John Wiley & Sons, Ltd., The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, United Kingdom. The right of the author to be identified as the author of this work is asserted in terms of the Copyright, Designs and Patents Act 1988.
Contributors
Lynn began her nursing career in 1978 at the Royal Isle of Wight School of Nursing, becoming a state registered nurse working in acute care. Currently, Jane is a Program Counselor within the Pre-Registration Nursing Program at the University of Hertfordshire.
Acknowledgements
Introduction
The chapters
The chapter clearly explains the dangers to both the nurse and the patient if unsafe practices are adopted. The chapter begins by explaining the dynamics associated with thermoregulation and the role of the nurse in ensuring that the patient's body temperature is maintained as appropriate.
Terms used in the text
Sexuality as a life activity can often be neglected by nurses as it can have the potential to cause embarrassment and anxiety for both the nurse and the patient. Some people do not like the term 'service user' or 'user'; it could lead to the grouping of an otherwise diverse community of individuals with very individual needs.
For example, it can be used to identify those involved in the use of illegal substances. Informal carers are parents, grandparents and, in some cases, siblings who care for sick children.
The Nature of Nursing
Lynn Quinlivan
Learning opportunities
Pre-chapter quiz
It will also describe the hierarchical structure often associated with nursing and the roles and responsibilities of specific nursing positions. The National Health Service is not just a great institution, but a unique and very British expression of an ideal that health care is not a privilege to be bought, but a moral right guaranteed to all (Department of Health [DH ], 2008a).
The Nursing and Midwifery Council
Registration and professional accountability
Standards of conduct and performance
Maintenance of a register of nurses and midwives
In the reflection, the date and number of hours must be noted to ensure that a minimum of 35 hours is reached over 3 years. However, using a framework such as Gibbs' reflexive cycle (1992), a person can look retrospectively at the event and analyze his or her subsequent learning (Hogston and Simpson 2002).
Duty of care
For example, a district nurse may choose to attend a day of tissue viability study and then write a short reflective narrative that enables him or her to consider how this knowledge can be applied to clinical practice. For example, changing jobs or completing a period of study that has resulted in new and challenging responsibilities.
Fitness to practise
Nurses and accountability
The term "vicarious liability" refers to situations in which an employer accepts responsibility for the fault of its employees. Vicarious liability is laden with legal technicalities, so further reading in this area is recommended.
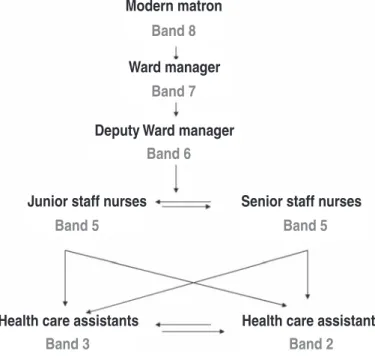
Nursing hierarchy
Ward manager
The Head of Department may be responsible for the recruitment and selection of new staff members. In addition, it may be involved in the implementation of government directives such as 'fractured neck of femur' (NHS Plan, 2000).
Government directives
For example, the "fractured neck of the femur pathway" is the integrated care pathway that aims to effectively and efficiently manage the patient's progression from accident and emergency department to discharge. This entry takes place within the first 12 months of appointment to any post, regardless of group, and aims to ensure that the individual is able to fulfill the role in question.
The structure of the NHS in England
PCTs are managed by local health services; within the primary care group are GPs, dentists, opticians, pharmacists and NHS Direct. Thirty-three ambulance services cover England and provide access to emergency medical care to the general population (DH, 2008b).
The structure of the NHS in Scotland
According to the government's strategic plans, some criteria related to the response time are defined.
The structure of the NHS in Wales
The structure of the NHS in Northern Ireland
Conclusions
Glossary
Standards for Better Health Seven care domains against which all care providers are measured.
Post-chapter quiz
Available at http://www.n-i.nhs.uk/. eds) (2002) Foundations of Nursing Practice: Making the Difference. Royal College of Nursing (2005) NHS Knowledge and Skills Framework outlines for Nursing Post.RCN Guidance for nurses and managers in creating KSF outlines in the NHS.
Safeguarding Vulnerable Adults
Victoria Darby
Safeguarding vulnerable adults is essential to ensure that individuals are empowered, respected and given the opportunity to make independent decisions about their health needs (Department of Health [DH], 2000). A number of the concepts will be used interchangeably throughout the chapter, but the key concept used is protecting vulnerable adults.
Defining a vulnerable adult and abuse
Vulnerable adult abuse statistics are broken down into many different categories, making it difficult to identify the extent of adult abuse in the UK. Action for Elder Abuse (2008) identified that approximately 4% of the elderly population in the UK experience abuse.
Ethics and safeguarding the vulnerable adult
However, the nurse has a duty of care to the patient and must adhere to robust guidelines for disclosing confidential patient information. To ensure that justice was maintained, the nurse had to ensure that all of the patient's nutritional needs were met.
Policies and legislation for safeguarding the vulnerable adult
Nurses should be aware of the policies and legislation that protect vulnerable adults and the specific policies identified by the clinical area in which they work. That is why the Ministry of Health, the Ministry of Criminal Justice and the Ministry of the Interior have started a review of the No Secrets directive.
Safeguarding vulnerable adults from unprofessional nurses
Some argue, for example, that it has created a set of specific criteria against which the vulnerable adult must be measured in order to benefit from protection (Dunn et al., 2008). With any legislation, it will be case law that identifies whether amendments or large-scale changes will be necessary in the future to protect vulnerable adults.
Fitness to practise panels
This may be because they have previously harmed a vulnerable adult or placed a vulnerable adult at risk of harm. This vetting and stopping scheme replaces and improves the POVA list by including NHS staff.
Interprofessional collaboration
Depending on the final sanction identified by the panel, the following decisions may be made regarding the nurse's ability to continue to practice.
Reporting suspicions of abuse as a nurse
It is important that the report is objective, without speculation or abbreviations or jargon. Student and registered nurses can advocate for an individual by ensuring that the rights and interests of vulnerable adults are protected (NMC, 2009).
Assessing the seriousness of abuse
Key guidelines for safeguarding vulnerable cases of adult abuse are to have a recognized co-ordinator and to ensure that the interprofessional framework is followed within a specific time frame. It is also essential that the decision-making process is shared in an interprofessional arena such as a case conference (DH, 2000).
Reporting suspicions of abuse as a student nurse
The investigation will also seek to identify what measures should be taken against the abuser of the vulnerable adult. List members of the multidisciplinary team who may be involved in the care of a vulnerable adult.
Assessing Needs and the Nursing Process
Lynda Sibson
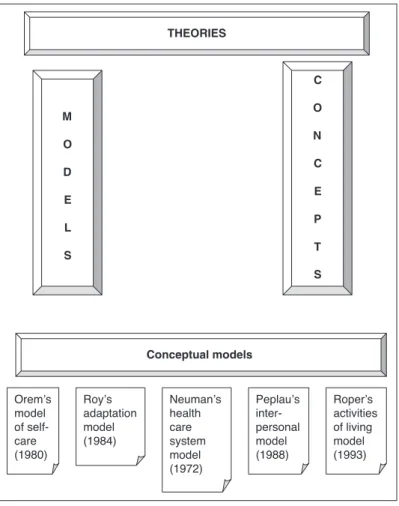
The aim of the chapter is to focus on a generic needs assessment from a broader perspective, particularly on some of the key concepts that underpin and inform practice in health care today. This chapter is not intended to include a detailed discussion of certain conceptual models of care, but rather to focus on some of the key components that support nursing practice.
Models of nursing
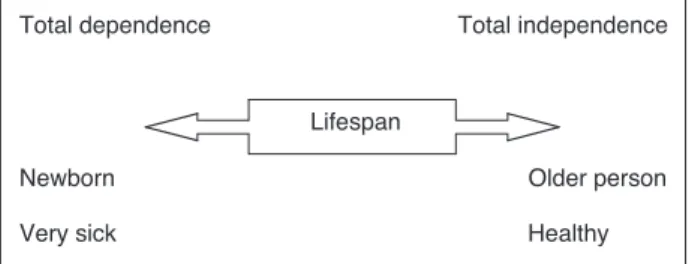
It will provide a background for the organization of nursing care, based on the Activities of Living approach of Roper et al. 2000), with specific reference to Florence Nightingale, who is considered by many to be the founder of nursing. Dependency will vary depending on illness and disease, and it is the assessment of the level of dependence and independence that is the cornerstone of nursing care, referenced from conception through to birth and death.
Activities of living
Organisation of nursing care
This approach was favored practice for many years, as nurses were considered to be 'the doctor's service'. As nurses have emerged as professionals in their own right, the 'science of nursing' has taken precedence, with nursing theory and knowledge seen as essential to achieving a scientific knowledge base in nursing practice (Chinn and Kramer, 1995).
Nursing practice
In other words, the nursing process is the approach to thinking and doing that nurses use in their work (Wilkinson, 1996). Nursing itself is a unique blend of art and science applied to our professional practice as nurses.
Nursing history
Florence volunteered again, and with 38 colleagues, she was appalled by the conditions she faced. At the same time, Mary Seacole, a black British woman born in Jamaica, provided health services to soldiers of the Crimean War.
Elements in nursing
Seacole worked at the front and at the docks, helping to nurse and care for men injured in the war. Her basic theory was that there was a connection between health and the environment, which had not been considered at the time.
Theories, concepts and models
She found that the environment in which her patients were cared for affected health and suggested that it was the physical, psychological and social environment that influenced health needs. As previously mentioned, this chapter will focus on the key components that make up the nursing process, rather than on individual conceptual models.

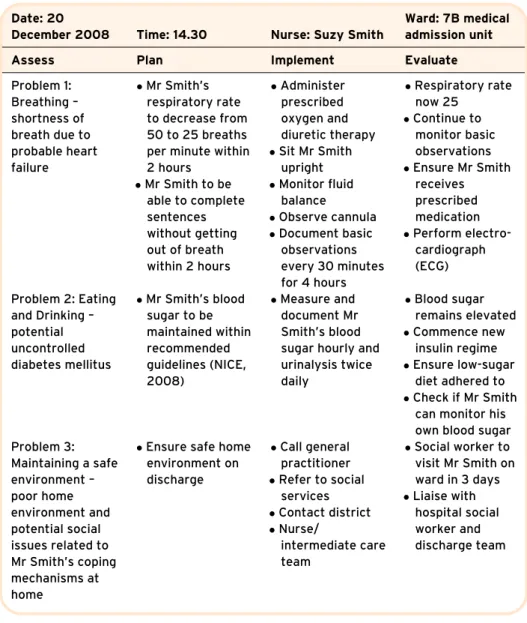
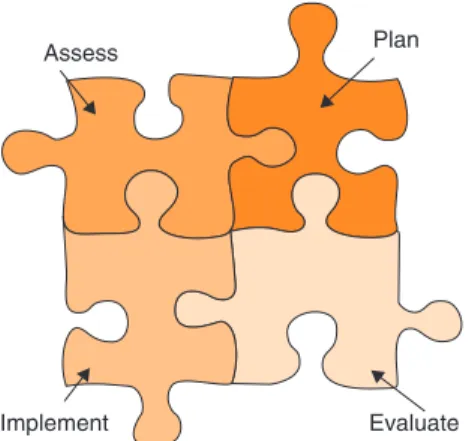
Nursing process
Determining the individual's need is the first step and clearly forms the basis of the process. It is essential that the information regarding the individual's needs is factual, relevant and comprehensive.
Promoting Safety
Janet G. Migliozzi
However, healthcare depends on a range of complex interactions between people, skills, technologies and medicines. This chapter focuses on minimizing risks for both patients and healthcare professionals.
Risk assessment
- Hazard identification
- Identification of who might be harmed and how
- Risk evaluation
- Documentation of risk assessment
- Risk assessment review and revision
As a result, healthcare professionals must be aware of the factors that affect patient and staff safety, what constitutes a safe environment for a particular person or group of people in a healthcare environment, and take steps to reduce risk accordingly. The second part of the chapter focuses on three areas of practice: medication administration, falls prevention, and infection prevention and control, and explores risk reduction methods related to these topics in the healthcare setting.
Common risks in health care
Provision and Use of Work Equipment Regulations (1998) Lifting Operations and Lifting Equipment Regulations (1998) Workplace (Health, Safety and Welfare) Regulations (1992) Construction (Planning and Management) Regulations (1994) Construction Regulations ( health safety and welfare) ( 1996) Control of Asbestos at Work Regulations (1987).
Common factors affecting patient safety
Minimising the risk of medication error
Before dispensing the medicine, it is important to check that the right patient receives it. To maintain a constant blood plasma level of the drug in an effective range, it is important to give the drug as close to the prescribed time as possible.
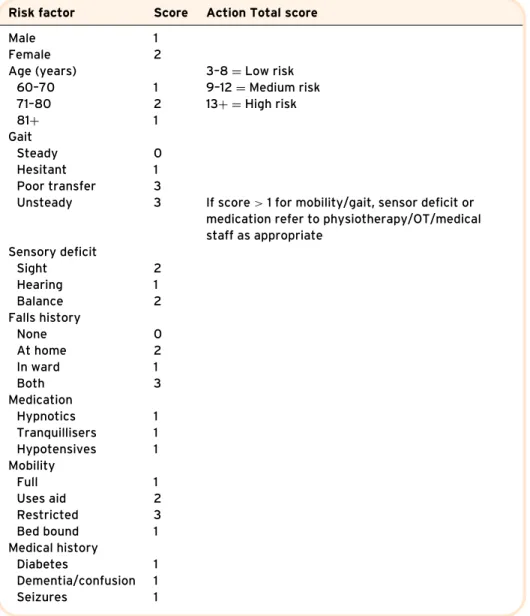
Minimising the risk of falls
Fall risk assessment is therefore an essential part of safe practice and there are many fall assessment tools that have been developed. A list of practical interventions that can reduce the risk of falls for older patients in a healthcare setting is provided in Box 4.3.
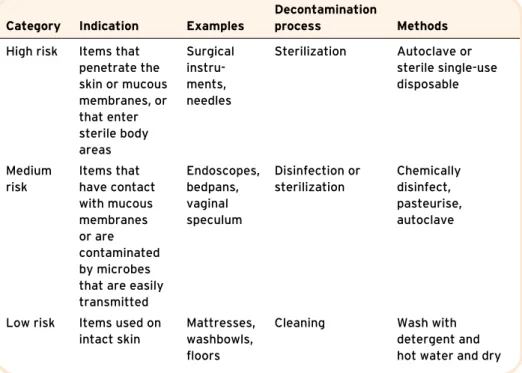
Minimising the risk of health care-associated infection
Chlorine-releasing granules or hypochlorite solutions should be used to remove bodily fluid spills, as they destroy the microorganisms present and thus reduce the risk of infection for the person cleaning up the spill (Gould and Brooker, 2008). Hands should be washed using a technique that ensures that all areas of the hand and wrists are sanitized.

Communicating Effectively
David Briggs
However, the process by which it is modified by the user within interpersonal interaction is a much more complex arrangement. Key issues related to the topic of communication are revisited and a story is developed on how to improve the reader's communication skills.
Understand how to use and receive non-verbal messages given by body language Use spoken, written and electronic methods of communication. Know when the information received should be passed on to another person/professional for action.
Talking to patients, carers and colleagues effectively and clearly conveying and receiving the intended message
For example, when talking to a chronic patient and family about maintaining the patient's independence, there may be multiple ways to address the same problem. For example, when a patient is being cared for at home, they may see a bed purchased downstairs as a way forward to be with their family, or they may want their upstairs room remodeled so that the family has a place to sit and talk. to them.
Facilitating patients and their carers to communicate effectively
By talking about the alternatives in care, the patient is encouraged to take ownership of any decision and is therefore more likely to act on it. communication) to encourage the patient to value you as a professional and to value what you stand for as a nurse.
The importance of listening effectively
Potential communication difficulties
Other factors include visual or hearing impairment and excessive noise in the room while the person is trying to talk to the patient. The concept of clear explanation by the person talking to the patient (instead of explaining out loud) was thought to be important.
The differing methods of communication used by individuals
Patients may also have problems with their perception of the meaning attached to the expressed ideas. Using these different methods allows various properties of each method to be best used when the sender sends the message.
Communicating with people from different cultures
Communication strategies should take into account the patient's belief system, and the patient should be approached with care and compassion. It is important that the nurse must show respect for the patient from another culture, and to do this he or she may need to involve an interpreter.
Coping in a very specific and difficult situation
The point of the conversation should be made quickly in as professional a manner as possible. Either way, if the nurse cannot speak the language of the patient, he or she should get an interpreter to bridge that gap to foster a caring environment.
Using body language effectively
An example is a nurse who turns her ear towards the patient while listening. What may seem superficial at first glance can be very important to the patient.
Using the electronic means of distributing information
The patient may be very aware of it, but the nurse, on the other hand, is left to decide whether to be upfront about it or to ignore its existence. The value of talking to a nurse or doctor is that the patient can ask them questions, the information can be related to the individual's circumstances, and the health professional can try to minimize the patient's anxiety.
The ability to know when someone needs to know a piece of information
This allows a report to be made on the patient's condition and care and to discuss what needs to be done for the patient in the future. The NMC in the code of conduct (NMC, 2008) sets out requirements for the nurse to act appropriately to ensure a level of trust between the patient and the nurse.
Information and record keeping
Such information must be kept confidential and passed only to the person who should have access to it. Hendrick (2000) reminds the reader of the importance of confidentiality and the fact that several issues must be considered when the police seek information from the health professional.
Communication and reflective practice
Unless all these aspects of communication are addressed in the delivery of care, the communication itself may be ineffective. Aspects of the chapter have considered the benefits of effective non-verbal communication and the benefits of good listening and how they can be used in healthcare.

Eating and Drinking: Fluid and Nutritional Care in Practice
Jane Say
Eating and drinking are normally social pursuits; how can the nurse ensure that eating and drinking remains a pleasant activity when caring for clients in the hospital? This chapter addresses specific nursing issues that arise in relation to eating and drinking in adult health care.
Nutritional issues and clinical practice
Describe the unique role and function of the nurse in relation to the client's fluid and nutritional needs. It will consider how you assess your clients in relation to their nutritional and fluid needs.
Obesity
The economic cost of the health problems caused by obesity has been estimated at £6.6–7.4 billion per year (House of Commons Health Committee, 2004). Nurses have a role in this strategy to promote healthy eating and lifestyle choices in their clients.
Undernutrition
He hopes that individuals, communities, the NHS and other aspects of the public sector, local government, the voluntary and community sector, the food industry, employers and the media will all contribute to finding sensible solutions to this growing health problem.
Disease-related factors
If such requirements are not met by the client's diet, deficiencies and malnutrition will occur. Changes in the client's psychological well-being, including conditions that cause chronic pain and depression, can also affect appetite and nutritional intake.
Non-disease-related factors
Specific disabilities, which are associated with changes in mobility or sensation (eg, arthritis, multiple sclerosis, cerebrovascular accidents, or coma), may affect how the client can eat. Physical factors such as poor oral/dental hygiene, dysphagia and pain while eating can also affect food intake.
Providing nutritional care in practice
The hospital includes specific guidelines for food services and nutritional care in its clinical governance arrangements. The hospital has a food service and food care policy which is patient-centred and performance managed in accordance with the governance frameworks of the country of origin.
Screening/assessment to identify patients’/clients’
All patients have a care plan which identifies their nutritional care needs and how they are to be met. Hospital facilities are designed to be flexible and patient-centered with the goal of providing and delivering an excellent food service and nutrition care experience 24 hours a day, every day.
Health professionals carrying out screening should receive the necessary education and training (NICE, 2006). In clinical practice, this is likely to be a registered nurse (and may include a nutritionist nurse) or a dietitian.
Body mass index
Examination should be performed at weekly intervals to further monitor the nutritional status of the client. This must be carried out by a registered contractor who has the necessary education and training and has been assessed as competent.
Weight loss
To facilitate the screening process, a number of screening tools have been developed which aim to determine the nutritional 'risk' status of the client (BAPEN, 2003; Reilly et al., 1995; Robshaw and Marbrow, 1995; Royal College of Nursing (RCN) ), 1993). Severe multiple injuries, multiple fractures/burns, multiple deep pressure sores/sores, severe sepsis, carcinoma/malignant disease.
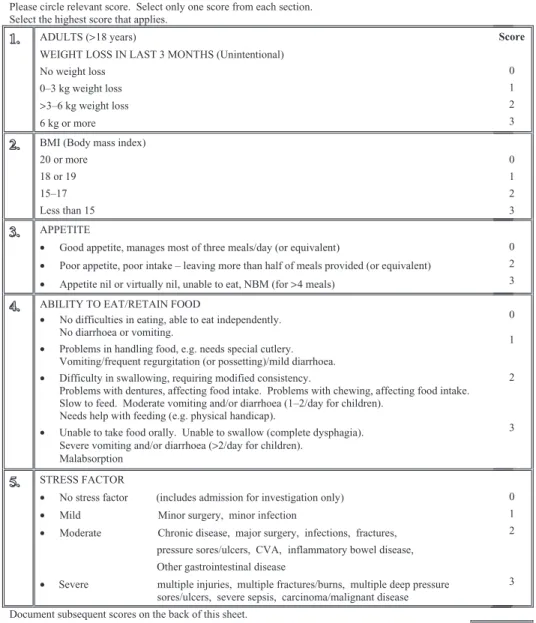
Recent dietary intakes
Stress factors/nature of current illness
For some patients, the nature of their condition may mean they eat little or nothing for some time. NICE (2006) recommends that those who have eaten little or nothing for more than 5 days and/or are likely to eat little or nothing for the next 5 days or longer should be classified as being at risk of malnutrition.
Further action, assessment and referral
Patients with poor absorptive capacity and/or high nutrient losses and/or increased nutritional requirements due to causes such as catabolism should also be classified as being at risk for malnutrition (NICE, 2006).
Planning, implementation and evaluation of nutritional care
Monitoring and re-screening
Previous work has indicated that there may be a lack of documentation on nutritional care and no clear strategy for nutritional care (including monitoring) (BAPEN, 2008). If necessary, informal carers can also be involved, provided they have learned how to fill in the correct administration.
Factors that affect nutritional care: the hospital and care environment
However, food intake should be monitored and action should be taken if there is any cause for concern (DH, 2001a). As recommended by the Council of Europe Association (UK), all staff should have the appropriate skills to ensure nutritional needs are met, and all aspects of food provision should be patient-centred.
Assistance with eating and drinking
Within a clinical area, the registered nurse will have ultimate responsibility for the overall environment and organization of the area. If the client agrees and when appropriate, encourage a relative or caregiver to help with their feeding.
Food provision
However, it is important that staff are properly trained and educated to provide this care and that they are aware of their roles and responsibilities in carrying out these activities.
Nutritional support
Improving oral intakes
Oral supplements
Enteral (or tube) feeding
As such, the client may need psychological and social support while receiving this type of food. Another aspect of care that needs attention is the client's oral hygiene or oral care.
Specific nursing care associated with enteral feeding
Clients (and their carers) receiving nutritional support in this way may be anxious and may need reassurance and explanations of the treatment involved. Nasojejunal feedings carry a greater risk of infection as the acidic environment of the stomach is bypassed.
Parenteral nutrition
As with the other types of enteral feeding, responsibility for the client's care will remain with the registered nurse. Any changes in the client's condition can then be acted upon quickly and further complications prevented.
Fluid management in clinical practice
Clinical assessment of fluid balance
There are a number of vital signs that can be used to assess and monitor a client's fluid balance. The choice of fluid will be determined by the client's condition and should be prescribed.
Conclusion
American Geriatrics Society, British Geriatrics Society and American Academy of Orthopedic Surgeons Panel on Fall Prevention (2001) Guidelines for preventing falls in older people. Journal of the American Geriatrics Society. 1988) The economic impact of malnutrition: a model system for hospitalized patients. Journal of Parenteral and Enteral Nutrition.
Elimination – Alimentary and Urinary Tract
Muralitharan Nair
Any undigested food, water, bacteria and dead cells lining the digestive tract are then eliminated. The small intestine is about 6 m long and the large intestine is about 1.5 m long (Mader, 2005).

The oral cavity
The tongue is an auxiliary organ which forms the floor of the mouth; it helps mix food when chewing and helps push food particles to the back of the mouth when swallowing. Tongue movement can change the volume of the oral cavity and also constitutes an important role in speech.
Pharynx
There are about 20 baby teeth and they usually begin to develop from 6 months of age. Often one pair of baby teeth grow per month and usually fall out between the ages of 6 and 12 years.
Oesophagus
It contains about 10,000 taste buds (Silverthorn, 1998), which tell us the taste of the food we eat, for example, whether the food is sweet or sour. The first permanent molars appear at age 6, the second at age 12, and the third may develop after age 13.
Stomach
This action is the result of three muscle layers in the stomach: longitudinal, circular and oblique muscles. While in the stomach, various digestive enzymes also help in breaking down food, thus helping in chemical digestion.
Small intestine
It must be broken down and only a small amount at a time is passed through the pylorus. Enzymes such as pepsin, for example, act on proteins and then convert them into peptones, gastric lipase begins the digestion of fats, and rennin converts the soluble protein of milk into an insoluble form.
Large intestine
The accessory organs
It is located in the upper right quadrant of the abdominal cavity below the diaphragm. The head of the pancreas lies in the loop of the duodenum and the tail touches the spleen (Marieb and Hoehn, 2007).

Care of patients with gastrointestinal disorders
Ask the patient to hold the suppository for at least 30 minutes or as recommended by the manufacturer before emptying the rectum. The contents of the bag should be observed and any changes, such as withdrawal of the stoma, reported to the nurse in charge.
Renal system
Patient education in ostomy care such as emptying the bag when necessary, applying the bag clamp and changing the ostomy bag helps acceptance of the ostomy and promotes patient independence (Finlay, 2002). Regardless of whether the ostomy is temporary or permanent, the patient will ultimately be responsible for the ostomy treatment upon discharge.
The prostate gland
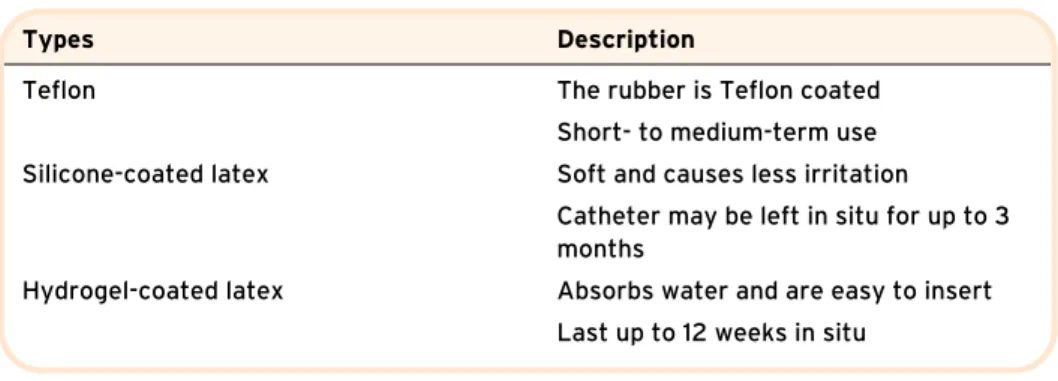
Care of patients with urological disorders
When cleaning the ear canal of the penis, the nurse must ensure that no infection enters the bladder. All care and outcomes must be documented accordingly to ensure that the care provided is based on an individual assessment of the patient's needs.
Breathing
Sean Mallon
Pryor and Prasad (2002) suggest that diseases associated with the respiratory tract account for the highest number of GP consultations. To effectively care for patients who have diseases of the respiratory tract, the nurse must understand the role that the respiratory tract plays in the metabolism of the body's cells (Cutler and Murch, 2003).
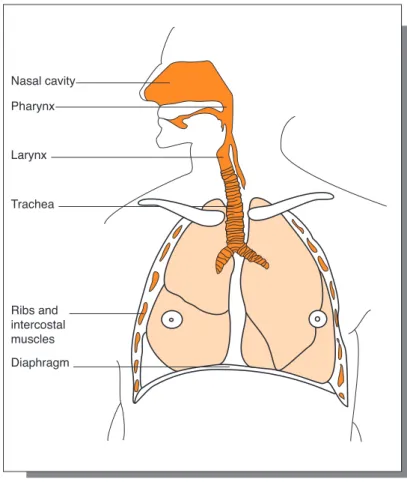
Structure and function of the respiratory tract
Phrenic nerves on either side of the diaphragm cause the diaphragm to contract, and the respiratory center, located in the brain (the medulla oblongata), controls this action. At the root of the lung is the parietal pleura, which covers the inside of the chest, the mediastinum and the diaphragm.
Assessment of respiration
The rate, depth, and rhythm of respirations should be noted, and the nurse should observe the chest wall to see if it moves equally on both sides. Listening skills are also required and the nurse must be alert to any noises made during inspiration and expiration.
Measuring respiratory rate, depth and rhythm
Respiratory distress may be associated with the use of the auxiliary muscles, so the distress may be visual, the nurse can learn a lot from the patient through close observation. The nurse records the observations in the patient's nursing notes according to the Guidelines for Records and Records (Nursing and Midwifery Council (NMC), 2007) and reports any airway abnormalities.
Respiratory sounds
He or she may need to change or adjust the frequency of observation based on the patient's condition. Evaluation of a patient with respiratory disease includes observation of the skin for signs of cyanosis.
Observation of cough and sputum
The nurse should also observe, record and report the type of sputum produced by the patient. A sputum sample can be obtained more easily from the patient if it is collected early in the morning.
Other methods of assessing respiratory function
The dial attached to the peak flow meter must be returned to the lowest setting between each test. If this is the case, the nurse should ask the patient to try the procedure only once and this should be noted on the chart.
Aerosols and nebulisers
The nebulizer is connected to an air or O2 flow and converts a solution of the prescribed medication (with 2-3 mL of saline [0.9%] saline) into an aerosol for inhalation. Nebulizer therapy is typically administered three to four times daily, and nebulizer use should be in accordance with local policy and procedure.
Some common respiratory diseases
The nurse must have acute observation skills to observe the patient's posture, verbal and non-verbal cues. It advocates that the nurse should record and report any changes in the patient's condition (NMC, 2007).
Personal Cleansing and Dressing
Laureen Hemming
Allen (2008) claims that this 'can be the most meaningful interaction of the day for the patient'. The skin is the largest organ of the body (Allen, 2008; Burr and Penzer, 2005), it forms a protective barrier and it can be damaged by neglect or exposure to the elements (Tortora and Derrickson, 2009).
Anatomy and physiology of the skin
The next layer consists of eight to ten layers of cells called the stratum spinosum. He claims that "the stratum corneum is not an inert protective barrier, but a most elegantly designed and dynamic structure".