I have called Chapter 2 the "ologies" of Primary Health Care because I believe that no single "ology" (be it basic biomedical science, epidemiology, psychology, sociology, anthropology, or philosophy) can alone support primary care practice or research. . In the US in the early 1980s, a single family medicine department in Worcester, Massachusetts, employed more staff than all the primary care and general practice departments in the United Kingdom combined.
Introduction
What is primary (health) care?
This definition reflects some undoubted strengths of primary care: closeness and continuity in the clinician-patient relationship, broad scope of care and anchoring in the wider healthcare system. The general practitioner is increasingly seen as responsible for health at population level.

What is academic study?
Culture, values and identities (including organizational culture, professional culture and so on, as well as the ideas and practices of different ethnic groups) Biomedicine The study of structure and function. Philosophy The study of the nature of knowledge (ontology) and how it is used in practice (epistemology).

What are theories – and why do we need them?
Much of primary care is characterized by disorder, uncertainty, and many different potential approaches to a single problem. You probably also did not understand section 1.2 about the many underlying disciplines in primary care.
The ‘ologies’ (underpinning academic disciplines) of primary health care
Biomedical sciences
It is beyond the scope of this book to give even the briefest outline of the biomedical basis of primary health care. The same can generally be said of the work of physiotherapists, pharmacists, osteopaths and nurses (depending on how the country and healthcare system defines the role of each of these professions).
Epidemiology
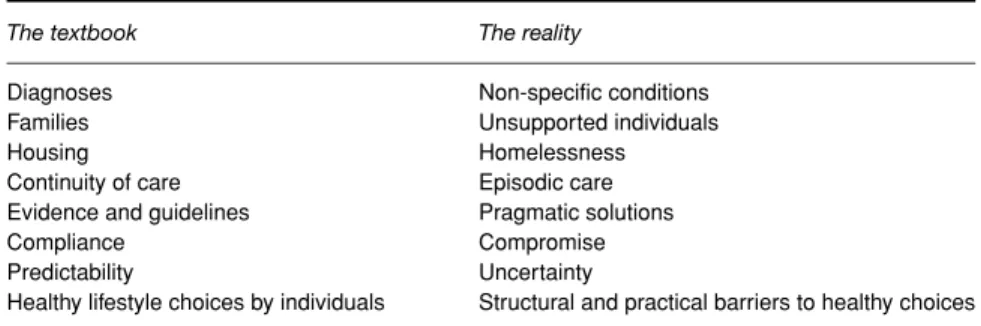
The reality of primary care (see section 1.1, especially the right column of Table 1.2) is that research data on much of its subject matter does not exist (and never will exist) in the form that EBM requires. I will discuss the different types of epidemiological research in section 3.3, and sections and 11.2 all provide examples of the practical and philosophical challenges of delivering the so-called gold standard of 'evidence-based' primary care.

Psychology .1 Overview
Psychological theories generally take the individual as the unit of analysis (see Section 3.9) and offer explanations in terms of rewards and punishments, attitudes and motivation, identity (the 'self' and how it is constructed and represented) or unconscious desires. They are intended to be used as examples rather than as an exhaustive selection of psychology's contribution to the study of primary care.
Sociology .1 Overview
An important branch of clinical psychology is based on moral philosophy (see section 2.7) and is dedicated to supporting and monitoring patient well-being and professional behavior – for example, respect for dignity, responsible care, integrity in relationships and responsibility to the society. Of the hundreds of psychological theories available in the literature, I have mentioned only a few in this book: Prochaska and DiClemente's stages of change theory (also known as the transtheoretical model – section 4.3), Azjen and Fishbein's theory of reasoned action (section 4.3). 4.3), Freud's psychoanalytic theory (see section 6.3), Bandura's social learning theory (which includes the theory of self-efficacy – see section 2.8.1), and Vygotsky's social development theory (see section 2.8.2).
Anthropology
- Structuralist anthropology
- Post-structuralist anthropology
- Symbolic anthropology
Today, the anthropologist's research tools (mostly in-depth qualitative methods) can be used to study one's own culture through self-awareness and distancing techniques designed to "make the familiar strange." In Section 10.3, I discuss how ethnographic observation, a traditional hallmark of anthropology, can be used in a "sociotechnical" study of the impact of electronic patient records.
Literary theory
As Susan Rubin argues in a paper entitled Beyond the authoritative voice, using the patient's own narrative as the starting point for ethical analysis prevents the clinician (or ethicist) from using his or her own perspective and values to decide which are and are not important components of the 'case'. 24. I use literary theory in Section 4.2 when I introduce the work of Arthur Frank on illness narrative; in Section 6.4 when I consider how the work of Bakhtin can illuminate the study of the clinician-patient relationship; and again in Section 11.3 when I consider the significant event audit approach to quality improvement.
Philosophy and ethics
- Epistemology
- Moral philosophy
- Rhetoric and logic
According to Scruton, extreme relativism (like extreme skepticism) is the scoundrel's first refuge. Careful analysis (deconstruction) of texts (including questioning what is not said) will reveal the unspoken and implicit assumptions, ideas and frameworks that form the basis of thought and belief, and will also shift and complicate the obvious (apparent) meaning of the text itself.

Pedagogy
- Experiential learning theory
- Social learning theory
- Social development theory
In fact, both unemployment and high crime rates may have another cause (or rather a determining factor): the state of the national economy. He used a rather strange term for the social interaction that sows the seeds of learning: the Zone of Proximal Development, which he defined as “the distance between the actual level of development as determined by independent people.”

Research methods for primary health care
- What is good research in primary health care?
- Qualitative research
- Quantitative research
- Questionnaire research
- Participatory (‘action’) research
All (or almost all) questions in quantitative research can be expressed in the general format 'What is the chance that. The incidence of multiple sclerosis in the UK is 4 per 100,000 – in other words (on average) in a population.

SOCIAL SITUATION
- Research data – and analysing it
- Critical appraisal of published research papers
- Systematic review
- Multi-level approaches to primary care problems
Incidentally, it is no accident that I have divided the rest of this book primarily according to the main level of analysis of the research presented. What are the most important results, and do they make sense in relation to the research.

The person who is ill
The sick role
A lesser known element of Parsons's work (published later and after criticism of his early work) was a revised concept of the sick role of chronic conditions. Michael Bury linked Parsons' concept of the sick role with the biography of the unfolding illness.

The illness narrative
The presence of the dog is described, with heavy irony, as 'lucky' (a description which I am asked to confirm), presumably because the patient unconsciously seeks to achieve a level of moral order in the story. The dog's effort is symbolic of the effort my patient himself would have made if he only knew that he was needed.
Lifestyle choices and ‘changing behaviour’
Action Actively trying to change Have you really changed (even for a short time) in the last 6 months. Clinicians are rightly cynical about giving lifestyle advice as it is increasingly apparent that patients do not 'obey' the doctor, nurse or pharmacist – they make their own choices which may or may not be influenced by it what the professionals say.

Self-management
Many lay-led self-management programs are modeled on the pioneering work of Kate Lorig and colleagues in the US, whose 'landmark' randomized trial of Arthritis Self-Management Training (ASMP) in 1986 had led to three arms: professional teachers, lay teachers and no training (control). Many so-called lay-led self-management programs are actually professionally supported and directed, but include lay people as peer educators.
Health literacy
Models of how people (and self-help groups and local communities) learn and change, particularly the link between social learning and action (see Section 2.8), could enrich the theoretical basis of the emerging health literacy research tradition. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies in the 21st century.
The primary care clinician
The role of the generalist
General knowledge of any condition, like that of a specialist, is partial and selective. A specialist may be less able than a generalist to manage a common condition that he rarely sees.
Clinical method I: rationalism and Bayes’ theorem
I will return to the "disturbing noise of the patient as a person" in Section 5.3 (on clinical intuition) and in Chapter 6 (on the doctor-patient relationship). Also remember that in primary care we see many patients with mild and often self-limiting disease and many in the very early stages of more severe conditions.
Clinical method II: humanism and intuition
In light of the steroids I admitted him to hospital and the registrar put him on 'observations every four hours'. Another point of view is that clinical work is usually a dialogue, and the patient's input has a great influence on the diagnostic and treatment decisions that are made, as well as on how these are communicated to the patient.
Clinical method III: the patient-centred method
The patient-centered clinical method is the name for an approach that combines both rational, objective reasoning and a humanistic perspective on the patient, as well as taking into account the wider social context that may have caused the illness and brought the patient to the consultation room in the first place. From this short section it is probably clear that there are many possible variations on the theme of the patient-centred method, and that all will involve judicious (rather than formulaic) use of rationalist approaches such as evidence-based medicine. , reflective use of subjectivity and intuition, and consideration of the social causes of illness and counseling behavior.

Influencing clinicians’ behaviour
Based on some 300 observational studies of the adoption (and non-adoption) of various innovations, Rogers has distilled a number of general principles about the properties of innovations – that is, the characteristics that (in the eyes of potential adopters). Important preconditions for adoption are that the intended adopter is aware of the innovation; has sufficient information about what it does and how to use it; and it is clear how the innovation would impact them personally.

The ‘good’ clinician
Furthermore, the qualitative studies have shown that opinion leadership is not static – the question of who influences us and how much changes over time and perhaps even with what mood we are in. The shift from an 'internal' view of professionalism (based on the person's commitment to professional values and codes) to an “external” one (based on accountability to the state and the public and the implementation of formally agreed, approved and measurable standards, as in – but not limited to – clinical governance92–94) also reflects a very different theoretical model of 'the good clinician' (and incidentally a philosophical shift from humanism to objectivism as illustrated in table 2.2, page 47).
The clinical interaction
The clinical interaction I: a psychological perspective Both the doctor–patient relationship, traditionally defined in terms of curing,
The RIAS has been used in over 100 research studies on doctor-patient (and occasionally nurse-patient) communication. Interaction analysis tools are often used in combination with other psychometric instruments – particularly patient satisfaction questionnaires27−29 – which can also be 'quality-assured' against the psychometric dimensions of validity and reliability, and which can serve as an outcome measure. goals in intervention studies to improve the quality of the clinician-patient interaction.

The clinical interaction II: a sociolinguistic perspective A related, but I believe conceptually and theoretically distinct, approach to the
While remarkably few research studies in primary care draw explicitly on symbolic interaction theory, the notion that clinical conversation is imbued with symbolic meaning (and must be studied closely, and in context, to extract this meaning) is central to the study sociolinguistic. of consultation. Mishler uses the notation "L" for the voice of the life world and "M" for the voice of medicine.
The clinical interaction III: a psychodynamic perspective
I want to argue that the instrument in psychotherapy – the counterpart of the surgeon's knife or the radiologist's X-ray machine – is the doctor himself. But Groves did have the insight to note that “the physician's negative responses provide important clinical data that should facilitate better understanding and more appropriate psychological management for all.”
The clinical interaction IV: a literary perspective
In doing so he would have acquired a clinically important datum, at the expense of the trust that we see built up by the subtle exchange of 'uh-huhs' and 'this and that' in the consultation fragment in Box 6.4. This is an example of the use of clinical intuition, which I discuss in more detail in section 5.3.
The interpreted consultation
A profile of communication in telephone consultations with primary care physicians: application of the Roter interaction analysis system. You have to cover up the words of the doctor': the mediation of trust in interpreted consultations in primary care.
The family – or lack of one
Family structure in the late modern world
The overall independent living rate of 30% for people over 60 masks some important subgroup differences. Thirdly, the numerical data mentioned above raise questions about qualitative changes in the nature of society.