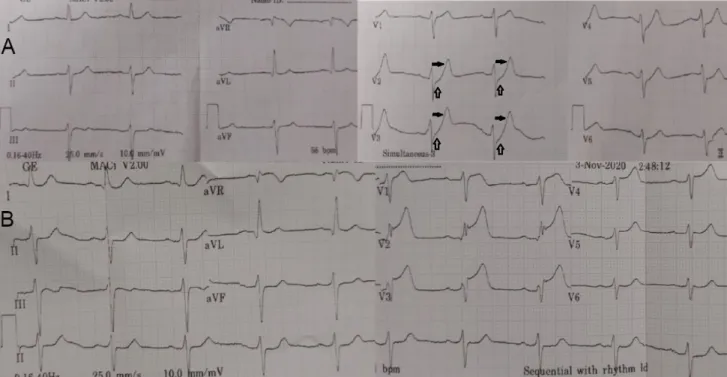
Acute myocardial ischemia caused by coronary artery occlusion causes electrophysiological changes in the cardiac cell that result in a characteristic pattern on the surface electrocardiogram (ECG). The de Winter pattern (dWP) was first described by de Winter et al in 2008 as a static ECG pattern associated with anterior myocardial infarction associated with left anterior descending artery (LAD) occlusion.1 ECG features including ST segment elevation depression at J point in the precordial leads followed by a prominent positive symmetric T wave, other additional features including mild ST segment elevation in aVR and loss of precordial R wave progression.1. The prevalence of this pattern was 2% in a patient with anterior myocardial infarction with significant myocardial loss despite a successful reperfusion procedure.1-4 The mechanism of this ECG pattern was still unclear and the first report stated that the ECG pattern was static, but later reports .
In this paper, we discuss the case of a 56-year-old man with a dWP ECG at first medical contact followed by a typical anterior STEMI pattern with review of the mechanism.
Case Illustrations
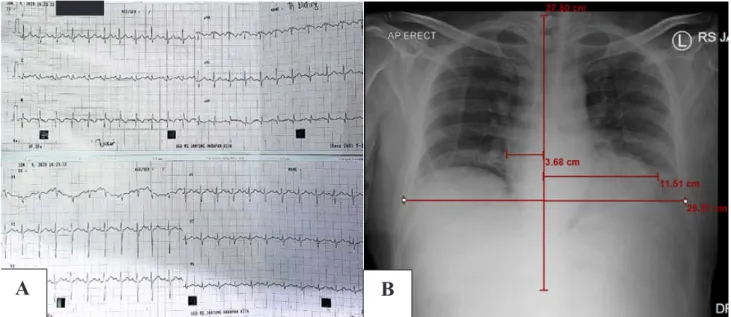
Point-of-care ultrasound showed regional wall motion abnormalities in the septal and anterior segments. The ECG 1 hour after thrombolytic therapy showed typical ST-segment elevation in the precordial area with marked loss of R-wave progression (Figure 2). The ECG was obtained an average of 1.5 hours from baseline.1 The ECG pattern continued from the baseline ECG to the pre-procedural ECG.
The mechanism of ST-segment depression in dWP would be related to the negative voltage difference between ischemic subendocardial and normal subepicardial action potentials during the plateau phase (phase 2 AP) caused by subendocardial ischemia; this negative voltage difference is based on the theory of TAP summation causing ST depression on the surface ECG. In this case presentation, we have shown dWP evolving into a typical anterior STEMI. A serial ECG is mandatory to show the development of dWP and, most importantly, to recognize this pattern in the "first look" ECG to avoid delay in treatment and induce early reperfusion and better myocardial salvage, as anterior STEMI has a poor short- and long-term outcome .