The final book to complete the series will focus on emergency procedures in interventional radiology. These technique-specific books will benefit those residents and fellows training in interventional radiology who may be taking subspecialty certification exams in interventional radiology.
Aneurysm Treatment
Intracranial Embolization
Spinal Embolization
Intra-arterial Therapy in Acute Ischaemic Stroke
Angioplasty and Stenting of Arterial Stenosis
Venous Procedures
Interventional Neuro-Oncology Percutaneous Treatment of Venolymphatic
Spine Intervention
Series Editors
Volume Editors
Roberto Izzo, MD Department of Neuroradiology, AORN Cardarelli, Napoli, Italien Sudhir Kathuria, MD Division of Interventional Neuroradiology,. Mario Muto , MD Department of Neuroradiology , AORN Cardarelli , Napoli , Italien Peter Kim Nelson , MD Department of Radiologi og Neurokirurgi.
Abstract
Keywords
Diagnostic Evaluation
Indications for Performing a Diagnostic Cerebral Angiogram
Patient Preparation
Relevant Aberrant Anatomy
Preprocedure Medications
When manual compression is used, non-occlusive pressure should be applied to the arteriotomy puncture site for at least 10 minutes after the procedure. Follow-up should be planned before discharge and is essential to ensure the patient's long-term well-being.
Key Points
Suggested Reading
Introduction
Venous drainage is through a plexus of epidural veins that freely anastomoses with a plexus of paravertebral veins.
The combination of umbilical cord edema, mild swelling of the umbilical cord, and abnormally enlarged perimedullary veins is strongly indicative of a spinal vascular abnormality. Diagnostic angiography is indicated before surgery to map the vascular supply to the tumor deposit and plan preoperative embolization.
When performing surgery on the lower thoracic/upper lumbar spine or on the adjacent aorta, there is a risk of occlusion of the Adamkiewicz vessel. Extensive spinal DSA is not always appropriate in these circumstances due to the inherent risk of spinal cord ischemia.
A forward-facing catheter (eg, cobra shape) works well in the thoracic spine, but a retroflexed (Simmons 2 or 3) catheter shape may be better in the lumbar region. It is common for there to be a small infundibulum from which both segmental vessels arise, and it may be possible to move from right to left without completely freeing the catheter and simply to twist and reengage the other vessel.
Complications
Normal stage without distension of perimedullary veins indicates that there is venous hypertension and AVM/AVF is less likely. It alters normal hemodynamics and will prevent normal contrast flow to the perimedullary veins.
Usage, and Compatibility
More general considerations regarding the choice of guiding catheter often depend on personal preference or experience. What complications can be expected in a particular case and whether the guiding catheter will accept (separately or simultaneously) any additional catheters/balloons/stents etc.
Guide Catheter Types
Disadvantages: Large internal lumen can empty a lavage bag in seconds if not closely monitored, with the risk of gas embolus. Pros: Thin-walled profile, so 6 F version has slightly larger internal lumens than some of the other 6 F competitors.
Guide Catheter Positioning
Taking the anatomy into account, an attempt can be made to advance the guiding catheter to a more distal position (almost always a more proximal position will only worsen the problem). Place a stiff 'buddy' microwire next to the microcatheter with the tip inside the guiding catheter to provide additional support without traumatizing the vessel (e.g. Platinum plus 014, Boston Scientific).
Device Compatibility: French, Gauge and Inches Made Easy
The incidence of spontaneous aneurysmal subarachnoid hemorrhage is 6-10 per 100,000 patients per year, and the prevalence of intracranial aneurysms is between 1 and 5% of the population. The incidence of spontaneous aneurysmal subarachnoid hemorrhage (SAH) is 6–10 per 100,000 patients per year, and the prevalence of intracranial aneurysms is between 1 and 5% of the population.
Treatment Options
This has two peaks of increased risk: in the early and subacute phase within 24 hours and within 7–10 days. In general, if left uninsured, about 25% will rebleed within the first 2 weeks and two-thirds within the first 2 months.
Clinical Presentation
Due to the high rebleeding rate in aneurysmal SAH, urgent investigation and treatment has become routine after the publication of the International Study of Aneurysm Treatment (ISAT), and this has led to the subsequent development of interventional neuroradiology and endovascular neurosurgery. Aneurysms may present with mass effect (Fig. 3a, b) or rarely with thromboembolic complication of the intraluminal thrombus.
Risk Factors
Endovascular Aneurysm Treatment (EVT)
The length of the first coil should be sufficient to provide a stable peripheral configuration and cover the aneurysm neck with sufficient metal to prevent subsequent prolapse of the coil into the parent vessel. CEMRA in cases of stent remodeling or large aneurysms where post-contrast assessment of the aneurysm wall is required.
Two Years from EVT
Once the aneurysm is ligated, the MAP can be increased to prevent delayed cerebral ischemia (DCI). CTA (computed tomography angiography) can be used to determine incidental aneurysms in distant locations if there is a contraindication to MRI, but is usually not good enough to look at the coiled or clipped aneurysm.
Five Years from EVT
There has been a progressive, stepwise paradigm shift for the treatment of intracranial aneurysms, both ruptured and unruptured, via endovascular techniques. The appeal of endovascular techniques for patients lies in the minimally invasive approach and shorter recovery periods.
Indications
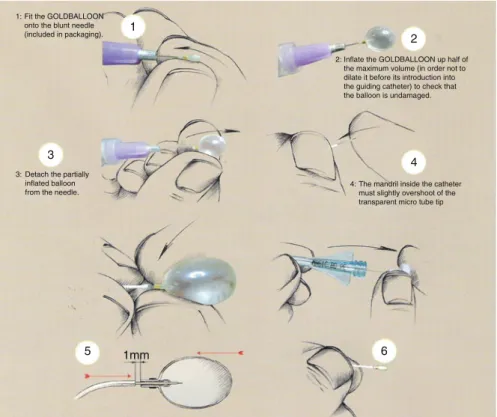
Balloon Configuration
Stage 1
Use of clear contrast results in prolonged balloon deflation, which may require removal of the microwire to achieve balloon deflation. It can potentially contaminate the microballoon with blood, making post-inflation difficult, reducing visibility and making post-deflation impossible, even when the microwire is fully withdrawn.
Stage 2
The importance of identifying the correct mixture of contrast and saline cannot be overemphasized to avoid balloon inflation with pure saline and the inherent risk of overinflation and vessel rupture.
Stage 3
Safety and Efficacy
Principle of Balloon Remodeling Technique
The duration of balloon inflation should be shortened as much as possible and longer inflation times exceeding 2 minutes should be avoided.
A balloon or a microcatheter can be positioned in the origin and proximal segment of the vessel to be "protected". Alternatively, the balloon can be advanced further into the most distal part of the vessel, allowing the microcatheter to be positioned.
The interface is usually irregular with large spaces between coil loops in the area of the aneurysm neck. Computed tomographic angiographic image in the axial plane 24 hours after reconstruction of the aneurysm shown in Fig.
When the aneurysm is completely excluded from circulation, the intra-aneurysmal thrombus begins to resorb and the entire mass of the aneurysm collapses around the periphery of the construct (Fig. 5. Cases most often performed within the context of "compassionate use): Case- Specific permission was obtained by regulatory bodies for patients with aneurysms not treated by conventional surgical or endovascular methods.
An understanding of these landing zones is more important than a consistent visualization of the aneurysm-parent artery interface (as opposed to aneurysm coiling). The duration of dual platelet therapy varies with the complexity of the aneurysm and the length of the reconstructed vessel.
Delayed parenchymal bleeding has been described after treatment of anterior circulation aneurysms with flow diverters. Very late thrombosis of flow-diverting constructs after treatment of large fusiform posterior circulation aneurysms.
The goal of treatment of cerebral aneurysms is complete, permanent closure of the aneurysm by preserving the parent artery and its branches (constructive technique). Parent artery occlusion or aneurysmal segment capture (deconstructive) techniques remain the safest option in some settings.
Indications for Treatment
Anatomy
Equipment
Embolization Techniques
The balloon may need to be deflated and reinflated more than once as you progress. It has only two nitinol mesh membranes covering the vessel lumen, so vessel occlusion may be slow.
Pre-procedure Medications
The Amplatzer 4 device is very attractive in that it can be delivered through a simple 4 F angiographic catheter that has a 0.038" lumen. Four membranes of nitinol mesh cover the lumen, but the wire is of a thinner quality, so occlusion is not as rapid as the Amplatzer 2 device, and more than one device may be required to achieve occlusion.
The patient can be extubated immediately after the procedure; they should be optimally monitored in Neuro ITU or HDU for 24 hours. Continued use of antiplatelet agents is inconsistent and should be considered on a case-by-case basis.
Follow-Up
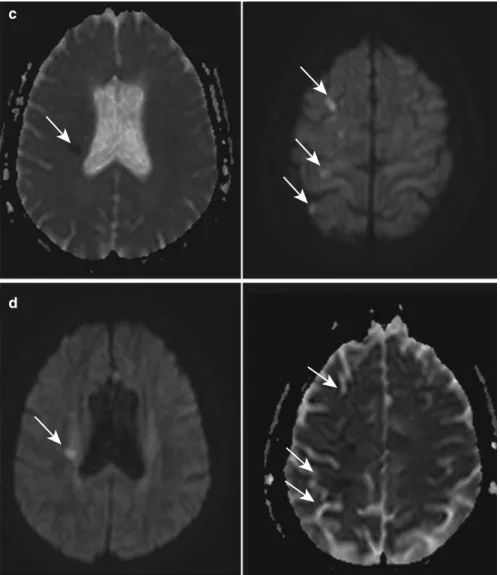
The patient should not be allowed to become hypotensive – a period of relative hypertension should be tolerated and antihypertensive medications should be used and resumed only later, gradually and after careful assessment. In the case of a new neurological deficit, MRI with diffusion-weighted imaging should be urgently performed to identify the lesion.
Alternative Treatments
Endovascular coiling of intracranial aneurysms is an accepted treatment with good outcomes and long-term efficacy. Endovascular coiling of intracranial aneurysms is an accepted treatment with good outcomes and long-term efficacy.
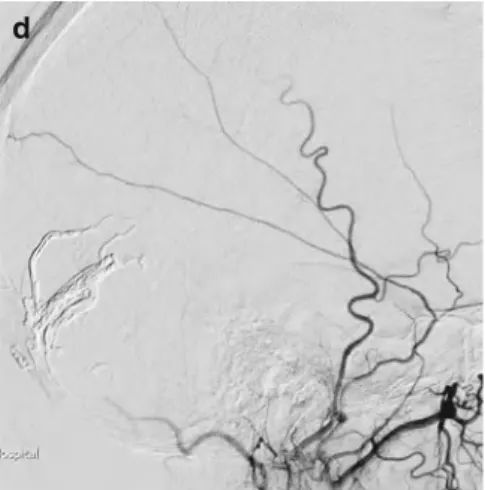
If distal access with the guide catheter is required, the catheter is advanced over the microcatheter/guidewire combination instead of the Terumo wire (Fig. 4a–c. Guide catheter placed in the petrous segment of the ICA to achieve stability for balloon-assisted coiling of ACOM aneurysm c ) Angiogram post -coiling shows dissection caused by guide catheters. d) Angiogram in the same patient shows post-stenting.
Aneurysm Coiling
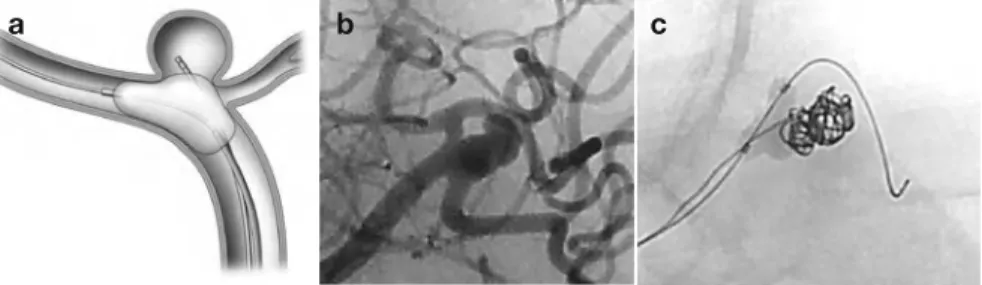
Other potential cause of rupture: while pushing coils out of microcatheters, which are opposite the walls of the aneurysm. Demonstrates tortuous vessel with small Rt MCA bifurcation aneurysm. build-up in the microcatheter is shown by positioning the catheter against the wall.
Thromboembolic Complications
One of the complications with the use of stents and balloons is wire perforation of small perforated vessels. During stenting and balloon use, great care must be taken in the position and placement of the distal wire.
Conclusion
Other less common causes of SAH include bleeding from an arteriovenous malformation, vasculitis, reversible cerebral vasoconstriction syndrome, and brain trauma. Other less common causes of SAH include hemorrhage from an arteriovenous malformation, vasculitis, reversible cerebral vasoconstriction syndrome (RCVS), and brain trauma.
Clinical Features
Pathophysiology
Risk of Vasospasm
Time Course
Benign oligemia: increased MTT, normal CBF and normal or increased CBV Penumbra: increased MTT, decreased CBF and normal or increased CBV. Irreversible ischemia: increased MTT, decreased CBF and decreased CBV. DSA remains the gold standard for evaluating cerebral vasospasm and is the basis for endovascular treatments.
Indications for Intervention
This will not prevent vasospasm in all cases, and up to 19% of patients may still develop major neurological disorders or death from vasospasm despite medical treatment. Patients who are unable to tolerate prolonged courses of hemodynamic therapy because of underlying medical comorbidities (eg, cardiac or renal insufficiency).
Contraindications
Calcium channel blockers (CCBs) are the most widely used agents due to their excellent safety and efficacy profile. Mechanical augmentation of smooth muscle and endothelial cells produces sustained patency of the spastic vessel segment.
Procedure
They work primarily by inhibiting voltage-gated calcium channels on smooth muscle cells, but there is also evidence of indirect neuroprotective effects.
Treatment Plan and Technique
Superselective injections have been performed for severe vasospasm, but there is no evidence in the literature to support the efficacy of this strategy versus proximal infusion. Vasopressor support may sometimes be necessary if there is a severe reduction in mean arterial pressure.
Balloon Angioplasty
Results
Reperfusion injury is a relatively rare complication and should be avoided by appropriate analysis of noninvasive studies and avoidance of large infarcts. The effect of IA vasodilators is generally not as permanent as that of angioplasty, so the intensive care team must be aware of the possibility of recurrent vasospasm.
Alternative Therapies
Safety and feasibility of intra-arterial nicardipine for the treatment of vasospasm associated with subarachnoid hemorrhage: initial clinical experience with high-dose infusions. Vasospasm after subarachnoid hemorrhage: utility of CT perfusion and CT angiography in diagnosis and management.
Arteriovenous Malformations
Minority associated with congenital and hereditary syndromes: Rendu-Osler-Weber, Wyburn-Mason and Sturge-Weber.
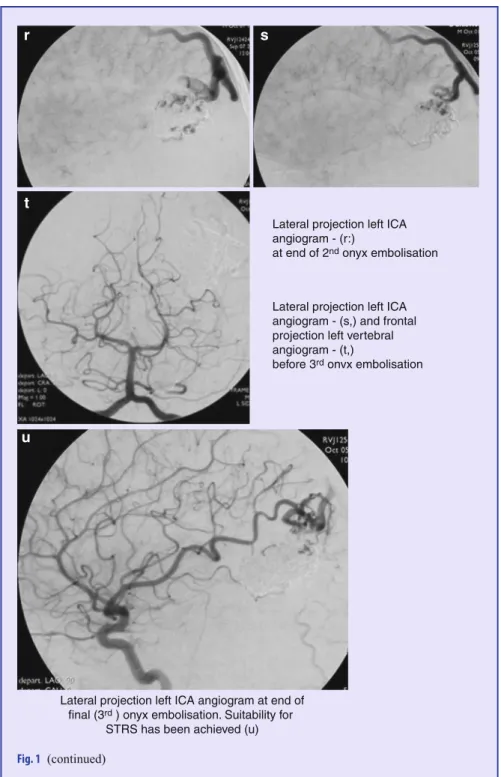
A point is assigned for size, location, deep venous drainage Eloquent cortex is sensorimotor, language, visual cortex, hypothalamus, internal capsule, brainstem, cerebellar peduncles, and deep cerebellar nuclei. STRS is the preferred single treatment for those <3 cm in diameter when the vascular anatomy is unsuitable for surgery and in anatomically difficult locations. For II–V, a combined approach with embolization (which may be staged) before surgery/STRS may be considered.
Embolic Agents
The author uses dexamethasone 12 mg intravenously at the beginning of each procedure to limit any inflammatory reactions that could be caused by the embolic agent.
A minimum of four-vessel angiography should be repeated at the start of each session of embolization. External carotid artery injections should be considered where dural supply is possible – superficial lesion/previous intervention.
Embolization Strategies
The microcatheter is navigated distally in a supplying arterial pedicle (care to avoid perforation) under roadmap guidance. Select angiographic protrusions that extend the microcatheter and do not overlap with the nidus or draining vein.
Post-procedural Care
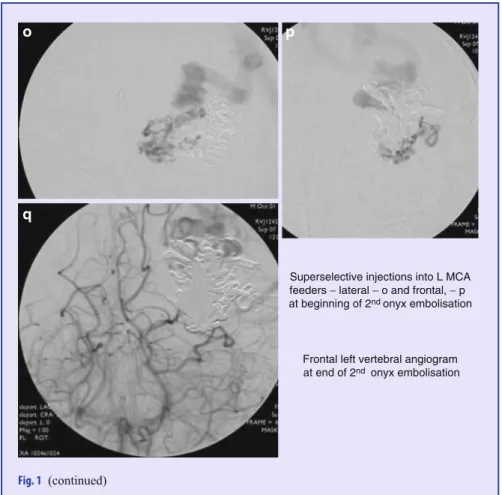
The goal was to reduce the size of the AVM to facilitate STRS and thus achieve complete obliteration. At the end of the second embolization, there was residual inflow from PCA-MCA collaterals (q) and distal MCA feeders (r.
Pathogenesis
Location
History of venous or arterial thrombotic events (DVT, pulmonary embolus (PE), etc.) both for pathogenesis of the DAVF and for prophylaxis against possible admission-related extracranial thrombotic events.
Classification of DAVF by Venous Drainage Pathway
Natural History
Transvenous access to the venous circulation can be indirect by femoral, cubital, or jugular puncture or direct through surgical access, orbitotomy, or direct puncture of the cavernous sinus. The diseased venous segment can be closed with coils (bare platinum, thread, or hydrogel) or onyx.
Surgery
Treatment Options Based on DAVF Location
Case 3b: Left ICA image showing filling of the DAVF from the meningohypophyseal trunk via the basal tentorial circulation. c. Example 5c: Left ICA image showing filling of the DAVF from the anterior ethmoid circulation arising from the left ophthalmic artery.
Carotid-Cavernous Fistula
Enlarged superior ophthalmic vein (SOV) (Fig. 4) Table 2 Barrow spontaneous carotid-cavernous fistula classification. Distal arterial territory supply – may be no antegrade flow in the ICA distal to fistula – cerebral hypoperfusion.
Transvenous injection of Onyx for casting of the cavernous sinus for the treatment of a carotid-cavernous fistula. Closure of carotid-cavernous fistulas by external compression of the carotid artery and jugular vein.