Despite tremendous progress in the understanding and management of sleep disorders over the past 50 years, many sleep disorders remain underdiagnosed and undertreated. The book will be of interest to all clinicians who wish to improve their understanding and knowledge of sleep disorders.
PaO2 >10.6kPa
- How common is OSA?
- What are the main risk factors for OSA?
- What are the main presenting features of OSA?
- What are good clinical predictors of OSA?
- How do you confirm the diagnosis of OSA?
- Is there a correlation between symptoms of OSA and the severity measured on a sleep study?
The main features of OSA are snoring, perceived apnea and excessive daytime sleepiness (EDS). Several sleep questionnaires use a combination of the clinical features described here to predict or determine the risk of OSA.
An obese post-menopausal woman snored like a tank
- Does nasal obstruction cause or contribute to snoring and OSA?
- What is the natural history of a snorer?
- Is there an effect of gender on OSA?
- What are the possible reasons for gender differences in the prevalence and severity of OSA?
- Do sex hormones contribute to the difference in OSA between the two genders?
4 What are the possible reasons for gender differences in the incidence and severity of OSA. What are the possible reasons for gender differences in the incidence and severity of OSA.
Severe OSA in an overweight Chinese man—craniofacial
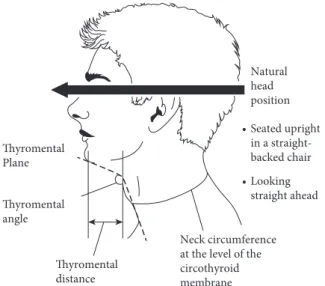
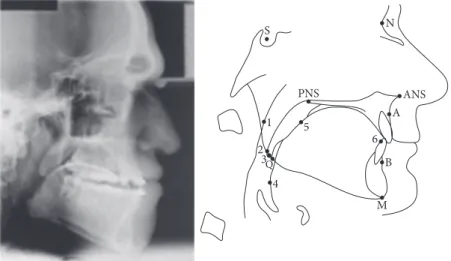
What are the craniofacial features associated with OSA and how can you detect these features?
Neck obesity with an increased neck collar size (>43) is one of the most prominent craniofacial features associated with OSA. However, detection of subtle craniofacial features, particularly skeletal features, associated with OSA requires detailed analysis of the lateral face and head radiograph (cephalogram) (see Figure 3.2).
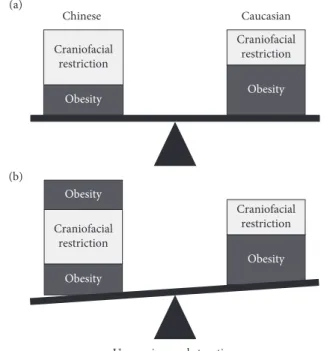
What is the contribution of craniofacial features to the prevalence of OSA in different ethnic populations?
What is the contribution of craniofacial characteristics to the prevalence of OSA in different ethnic populations.
What are the clinical implications of craniofacial abnormalities in OSA?
Non-CPAP treatments, such as a mandibular splint and surgical advancement of the mandible and maxilla, may have a more important role in OSA patients with craniofacial abnormalities. Craniofacial features (often genetic/racial) can cause OSA and increase the severity of OSA due to obesity.
Unable to throw a cricket ball and could not breathe at night
- What is the role of upper airways muscles in pathogen- esis of OSA?
- What are the common neuromuscular conditions that affect upper airway muscles?
- How common is sleep apnoea in FSH muscular dystrophy?
- Does upper airway muscle training, strengthening or stimulation have a role in the treatment of OSA?
There are four groups of upper airway muscles—the tongue, palatal, hyoid, and pharyngeal muscles. Upper airway muscles in patients with OSA are intrinsically normal—in fact, they work harder to keep the upper airway open.

A sleepy bus driver
How is sleepiness assessed?
Typically, a score of >11 is considered to indicate that the patient is drowsy, and a score of >15 indicates severe drowsiness. The patient is subjected to EEG monitoring and placed in a quiet, dark room for five separate periods.
What are the post-operative risks of sleep apnoea?
The test is mainly used to aid in the diagnosis of narcolepsy (a neurological disorder that causes drowsiness). In this case, the onset of REM sleep can occur during at least two sleep episodes with an average sleep latency of <8 minutes. considered diagnostic. Many anesthetists will recommend that postoperative patients with sleep apnea use CPAP when they are extubated. For this reason, they prefer that patients be started on and become accustomed to CPAP in the preoperative period.
What are the motor vehicle accident risks of sleep apnoea?
Reductions in lung volume will allow the upper airway to become more collapsible and may worsen pre-existing sleep apnea. It is very difficult to conduct any randomized trials on the risk of sleep apnea in the postoperative period, and much of the evidence comes from observational studies that vary widely in the surgery performed, the type of anesthesia given, and the location of postoperative care. (High dependency unit (HDU) versus ward).
Rapid onset daytime sleep presenting as transient loss
How do you differentiate between EDS due to OSA and transient loss of consciousness due to epilepsy?
However, rapid onset of intense daytime sleepiness leading to sleep may be confused with transient loss of consciousness due to other causes. EDS is primarily due to sleep disturbances and poor sleep quality as a result of recurrent obstructive apneas.
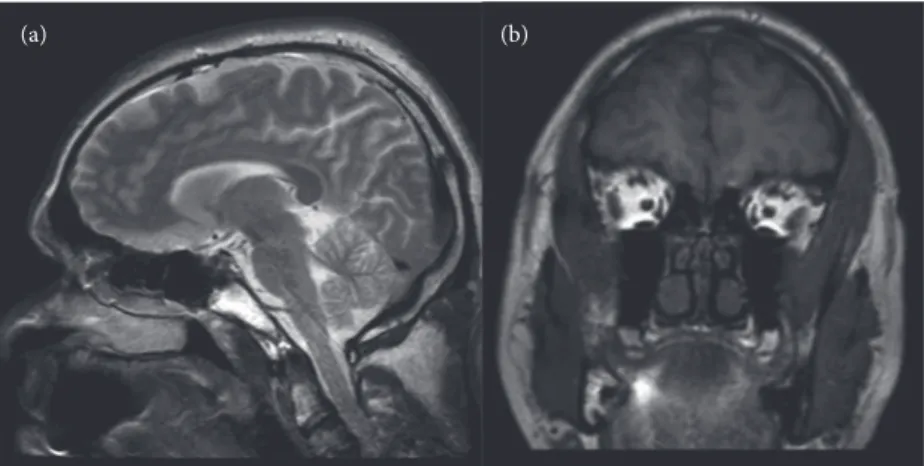
What does an MRI head scan show?
Transient loss of consciousness due to epilepsy is easy to recognize if it is associated with other features of epilepsy. EDS is common in OSA patients and they often report falling asleep while watching television, reading a book or sometimes when stopped at traffic lights while driving.
What are the effects of obstructive apnoea on the heart rate?
Unexplained breathlessness and pulmonary arterial
What was the explanation for the breathlessness?
Obese smokers are short of breath even at rest because the effect of a minor degree of airflow obstruction on breathlessness is exaggerated. Obesity often causes mild pulmonary restriction due to a large amount of extrathoracic and abdominal fat, which causes a reduction in chest wall compliance and diaphragmatic excursion.
What was the explanation for the pulmonary arterial hypertension?
The abdominal visceral obesity causes a mismatch between ventilation and perfusion at the lung base and a mild degree of hypoxia at rest, which worsens with exercise or lying flat. Approximately one third of patients with OSA have a modest degree of pulmonary arterial hypertension without a cardiopulmonary cause.
Why did he have nocturia and urinary frequency?
Post-operative apnoeas and
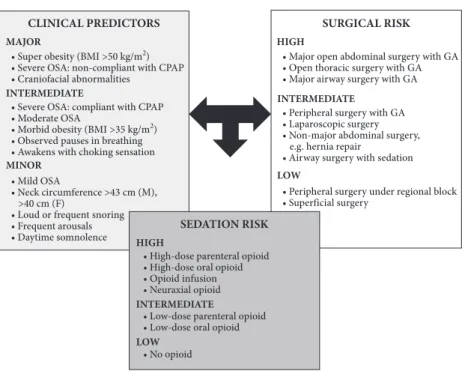
What are the peri-operative risks and peri-operative complications of undiagnosed/untreated OSA?
Prolonged apnea during the postoperative period during recovery from general anesthesia can cause respiratory distress and respiratory arrest. In addition, trauma from airway manipulation, medications, and pain can affect sleep architecture and upper airway muscle regulation in the postoperative period.
How can you prevent these complications?
Patients with OSA have a narrow upper airway and are at increased risk for difficult (tracheal) intubation. Is there any difference in risks between different types of surgery in patients with OSA?
Is there any difference in the risks between different types of surgery in patients with OSA?
However, patients undergoing upper airway surgery have a much higher risk of postoperative dyspnea and respiratory complications. OSA patients at high risk for postoperative complications, such as morbidly obese patients with cardiovascular comorbidities, should have a sleep study and CPAP established before surgery.
Polycythemia got better with CPAP
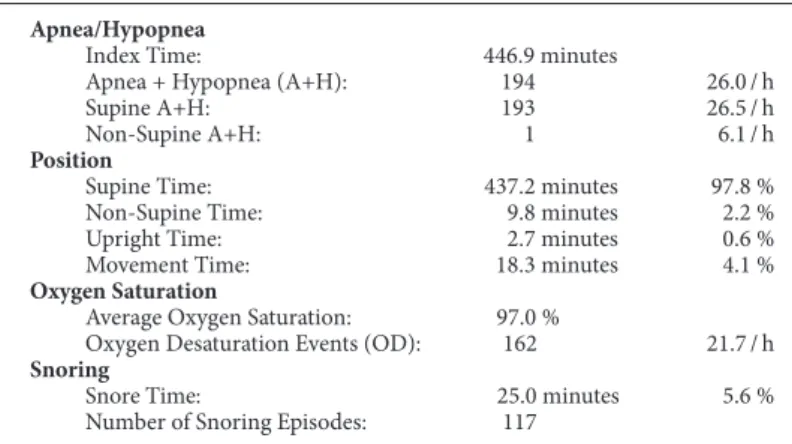
- What are the criteria for the diagnosis of OSA?
- How does OSA affect sleep?
- What is the effect of OSA on respiration during sleep?
- What is the effect of CPAP on sleep and respiration in OSA?
Apneas and hypopneas during sleep result in recurrent arousals, sleep fragmentation and poor sleep quality. Apneas and hypopneas during sleep result in recurrent nocturnal SaO2 desaturation and chronic intermittent nocturnal hypoxia.

Hyperphagia and sleep disorder in Prader-Willi Syndrome
What are the common causes of obesity in children?
Obesity in most children is due to an unhealthy lifestyle—overeating and lack of exercise. In most it is due to non-inherited (de novo) mutation in paternally derived chromosome 15.
What is the explanation for hyperphagia and obesity in patient with Prader-Willi Syndrome?
How common is sleep apnoea in patients with Prader- Willi Syndrome?
Marked daytime sleepiness (hypersomnia) is due to a combination of OSA and hypothalamic dysfunction, and may persist despite treatment of OSA. In most children it is due to an unhealthy lifestyle, but in a few it may be due to genetic and endocrine causes.
Shot in the head—acquired hypothalamic syndrome
What is the role of hypothalamus in control of appetite and sleep?
Appetite (hunger and satiety) is controlled by a group of neurons located in the ventromedial nucleus of the hypothalamus. Neurons in the lateral part control satiety - stimulation of the satiety center causes an increase in food intake while damage leads to complete cessation of food intake.
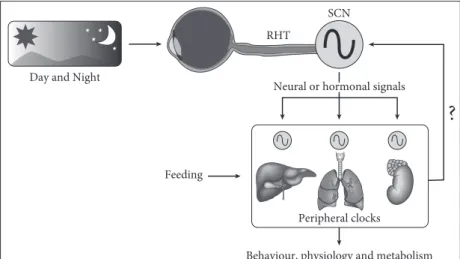
How is our sleep rhythm generated and controlled?
This makes us feel sleepy at certain times of the day - late evening or afternoon. These environmental signals, the core circuit oscillator, and output rhythms are three basic components of the circadian clock system.
What is hypothalamic syndrome?
Dhibee Hojii Gadi Dhiigaa (Hypothalamic Syndromes) 2.4.1 Kitaaba Barnootaa Oksifoord kan Endocrinology fi Dhukkuba Sukkaaraa (Maxxansa 2ffaa) Gulaalaa JAH Wass, PM Stew-art, SA Amiel, MC Davies.
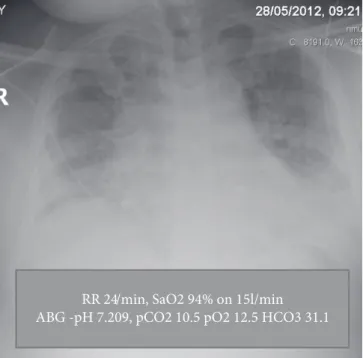
Collapsed in a café: acute respiratory failure
- What are the clinical features of acute hypercapnic res- piratory failure?
- What are the common causes of acute hypercapnic respiratory failure?
- How does obesity affect the respiratory system?
- What is obesity hypoventilation syndrome, or Pickwickian syndrome?
- How does OSA/obesity hypoventilation syndrome increase the risk of AHRF?
5 How does OSA/obesity hypoventilation syndrome increase the risk of acute hypercapnic respiratory failure (AHRF). The absence of clinical features of respiratory distress, especially in patients without known respiratory disease, can make acute hypercapnic respiratory failure difficult to recognize.
Overlap syndrome—COPD and OSA
What is overlap syndrome?
Both conditions are very common and it has been suggested that the presence of one condition increases the chance of finding the other by 10%. In animal models of OSA, it has been noted that repeated upper airway collapse causes increased lower airway resistance, which can worsen the symptoms of COPD.
When should overlap syndrome be suspected?
In patients with OSA and a significant smoking history who remain drowsy despite good CPAP compliance at an adequate pressure, the diagnosis should be considered. COPD patients with more pulmonary hypertension than might be expected or those with symptoms suggestive of OSA should be referred for a full assessment by a sleep physician.
How is overlap syndrome treated?
Thus, it seems reasonable to screen patients with COPD or OSA for signs of the other conditions, as the mortality associated with overlap syndrome is higher than for either condition alone. Patients with overlap syndrome (combination of OSA with COPD) are more symptomatic and at higher risk of pulmonary hypertension and respiratory failure than those with OSA alone.
Neuropsychological impairment in a psychoanalyst with
What is post-polio syndrome?
Describe the respiratory problems in patients with post- polio syndrome
A large proportion (75%) of patients who have had polio in childhood, which mainly requires iron lung ventilation, develop further muscle weakness and fatigue after a latent period of 30 years due to a gradual deterioration of the anterior horn cells (motor neurons) in the heart. the spinal cord. However, with a further increase in respiratory muscle weakness and a reduction in vital capacity, they develop respiratory failure and hypoxia during the day.
How do you differentiate between nocturnal
Daytime dyspnea due to reduced mobility is rarely reported, and daytime resting SaO2 is normal. OSA is primarily caused by upper airway muscle weakness and responds well to CPAP.
Nocturnal choking in a patient with a goitre and retrosternal
How does the spirometry flow volume loop help with di- agnosis of upper airway obstruction?
Peak inspiratory flow volume (MIFV) is greatly reduced at mid-lung volume compared with peak expiratory flow volume (MEFV) in patients with floppy upper airways. Therefore, an incidental finding of a sawtooth pattern on the spirometry flow volume loop should lead to a diagnosis of OSA.
Do thyroid problems cause or contribute to upper airway obstruction in OSA?
Are cigarette smoking and drinking alcohol risk factors for OSA?
Epidemiological studies have shown a variable association between self-reported alcohol consumption and sleep apnea, particularly in men. The presence of a sawtooth pattern in the output limb of the volume flow circuit and an increase in MEF50/MIF50 should be investigated for OSA.

OSA persists despite removal of a pituitary tumour causing
- How common is sleep apnoea in acromegaly patients?
- What is the cause of OSA in acromegaly?
- Does cure of acromegaly improve or eliminate sleep apnoea?
- Is it safe to use CPAP after transsphenoidal surgery?
Upper airway edema due to transsphenoidal surgery in patients with acromegaly with OSA may increase the risk of postoperative respiratory problems. Treatment of acromegaly (surgical or medical) can lead to complete reversal of OSA, but in a significant part (40%) of patients it persists.

CPAP transformed my life
What is the lag time for the diagnosis of sleep apnoea?
A recent survey of undergraduate medical education in the UK found that the average teaching for all aspects of sleep medicine (pathology, pharmacology and diagnostic evaluation) was 2.5 hours. Even when patients exhibit clinical features of sleep apnea, there may be poor recognition by the medical profession.
What opportunities are there for screening patients for sleep apnoea?
It is therefore perhaps not surprising that doctors themselves may have difficulty recognizing the signs and symptoms of sleep apnea. Often, symptoms of OSA, such as sleepiness and nocturia, can be attributed to type 2 diabetes mellitus.
What are the consequences of untreated sleep apnoea?
There is a long delay between the onset of symptoms of OSA and diagnosis due to a lack of awareness among the population and insufficient education in health professionals. CPAP is the most effective treatment for OSA and results in the resolution of symptoms, an improvement in quality of life, and a reduction in the risk of driving-related accidents and cardiovascular morbidity.
Persistent daytime sleepiness despite CPAP
- How common is persistent EDS despite CPAP in OSA?
- What is the initial management of patients who report persistent daytime sleepiness despite CPAP?
- What is the next step in patients who have persistent EDS, despite good objective demonstration of good CPAP
- Are there any therapeutic options for persistent daytime sleepiness?
Suboptimal CPAP compliance is one of the most common causes of persistent symptoms, including daytime sleepiness. Longer hours of CPAP use result in further improvements in daytime sleepiness: the more, the better.

CPAP intolerance and
What are the main reasons for CPAP intolerance and non-compliance?
Compliance with CPAP is likely to be much better if CPAP therapy is explained to the patient and set up by an experienced sleep professional with proper CPAP mask selection and CPAP pressure titration. Cognitive behavioral therapy (CBT) can help, especially for patients who feel claustrophobic with a CPAP mask.
Are there any curative treatments for OSA?
In general, symptomatic patients with EDS are more likely to comply with CPAP than patients with few symptoms. However, a clear explanation about the long-term health benefits of CPAP may convince asymptomatic patients to comply with CPAP.
What is the role of MAS in the management of OSA?
The use of splint was as much dependent on social conditions as physical symptoms in patients with mild sleep apnea. In more severe cases in patients with daytime symptoms, the splint was preferred over CPAP, and compliance was better.
Will not use CPAP—ends up with tracheostomy
What are the risks associated with untreated OSA?
The use of CPAP during the peri-operative period can reduce the post-operative risks in OSA patients. There is evidence that OSA patients who are well established on CPAP before surgery have a lower risk of post-operative problems.
What are the pros and cons of tracheostomy for the treatment of OSA?
OSA alone at least doubles the risk of cardiovascular disease, especially in men with severe OSA. Similarly, patients with OSA have approximately twice the risk of death from sudden death, cardiovascular causes, and cancer.
Bariatric surgery cures sleep apnoea
What are the current guidelines regarding referral of patients for consideration of bariatric surgery?
Current NICE guidelines suggest that bariatric surgery should be considered in patients with a BMI >40. However, bariatric surgery should be considered as a first-line option in those with BMI >50, as these patients are unlikely to achieve weight loss through lifestyle changes or drug treatment alone.
What are the benefits of bariatric surgery?
Patients should be referred to a specialist weight loss service and should be aware that long-term follow-up will be required and be prepared to adhere to this follow-up. However, weight loss is greater than with the other two procedures and there is a higher rate of discontinuation of medical treatment in people with diabetes.
How does weight loss impact on OSA?
Patients with sleep apnea should be followed up after bariatric surgery until their weight loss has subsided. Weight loss after bariatric surgery such as sleeve gastrectomy and gastric bypass not only cures sleep apnea, but also type 2 diabetes mellitus, hypertension and hyperlipidemia.
Sleep disturbance and daytime sleepiness persists in a snorer
What is the differential diagnosis of sleep disruption and daytime sleepiness in a snorer?
The oximetry sleep study in a symptomatic OSA patient often shows a characteristic repetitive oxygen desaturation pattern. However, negative sleep study screening in a sleepy snorer and failure of response to a therapeutic trial of CPAP should lead to consideration of an alternative diagnosis.
What are the common movement disorders during sleep?
Snoring is very common, and sleep disturbances and daytime sleepiness in snorers are often the result of OSA. It has been suggested that treatment of OSA with CPAP may hasten the resolution of underlying PLMS.
What is PLMS?
The patient's or partner's description of the state of the bedding and the movements during sleep can also provide a clue to the diagnosis. Clues to the diagnosis may be provided by the partner's report of being kicked during sleep or the condition of the bedding in the morning.
Worrying pauses in breath
Central Sleep Apnoea
What is CSA?
Typical CSA patients have witnessed apnea but no snoring or choking episodes. CSA must be distinguished from "pseudo-CSA" in patients with respiratory muscle weakness/paralysis with OSA.
How does heart failure cause CSA?
It is clear that this group of patients will not respond to CPAP and may contribute to CPAP non-adherence.
How do you treat CSA?
In patients with CSR-type CSA, optimization of heart failure treatment improves CSA. Suspected CSA as a cause of observed apnea in patients without history of snoring or choking episodes during sleep.
- What will you do next?
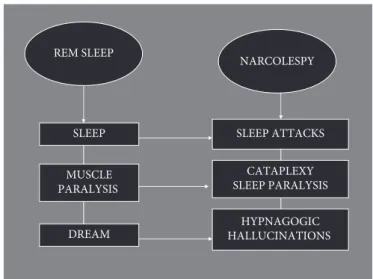
- What is the probable diagnosis and how will you confirm the diagnosis?
- What is the cause of narcolepsy?
- How do you treat narcolepsy?
The cause of narcolepsy is unknown, but levels of the brain (hypothalamus) neuropeptide hypocretin are low. The cause of narcolepsy is unknown, but levels of the brain (hypothalamus) neuropeptide hypocretin are low.
Contribution of facial skeletal pattern to sleep apnoea
What is the value of sleep nasendoscopy in MAS selection?
The sleep nasendoscopy allows a dynamic evaluation of the pharyngeal airway in a state that 'mimics' sleep and allows an assessment of the site of collapse and the effect on both airway collapse and snoring while performing simulated mandibular advancement.
What type of follow-up measures would be appropriate for a patient with severe sleep apnoea being treated
How can the facial skeletal pattern of OSA patients be assessed? List two such findings
Effectiveness of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. A study of the changes in airway dimension and effectiveness of mandibular advancement devices in subjects with obstructive sleep apnea.
MAS therapy for severe OSAHS
What severity of OSA is recommended for the treatment with MAS therapy as a first-line choice?
Name two reported benefits of using the MDSA
Effectiveness, compliance
List one advantage and one disadvantage to a patient re- ceiving a customized MAS, when compared to a ‘boil and
What is the importance of ensuring patients have optimal dental health and asymptomatic TMJs prior to
What dental measurements permit the dentist to monitor the development of any occlusal side effects?
Sleep nasendoscopy: a diagnostic tool for predicting treatment success with mandibular advancement splints in obstructive sleep apnea.
Allergic rhinitis
What nasal symptoms should be sought out when taking a history from this patient?
On examination, the nasal septum was in the midline, but the nasal mucosa was very pale and edematous. The nasal airways were very restricted and there was a large amount of rhinorrhea in the nasal cavity.
What investigations could you consider?