Care has been taken to confirm the accuracy of the information present and to describe generally accepted practices. Performance and state of mind are essential for an individual's physical health.
THE BEGINNING OF LIFE: PREGNANCY
Childbirth and the Postpartum Period 1 I Infancy: Birth to 15 Months 4
SCHOOL AGE, ADOLESCENCE, SPECIAL ISSUES
Latency or School Age: 7–11 Years 13 I Adolescence: 11–20 Years 14
Middle Adulthood: 40–65 Years 16 Review Test 18
Aging 23
Stages of Dying and Death 25
Bereavement (Normal Grief) Versus Depression (Abnormal Grief or Complicated Bereavement) 25
GENETICS, ANATOMY, AND BIOCHEMISTRY OF BEHAVIOR 31
Behavioral Genetics 31 I Behavioral Neuroanatomy 32
Neurotransmission 34 IV. Biogenic Amines 35
Amino Acid Neurotransmitters 37 VI. Neuropeptides 37
BIOLOGICAL ASSESSMENT OF PATIENTS
Overview 44
Measurement of Biogenic Amines and Psychotropic Drugs 44 I Dexamethasone Suppression Test (DST) 45
Tests of Endocrine Function 45
Neuroimaging and Electroencephalogram Studies 45 VI. Neuropsychological Tests 46
Other Tests 47 Review Test 48
PSYCHOANALYTIC THEORY AND DEFENSE
Overview 52
Freud’s Theories of the Mind 52 I Defense Mechanisms 53
Overview 60
Habituation and Sensitization 60 I Classical Conditioning 61
Operant Conditioning 61 Review Test 64
CLINICAL ASSESSMENT OF PATIENTS
Overview of Psychological Testing 69 I Intelligence Tests 69
Achievement Tests 70 IV. Personality Tests 71
Psychiatric Evaluation of the Patient with Emotional Symptoms 71 Review Test 74
SUBSTANCE ABUSE 77
Substance Abuse, Definitions, Epidemiology, and Demographics 77 I Stimulants 78
Sedatives 79 IV. Opioids 81
Hallucinogens and Related Agents 82 VI. Clinical Features of Substance Abuse 83
NORMAL SLEEP AND SLEEP DISORDERS 91
Normal Awake and Sleep States 91 I Classification of Sleep Disorders 93
Breathing-Related Sleep Disorder (Sleep Apnea) 95 V. Narcolepsy 95
Treatment of Sleep Disorders 95 Review Test 97
SCHIZOPHRENIA AND OTHER PSYCHOTIC DISORDERS 103
Schizophrenia 103
Other Psychotic Disorders 106 Review Test 108
Overview 113
Classification of Mood Disorders 114 I Etiology 117
Treatment 118 Review Test 119
ANXIETY, SOMATOFORM AND FACTITIOUS
Anxiety Disorders 124 I Somatoform Disorders 126
Factitious Disorder (Formerly Munchausen Syndrome), Factitious Disorder by Proxy, and Malingering 127
COGNITIVE, PERSONALITY, DISSOCIATIVE,
Cognitive Disorders 136 I Personality Disorders 139
PSYCHIATRIC DISORDERS IN CHILDREN 150
Pervasive Developmental Disorders of Childhood 150
Attention Deficit Hyperactivity Disorder and Disruptive Behavior Disorders of Childhood 151
Other Disorders of Childhood 152 Review Test 154
BIOLOGIC THERAPIES: PSYCHOPHARMACOLOGY 158
Overview 158
Antipsychotic Agents 158 I Antidepressant Agents 160
Antianxiety Agents 163
Electroconvulsive Therapy 164 Review Test 166
Psychoanalysis and Related Therapies 172 I Behavioral Therapies 173
Other Therapies 174 Review Test 176
THE FAMILY, CULTURE, AND ILLNESS 180
Overview of the Family 180
Demographics and Current Trends 180 I Culture in the United States 181
SEXUALITY 189
Sexual Development 189
The Biology of Sexuality in Adults 190 I Sexual Dysfunction 191
Paraphilias 193
Drugs and Sexuality 195
The Human Immunodeficiency Virus and Sexuality 195 Review Test 197
Aggression 203
Abuse and Neglect of Children and the Elderly 204 I Physical and Sexual Abuse of Domestic Partners 206
The Role of the Physician in Suspected Child, Elder, and Domestic Partner Abuse 206
Sexual Aggression: Rape and Related Crimes 207 Review Test 209
THE PHYSICIAN-PATIENT RELATIONSHIP 213
Medical Practice 213
Compliance (Adherence) 214 I The Clinical Interview 215
Stress and Health 225
Psychological Stress in Specific Patients 226 I Patients with Chronic Pain 227
Patients with Acquired Immune Deficiency Syndrome 228 Review Test 229
LEGAL AND ETHICAL ISSUES IN MEDICINE 233
Legal Competence 233 I Informed Consent 234
Ethical Issues Involving HIV Infection 236
Involuntary and Voluntary Psychiatric Hospitalization 236
Advance Directives 237 VIII. Death and Euthanasia 237
Medical Malpractice 238 X. Impaired Physicians 239
Answering USMLE Legal and Ethical Issues Questions 239 Review Test 240
HEALTH CARE IN THE UNITED STATES 249
Health Care Delivery Systems 249 I Costs of Health Care 250
Payment for Health Care: Health Insurance 251 IV. Demographics of Health 252
Epidemiology: Incidence and Prevalence 259 I Research Study Design 260
Quantifying Risk 260
Elements of Statistical Analyses 273 I Hypothesis Testing 276
Specific Statistical Tests 276 Review Test 278
While she previously slept in her own bed, a five-year-old girl begs to sleep in her mother's bed every night after her parents' divorce.
CHILDBIRTH AND THE POSTPARTUM PERIOD
Birth rate and cesarean birth
Premature birth
Infant mortality
Postpartum maternal reactions 1. Baby blues
INFANCY: BIRTH TO 15 MONTHS
Bonding of the parent to the infant
Attachment of the infant to the parent
With continued absence of the mother, the infant is at risk for depression
Studies of attachment
Harry Harlow demonstrated that infant monkeys reared in relative isolation by surrogate artificial mothers do not develop normal mating, maternal, and social behaviors as
Characteristics of the infant
Theories of development
THE TODDLER YEARS: 15 MONTHS–2 1 / 2 YEARS
Attachment
Motor, social, verbal, and cognitive characteristics of the toddler See Table 1-6
THE PRESCHOOL CHILD: 3–6 YEARS
Characteristics
Changes at 6 years of age
LATENCY OR SCHOOL AGE: 7–11 YEARS
Prefers to play with children of the same sex; usually avoids and is critical of the opposite sex. Conservation involves understanding that an amount of a substance remains the same regardless of the size of the container or the shape it is in (eg, two containers can contain the same amount of water even though one is a long, thin tube and one is a short, wide bowl).
ADOLESCENCE: 11–20 YEARS
Seriation involves the ability to arrange objects in order with respect to their sizes or other properties.
Early adolescence (11–14 years of age)
Middle adolescence (14–17 years of age) 1. Characteristics
Risk-taking behavior
Late adolescence (17–20 years of age) 1. Development
Teenage sexuality
Teenage pregnancy
SPECIAL ISSUES IN CHILD DEVELOPMENT
Adoption
Children should be told by their parents that they are adopted at the earliest age possible to avoid the chance of others telling them first
EARLY ADULTHOOD: 20–40 YEARS
Characteristics
Responsibilities and relationships
MIDDLE ADULTHOOD: 40–65 YEARS
Relationships
Seventy to eighty percent of men in their middle 40s or early 50s exhibit a midlife crisis
Midlife crisis is associated with an awareness of one’s own aging and death and severe or unexpected lifestyle changes (e.g., death of a spouse, loss of a job, serious illness)
Thus, the doctor should ask the 15-year-old to leave and talk to the 8-year-old with the mother present. The answer is E. The best thing for the medical student at this time is to interact with the child.
AGING
Demographics
Somatic and neurologic changes
Cognitive changes
Although learning speed may decrease, in the absence of brain disease, intelligence remains approximately the same throughout life
Psychological changes
Psychopathology and related problems
Life expectancy and longevity
STAGES OF DYING AND DEATH
BEREAVEMENT (NORMAL GRIEF) VERSUS DEPRESSION (ABNORMAL GRIEF OR COMPLICATED BEREAVEMENT)
Characteristics of normal grief (bereavement)
Grief is characterized initially by shock and denial
The stages usually occur in the following order, but may also be present simultaneously or in a different order. Mortality is high for close relatives (especially men who are widowed) in the first year of bereavement.
Physician’s response to death
BEHAVIORAL GENETICS
- Twin studies
19 Alzheimer's disease (location of the APO E4 gene) Depression, anxiety, dementia, late onset 21 Progressive myoclonic epilepsy Cognitive regression, aphasia, mental retardation. Alzheimer's disease (associated with Down syndrome) Depression, anxiety, dementia, early onset 22 Metachromatic leukodystrophy Personality changes, psychosis, dementia.
BEHAVIORAL NEUROANATOMY
- The cerebral hemispheres
- The autonomic nervous system, which consists of sympathetic and parasympathetic divisions, innervates the internal organs
Brain lesions caused by accident, disease, surgery, or other insults are associated with distinct neuropsychiatric effects (Table 4-2). Basal ganglia Movement disorders (eg, Parkinson's disease [substantia nigra], Huntington's disease [caudate and putamen], and Tourette syndrome [caudate]) Neuropsychiatric effects of brain lesions on behavior.
NEUROTRANSMISSION
The autonomic nervous system coordinates emotions with visceral responses such as heart rate, blood pressure, and peptic acid secretion. Visceral reactions that occur as a result of psychological stress are involved in the development and exacerbation of some physical diseases (see Chapter 22).
Synapses and neurotransmitters
The changeability of number or affinity of receptors for specific neurotransmitters ( neu- ronal plasticity ) can regulate the responsiveness of neurons
Regulation of neurotransmitter activity
BIOGENIC AMINES
Overview
The monoamine theory of mood disorder hypothesizes that lowered monoamine activity results in depression and elevated levels in mania
Dopamine
Dopaminergic tracts
Dopamine acts on the tuberoinfundibular tract to inhibit the secretion of prolactin from the anterior pituitary. This increase in turn leads to symptoms such as breast enlargement, galactorrhea and sexual dysfunction.
Synthesis
This tract may play a role in the expression of emotions as it projects to the limbic system and prefrontal cortex.
Histamine
Acetylcholine (Ach), a quaternary amine, is the transmitter used by nerve-skeleton-muscle junctions
Degeneration of cholinergic neurons is associated with Alzheimer disease, Down syndrome, and movement and sleep disorders (e.g., decreased REM sleep, see Chapter 10)
Cholinergic neurons synthesize Ach from acetyl coenzyme A and choline using choline acetyltransferase
Blocking the action of AchE with drugs such as donepezil (Aricept), rivastigmine (Exelon), and galantamine (Reminyl) can delay the progression of Alzheimer's disease, but cannot reverse the already lost function. Blockade of muscarinic Ach receptors with drugs such as antipsychotics and tricyclic antidepressants results in the classic "anticholinergic" side effects seen with the use of these drugs, including dry mouth, blurred vision, urinary hesitancy, and constipation.
AMINO ACID NEUROTRANSMITTERS
Glutamate
GABA
NEUROPEPTIDES
Endogenous opioids
Enkephalins , endorphins, dynorphins, and endomorphins are opioids produced by the brain itself that decrease pain and anxiety and have a role in addiction and mood
The area of the brain most likely to be affected in this patient is (are). The answer is E. The patient shows signs of Klüver-Bucy syndrome, which includes hypersexuality and docility and is associated with damage to the amygdala.
OVERVIEW
MEASUREMENT OF BIOGENIC AMINES AND PSYCHOTROPIC DRUGS
Plasma levels of some antipsychotic and antidepressant agents are measured to evaluate patient compliance or to determine whether therapeutic blood levels of the agent have been reached
Lithium levels also should be monitored regularly because of the drug’s narrow therapeutic range (see Chapter 16)
DEXAMETHASONE SUPPRESSION TEST (DST)
TESTS OF ENDOCRINE FUNCTION
Psychiatric symptoms are associated with endocrine and enzyme disorders, such as Addison disease (hypocortisolism), Cushing disease (hypercortisolism), and acute intermittent porphyria
- Addison disease
- Cushing disease
- Acute intermittent porphyria
- NEUROIMAGING AND ELECTROENCEPHALOGRAM STUDIES
- NEUROPSYCHOLOGICAL TESTS
- OTHER TESTS
Evoked EEG (Evoked Potentials) Measures electrical activity in the cortex in response to tactile, auditory, sound or visual stimulation. Used to evaluate vision and hearing loss in infants. Neuropsychological tests are intended to assess general intelligence, memory, reasoning, orientation, perceptuomotor performance, language function, attention, and concentration in patients with suspected neurological problems, such as dementia and brain damage (Table 5-2).
Drug-assisted interview
Sedatives can relax patients with conditions such as dissociative disorder, conversion dis- order (see Chapter 14), and other disorders involving high levels of anxiety and mute psy-
Sodium lactate administration. Intravenous (IV) administration of sodium lactate can provoke a panic attack (see Chapter 13) in susceptible patients and can thus help to identify individu-
FREUD’S THEORIES OF THE MIND
To explain his ideas, Freud developed the topographical theory of mind early in his career and the structural theory later in his career. In the structure theory, the mind contains three parts: the id, the ego, and the superego (Table 6-1).
DEFENSE MECHANISMS
It works closely with the preconscious mind, but has no access to the unconscious mind. The conscious mind uses secondary process thinking (logical, mature, time-oriented) and can delay gratification.
Specific defense mechanisms (Table 6-2)
Repression, pushing unacceptable emotions into the unconscious, is the basic defense mechanism on which all others are based
TRANSFERENCE REACTIONS
Intellectualization Using the higher functions of the mind to avoid A sailor whose boat is about to sink explains in detail the experienced emotional technicalities of the hull damage. Response Adopting opposing attitudes to avoid personal A woman who is unconsciously resentful of the formation of unacceptable emotions, i.e. unconscious responsibilities for raising children, spends too much money.
Transference
HABITUATION AND SENSITIZATION
In habituation (also called desensitization), repeated stimulation results in a reduced response (eg, a child receiving weekly allergy shots cries less and less with each injection). Desensitization, repeated stimulation results in an increased response (eg, a child who is afraid of spiders feels more anxiety every time they encounter a spider).
CLASSICAL CONDITIONING
Response acquisition, extinction, and stimulus generalization
Learned helplessness
An animal receives a series of painful electric shocks from which it is unable to escape
OPERANT CONDITIONING
Principles
Features
The likelihood that a behavior will occur is increased by positive or negative reinforcement and decreased by punishment or extinction (Table 7-1)
Extinction in operant conditioning is the gradual disappearance of a learned behavior when reinforcement (reward) is withheld. Resistance to extinction is the force that prevents behavior from disappearing when a reward is withheld.
Shaping and modeling
OVERVIEW OF PSYCHOLOGICAL TESTING
Types of tests
Individual versus group testing
INTELLIGENCE TESTS
Intelligence and mental age
Intelligence quotient (IQ)
In the absence of brain pathology, an individual's IQ is essentially the same in old age as it was in childhood.
Normal intelligence
Wechsler intelligence tests
Related tests
ACHIEVEMENT TESTS
Uses
Achievement tests evaluate how well an individual has mastered specific subject areas, such as reading and mathematics
Specific achievement tests
PERSONALITY TESTS
Personality tests are used to evaluate psychopathology and personality characteristics and are categorized by whether information is collected objectively or projectively. An objective personality test is based on questions that can be easily scored and statistically analyzed; a projective personality requires the subject to interpret the questions.
PSYCHIATRIC EVALUATION OF THE PATIENT WITH EMOTIONAL SYMPTOMS
Psychiatric history
Orientation, memory, attention, A 55-year-old female patient is oriented to person, place and time and shows normal concentration; cognitive, spatial, memory (cognitive ability), understanding of three-dimensional space (spatial ability) and abstraction abilities; and and can tell you how an apple and an orange are alike (abstraction ability). Describe (mood) and a 35-year-old male patient described feeling "low" and showing less external expression demonstrated (affect) emotions of mood than expected (depressed with limited affect).
The mental status examination and related instruments
Objective rating scales of depression that are commonly used include the Hamilton, Raskin, Zung, and Beck scales
To assess depression in a 54-year-old male patient using a self-report scale, which is the most appropriate test. The most appropriate test for assessing abstract reasoning and problem solving in a 54-year-old female patient is that.
SUBSTANCE ABUSE, DEFINITIONS, EPIDEMIOLOGY, AND DEMOGRAPHICS
While in the emergency room, the patient has a seizure and then develops life-threatening cardiovascular symptoms.
Definitions
Epidemiology and demographics
The use of illegal substances is more common among young adults (18–25 years of age) and is twice as common in males
Most abused substances can be classified categorically as stimulants, sedatives, opioids, or hallucinogens and related agents
STIMULANTS
- The effects of use and withdrawal of these substances can be found in Table 9-
Cocaine
Neurotransmitter associations
Stimulant drugs work primarily by increasing the availability of dopamine (DA)
SEDATIVES
Alcohol
Intoxication
Delirium tremens (“the DTs”)
Barbiturates
Benzodiazepines
OPIOIDS
- Compared to medically used opioids such as morphine and methadone, abused opioids such as heroin are more potent, cross the blood-brain barrier more quickly, have a faster
- In contrast to barbiturate withdrawal, which may be fatal, death from withdrawal of opi- oids is rare unless a serious physical illness is present
Methadone and related agents
HALLUCINOGENS AND RELATED AGENTS
Hallucinogens and related drugs include lysergic acid diethylamide (LSD), phencyclidine (PCP, "angel dust"), cannabis (tetrahydrocannabinol, marijuana, hashish), psilocybin (from mushrooms), mescaline (from cactus), and ketamine ("Special K") . The effects of use and withdrawal from hallucinogens and related drugs can be found in Table 9-5.
Marijuana
Increased availability of serotonin is associated with the effects of some of these agents (eg, LSD). Chronic users experience lung problems associated with smoking and a decrease in motivation ("the amotivational syndrome") characterized by a lack of desire to work and increased apathy.
LSD and PCP
While LSD and PCP both cause altered perception, in contrast to LSD, episodes of violent behavior occur with PCP use
CLINICAL FEATURES OF SUBSTANCE ABUSE
Laboratory findings often can confirm substance use (Table 9-6)
TREATMENT
Drug addiction treatment ranges from withdrawal and peer support groups to drugs that block physical and psychological withdrawal symptoms. Dual-diagnosis or mentally ill-chemically dependent (MICA) patients require treatment for both substance abuse and the comorbid psychiatric illness (e.g., major depression), often in a specialized hospital ward.
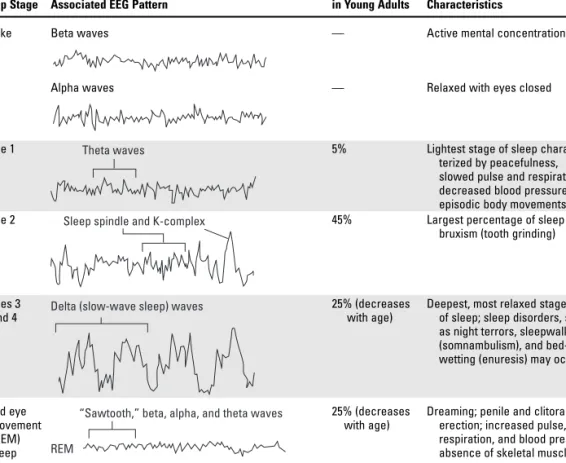
- NORMAL AWAKE AND SLEEP STATES
- Beta waves over the frontal lobes are commonly seen with active mental concentration
- During REM sleep, high levels of brain activity occur
- Increased levels of norepinephrine decrease both sleep efficiency and REM sleep
- CLASSIFICATION OF SLEEP DISORDERS
- These sleep disorders are described in Table 10-3
- INSOMNIA
- Insomnia is difficulty falling asleep or staying asleep that occurs three times per week for at least 1 month, and leads to sleepiness during the day or causes problems fulfilling social or
- Major depressive disorder
- BREATHING-RELATED SLEEP DISORDER (SLEEP APNEA)
- NARCOLEPSY
- TREATMENT OF SLEEP DISORDERS
The increased availability of dopamine is involved in the brain's "reward" system and the euphoric effects of stimulants. Increased levels of acetylcholine (ACh) in the reticular formation increase both sleep efficiency and REM sleep.
- SCHIZOPHRENIA
- Peak age of onset of schizophrenia is 15–25 years for men and 25–35 years for women
- Schizophrenia occurs equally in men and women, all cultures, and all ethnic groups studied
- Symptoms of schizophrenia can be classified as positive or negative
- Prognosis
- Schizophrenia usually involves repeated psychotic episodes and a chronic, downhill course over years. The illness often stabilizes in midlife
- Genetic factors
- Other factors
- Neural pathology 1. Anatomy
- Differential Diagnosis
- Treatment
- OTHER PSYCHOTIC DISORDERS
At the end of the month, the length of her circadian cycle will probably be closest to (A) 21 hours. Of the listed choices, the best treatment for this patient is continuous positive airway pressure (CPAP).
The mood or affective disorders are characterized by a primary disturbance in internal emotional state, causing subjective distress and problems in functioning
The mood states of depression and mania are associated with significant negative consequences for social and occupational functioning. Mood disorders due to a general medical condition and substance-induced mood disorders are secondary mood disorders.
Epidemiology
- CLASSIFICATION OF MOOD DISORDERS
Depression Depressed mood (having feelings of sadness, !!!! . hopelessness, helplessness, low self-esteem and excessive guilt). Psychomotor retardation (slows down) !!. seen especially in the elderly) or agitation (speeding up).
Major depressive disorder 1. Characteristics
- Masked depression
- Seasonal affective disorder (SAD)
- Suicide risk
Perception of serious illness No recent visit (most patients visited a doctor in the six months prior to suicide). SAD is characterized by atypical symptoms of depression (for example, sleeping too much and eating too much) and a feeling of heaviness in the extremities (“lead-like paralysis”).
Bipolar disorder
Unlike patients with hypochondriasis, patients with depression exhibit other symptoms of depression (eg, weight loss, suicidality) in addition to their physical complaints. In some patients (eg, poor patients with low access to health care), a mood disorder with psychotic symptoms may become severe enough to be misdiagnosed as schizophrenia.
Dysthymic disorder and cyclothymic disorder
- Cyclothymic disorder involves periods of hypomania and dysthymia occurring over a 2-year period (1 year in children) with no discrete episodes of illness
- ETIOLOGY
- TREATMENT
- Depression is successfully treated in most patients
- Only about 25% of patients with depression seek and receive treatment
- The most effective treatments for the mood disorders are pharmacologic
- Treatment for depression and dysthymia includes antidepressant agents (e.g., hetero- cyclics, selective serotonin and selective serotonin and norepinephrine reuptake inhibitors
- Mood stabilizers
Lithium and anticonvulsants such as carbamazepine (Tegretol) and divalproex (Depakote) are used to treat bipolar disorder. Mood stabilizers in doses similar to those used to treat bipolar disorder are the primary treatment for cyclothymic disorder.
Psychological treatment
- The symptoms do not respond to antidepressant medications
- ANXIETY DISORDERS
Of the following signs and symptoms this patient is most likely to experience. The answer is D. The sign or symptom most likely to indicate that this patient is experiencing a major depressive episode rather than a normal response to a serious illness is her overwhelming guilt.
Fear and anxiety
The mother of a 4-year-old child with diabetes takes the child to the pediatrician for a "checkup." at least 3 times a week. He watches the child all the time and does not let him play outside.
Classification and occurrence of the anxiety disorders
- The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) classification of anxiety disorders includes
In panic disorder with agoraphobia, the characteristics and symptoms of panic disorder (see above) are associated with fear of open places or situations in which the patient cannot escape or get help (agoraphobia). Panic disorder with agoraphobia is associated with separation anxiety disorder in childhood (see Chapter 15) Phobias (Specific and Social).
The organic basis of anxiety
Treatment of the anxiety disorders
- SOMATOFORM DISORDERS
Characteristics and classification
- Somatoform disorders are characterized by physical symptoms without sufficient organic cause
- Most somatoform disorders are more common in women, although hypochondriasis occurs equally in men and women
Most somatoform disorders are more common in women, although hypochondriasis occurs equally in men and women. The DSM-IV-TR categories of somatoform disorders and their characteristics are listed in Table 13-2.
Differential diagnosis
- The most important differential diagnosis of the somatoform disorders is unidentified organic disease
Hypochondria Excessive worry about health and illness that lasts for at least 6 months Worry persists despite medical assessment and reassurance More common in middle and older age. More common in undemanding adolescents and young adults Patients appear relatively unconcerned (“la belle indifférence”) Body dysmorphic disorder Excessive focus on a minor or imagined physical flaw.
Treatment
- FACTITIOUS DISORDER (FORMERLY MUNCHAUSEN SYNDROME), FACTITIOUS DISORDER BY PROXY,
- COGNITIVE DISORDERS
Which of the following additional signs or symptoms is this patient likely to exhibit? Of the following options, long-term treatment is likely to be the most effective for this patient.
Dementia of the Alzheimer’s type (Alzheimer disease) 1. Diagnosis
- Neurophysiological factors
- PERSONALITY DISORDERS
- Persons with PDs generally are not aware that they are the cause of their own problems ( do not have “insight” ), do not have frank psychotic symptoms, and do not seek psychiatric help
Decreased activity of acetylcholine (Ach) and reduced brain levels of choline acetyltransferase (ie, the enzyme needed to synthesize Ach) are seen in Alzheimer's disease (see Chapter 4). Condition Etiology Clinical example Major manifestations Medical interventions Alzheimer's disease Brain dysfunction A 65-year-old former Severe amnesia Structured environment.
Classification
- DISSOCIATIVE DISORDERS
- The dissociative disorders are characterized by abrupt but temporary loss of memory (amnesia) or identity, or by feelings of detachment owing to psychological factors
Individuals with personality disorders (PD) exhibit chronic, lifelong, rigid, inappropriate patterns of relating to others that cause social and occupational problems (e.g., few friends, strong association with others that cause social and occupational problems (e.g., few friends). People with personality disorders are generally unaware that they are the cause of their own problems (have no 'insight'), have no overt psychotic symptoms and do not seek psychiatric help.have no overt psychotic symptoms and do not seek psychiatric help.
Classification and treatment
- Treatment of the dissociative disorders includes hypnosis and drug-assisted inter- views (see Chapter 5) as well as long-term psychoanalytically oriented psychotherapy
- OBESITY AND EATING DISORDERS
Hallmark: Avoids social relationships, is "special" but not psychotic Genetic or family association: Psychotic illnesses. Attributes responsibility for own problems to others Interprets others' motives as malicious Collects weapons.
Obesity 1. Overview
BMI is calculated by placing a ruler between the weight column (left) and height column (right) and reading BMI from the point where the ruler crosses the BMI column.
Eating disorders: anorexia nervosa and bulimia nervosa
- PERVASIVE DEVELOPMENTAL DISORDERS OF CHILDHOOD
This medical student, who must constantly make lists and review and memorize her notes, is showing evidence of obsessive-compulsive personality disorder. The answer is E. This woman, who has always felt empty and alone (not just lonely), shows evidence of borderline personality disorder.
Autism spectrum disorders (ASD)
- Occurrence of ASD
At home, the child interacts appropriately with his parents and when friends come to visit, he plays well with them. Advise the parents to ignore the school refusal, take the child to school and tell him what time they will pick him up.
Other pervasive developmental disorders 1. Rett disorder involves
- ATTENTION DEFICIT HYPERACTIVITY DISORDER
In contrast to autistic disorder, Asperger's disorder involves normal cognitive development and little or no language development delay. A genetic component (for example, the concordance rate for ASD is three times higher in monozygotic than in dizygotic twins).
AND DISRUPTIVE BEHAVIOR DISORDERS OF CHILDHOOD
Attention deficit hyperactivity disorder (ADHD) and the disruptive behavior disorders (e.g., conduct disorder and oppositional defiant disorder) are characterized by inappropriate
There is no frank mental retardation
These disorders are not uncommon and are seen more often in boys
Differential diagnosis includes mood disorders and anxiety disorders
Etiology
- Pharmacologic treatment for ADHD consists of use of central nervous system (CNS) stimu- lants including methylphenidate (Ritalin, Concerta), dextroamphetamine sulfate
- OTHER DISORDERS OF CHILDHOOD
Although evidence of serious structural problems in the brain is not present, children with conduct disorder and ADHD may have minor brain dysfunction. Family therapy is the most effective treatment for conduct disorder and oppositional defiant disorder (see Chapter 17).
Tourette disorder
- Tourette disorder is characterized by involuntary movements and vocalizations (tics), that may include the involuntary use of profanity (coprolalia). While these behaviors can
- The disorder is three times more common in males and has a strong genetic component
- There is a genetic relationship between Tourette disorder and both ADHD and obsessive- compulsive disorder (see Chapter 13)
Hyperactivity is the first symptom of risk for criminal behavior. A significant number of cases disappear when the child reaches antisocial personality disorder, progresses to conduct disorder. Characteristics and prediction of attention deficit hyperactivity disorder, conduct disorder, and oppositional defiant disorder.
Separation anxiety disorder
- Individuals with a history of separation anxiety disorder in childhood are at greater risk for anxiety disorders in adulthood, particularly agoraphobia
Atypical antipsychotics (e.g., risperidone (Risperdal)) and typical agents (e.g., haloperidol) are the most effective treatments for Tourette's disorder.
Selective mutism
Which of the following is most involved in the etiology of this child's problem. Children with this disorder have little or no concern for others or animals (eg, this child finds torturing animals "fun") (see also answer 4).
Psychopharmacologic agents may also be useful in the treatment of symptoms of certain med- ical conditions (e.g., gastrointestinal problems, pain, seizures)
- ANTIPSYCHOTIC AGENTS
- Traditional antipsychotic agents act primarily by blocking central dopamine-2 (D 2 ) receptors
- Most of the atypical antipsycotics are also indicated to treat bipolar disorder
- ANTIDEPRESSANT AGENTS
- Heterocyclic antidepressants (HCAs), selective serotonin reuptake inhibitors (SSRIs), selec- tive serotonin and norepinephrine reuptake inhibitors (SSNRIs), monoamine oxidase
- While heterocyclics were once the mainstay of treatment, because of their more positive side effect profile, SSRIs (e.g., fluoxetine [Prozac]) are now used as first-line agents
- All antidepressants take about 3–6 weeks to work and all have equal efficacy
Low potency agents (e.g., thioridazine [Mellaril]) are primarily associated with nonneurological side effects (Table 16-1) and are now rarely used as a first-line agent. Atypical antipsychotics (e.g., clozapine (Clozaril), risperidone (Risperdal), olanzapine (Zyprexa), quetiapine (Seroquel), ziprasidone (Geodon), aripiprazole (Abilify), and paliperidone (Invega)).
Heterocyclic Agents
- Heterocyclics are dangerous in overdose
Atypical agents may increase the likelihood of hematological problems, such as agranulocytosis (very low granulocyte count leading to serious infections), with clozapine being the most problematic agent. All antidepressants are believed to increase the availability of serotonin and/or norepinephrine in the synapse via inhibition of reuptake mechanisms (HCAs, SSRIs, SSNRIs) or blockade of MAO (MAOIs), ultimately leading to downregulation of postsynaptic receptors and improvement of mood (see Chapter 4).
SSRIs and SSNRIs
- SSRIs selectively block the reuptake of serotonin only; SSNRIs block the reuptake of both serotonin and norepinephrine
Citalopram (Celexa) More cardiotoxic than other SSRIs Low cytochrome P450 effect Escitalopram (Lexapro) Most serotonin-specific of the SSRIs. Amoxapine (Asendin) Antidopaminergic effects (eg, depression with psychotic features parkinsonian symptoms, galactorrhea, . sexual dysfunction) Most dangerous in overdose.
MAOIs
- MAOIs and SSRIs used together can cause a potentially fatal drug–drug interaction, the serotonin syndrome, (see below)
- The serotonin syndrome
- MOOD STABILIZERS
- Because of potential toxicity, blood levels of lithium must be maintained at 0.8–1.2 mEqL
Anticonvulsants: carbamazepine (Tegretol), oxcarbamazepine (Trileptal), valproic acid (Depak- ene, Depakote), and others
- Anticonvulsants are also used to treat mania, particularly rapid cycling bipolar disorder (i.e., more than four episodes annually), and mixed episodes (mania and depression
- Carbamazepine may be associated with severe adverse effects, such as aplastic anemia and agranulocytosis
- ANTIANXIETY AGENTS
Benzodiazepines (BZs)
Non-benzodiazepines
- ELECTROCONVULSIVE THERAPY
Uses of electroconvulsive therapy (ECT)
Administration
- ECT involves inducing a generalized seizure, lasting 25–60 seconds, by passing an electric current across the brain
Problems associated with ECT
- PSYCHOANALYSIS AND RELATED THERAPIES
- The central strategy of these therapies is to uncover experiences that are repressed in the unconscious mind and integrate them into the person’s conscious mind and personality
Of the following, the most appropriate pharmacologic treatment for this patient is (A) a high-potency antipsychotic agent (B) an anticholinergic agent. C) an anti-anxiety agent (D) an antidepressant agent (E) lithium. This patient who became ill at a pizza party most likely took tranylcypromine, a monoamine oxidase inhibitor (MAOI).
Techniques used to recover repressed experiences include 1. Free association
- BEHAVIORAL THERAPIES
Treatment of phobias (irrational fears). In the past, through the process of classical conditioning (see Chapter 7, see Chapter 13), the person associated an innocuous object with a fearful stimulus. Treatment of Phobias The person is exposed to an actual (flood) or imagined (implosion) overwhelming dose of the feared stimulus.
In contrast to psychoanalysis and related therapies, the person’s history and unconscious conflicts are irrelevant, and thus are not examined in behavioral therapies
- OTHER THERAPIES
The person eventually stops the maladaptive behavior because it automatically provokes an unpleasant response. Through the habituation process (see Chapter 7), the person becomes accustomed to the stimulus and is no longer afraid.
Group therapy
- Groups with therapists
- Leaderless groups
Chronic mental illnesses dealing with ordinary life situations. Interpersonal therapy People with emotional problems due to problems with interpersonal skills. Stress management People with anxiety disorders or stress-related illnesses (eg, headaches, hypertension) Uses of group, family, marital/couple, supportive, interpersonal and stress management therapies.
Family therapy
- Family systems theory
Characteristics of specific behavioral therapies (e.g., systematic desensitization, aversive conditioning, flooding and implosion, symbolic economy, biofeedback, and cognitive/behavioral therapy), flooding and implosion, symbolic economy, biofeedback, and cognitive/behavioral therapy) can be found in Table 17-1. Other therapies include group, family, marital/couple therapy, supportive and interpersonal therapy, as well as stress management techniques.
Supportive and interpersonal therapy
- OVERVIEW OF THE FAMILY
Flooding is a treatment technique for phobias in which a person is exposed to an overwhelming dose of the feared stimulus or situation until he or she is no longer afraid. In flooding, a person is exposed to an overwhelming dose of the feared stimulus or situation—in this case, heights—until he or she is no longer afraid.
Definition
A 70-year-old Mexican American woman, whose husband died 4 months ago, calmly tells her doctor that she and her husband are still communicating. B) "Do other people in your cultural group believe that they can communicate with those who have died?".
Types of families
- DEMOGRAPHICS AND CURRENT TRENDS
Marriage and children
- Approximately 50% of children live in families with two working parents; only about 25%
Which of the following is the most appropriate question or statement from the physician at this time? Percentage of American children living with married parents, single parent, or other in 2001: Distribution by ethnic group.
Divorce and single-parent families
- Close to half of all marriages in the United States end in divorce
- Single-parent families
- Children in single-parent families
- Child custody
- CULTURE IN THE UNITED STATES
The total cost of raising a child in the United States to age 17 is currently over $100,000. Most elderly Americans spend their final years on their own; only about 20% live with relatives and about 5% live in nursing homes.
Culture and illness
Culture shock
- Culture shock is a strong emotional response, which may involve psychiatric symptoms, related to geographic relocation and the need to adapt to unfamiliar social and cultural
- SUBCULTURES
African Americans
- The average income of African American families is only about half that of white families

