Where the work of others was used, this was duly acknowledged in the text. The formation of cataracts, the clouding of the lens of the eye, is the leading cause of blindness in the world. It is estimated that 43% of all blindness is due to cataracts and that 90% of blind people live in Asia or Africa.'
Current surgeries differ in that surgeons remove only the anterior capsule and the nucleus of the lens and replace it with a synthetic lens placed in or on the remaining capsular bag. The natural crystalline convex lens of the eye has an effective power of about +20 diopters'. Since the advent of extracapsular cataract extraction, it has been possible to place an artificial lens in or on top of the remaining lens capsular bag.
In unilateral aphakic eyes, complete spectacle correction is impossible due to the different image sizes.' Because contact lenses are closer to the optical center of the eye, they cause very little magnification and virtually no optical aberrations2. However, the technique is technically difficult because it involves blindly placing fixation sutures through the ciliary sulcus, close to the greater arterial circle of the iris.
The haptic that supports the optics of the lens is located in the corner between the cornea and the iris.
The Artisan®/VerisyseT" Lens
H istory
The lens is also placed in the anterior chamber, similar to the angle-supported lenses, but the haptics attach to the base of the iris. The lens has been shown to allow virtually unlimited pupil dilation (Plate 2) since the lens is attached to the midperipheral immobile iris. Fluorescein angiographic studies showed no leakage of the iris vessels at the enclavation site.
This is in stark contrast to Binkhorst's fixed iris edge lenses which were used in the past and caused uveitis, iris atrophy, glaucoma and corneal decompensation". Two diametrically opposed haptics provide stable fixation and the lens has remained stable 4 years later. trials 14° 15. The predictability of the desired refraction is within I dioptre9 and no patient experienced a decrease in vision corrected with the best glasses.
Minor adverse events in the US Phase III Clinical Trial included postoperative glare (7.7%), iris pigment precipitates (7.2%), and halos (5.3%). The main concern was focused on the proximity of the lens to the endothelial surface of the cornea.
Study Plan
Statistical analysis was carried out by the Department of Biostatistics, University of KwaZulu-Natal. The study was submitted and approved by the Bioethics Board and Postgraduate Committee of the University of KwaZulu-Natal. Subjects were recruited from the eye clinics of the University of KwaZulu-Natal Department of Ophthalmology hospitals.
Black African patients: The study focused on the effects of the Artisan lens on highly pigmented irises. Patient Informed Consent: All patients participating in the study were required to understand and agree to participate in the study. Patients subsequently randomized to the Artisan arm of the study were required to sign a further consent for surgery.
Intraocular pressure > 21 mm (treated) with existing glaucoma: 1 Slight intraocular pressure is a contraindication for intraocular surgery due to the risk of suprachoroidal bleeding. Established but successfully treated glaucomatous eyes were excluded because one of the outcomes examined included intraocular pressure and glaucomatous changes. Pupil width greater than 5 mm under mesopic (moderate light) conditions: The lens has previously been successfully attached to irises with larger pupillary openings, but it was felt that the risk of lens dislocation in the vitreous during surgery was too high for this test.
Significant iris pathology: As we wanted to study the effects of lenses on the iris, eyes were excluded if the author felt that the iris pathology was severe enough. Chronic or recurrent uveitis/iritis: One of the outcomes of the study was chronic inflammation after lens implantation. Information sheets about the trial in English (Appendix A) and IsiZulu approved by the Department of Bioethics were given to each.
Monocular Visual Acuity: Since the purpose of implanting the Artisan lens was to improve vision in the eye, this was the most important measurable outcome. Iris atrophy and pigment dispersion: It was unknown how dark irises responded to direct contact of the Artisan lens clipped onto them. All previous research has demonstrated the stability of endothelial cells after Artisan lens implantation and there should be no reason why corneas in eyes with dark irises would behave differently.
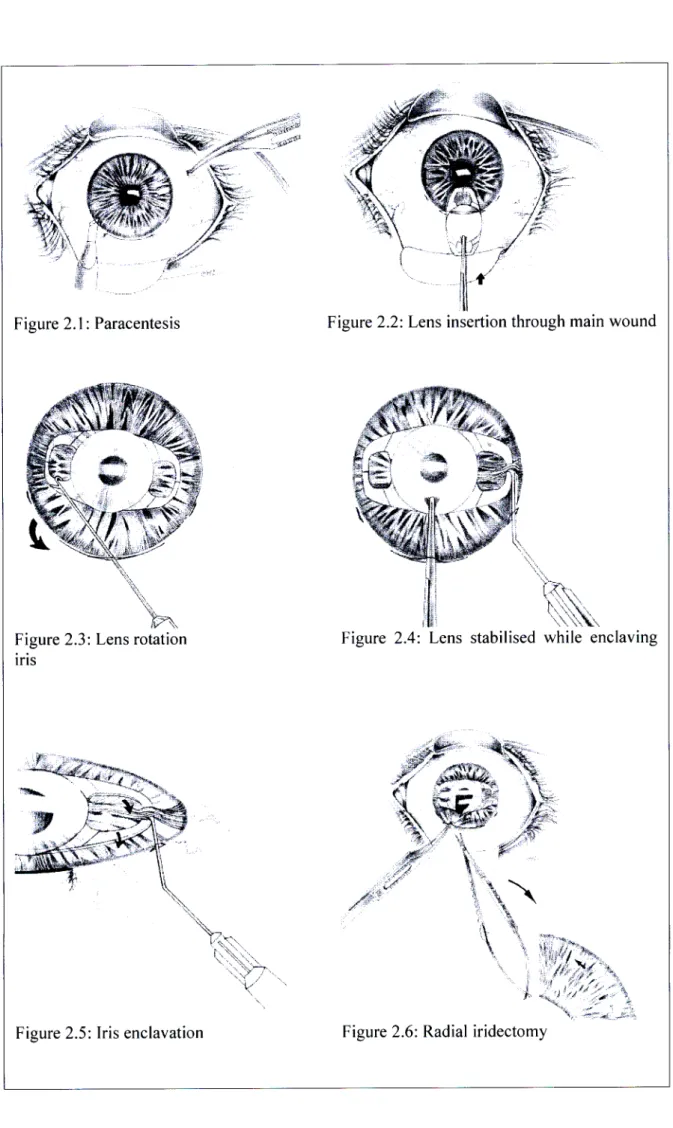
Surgical Procedure
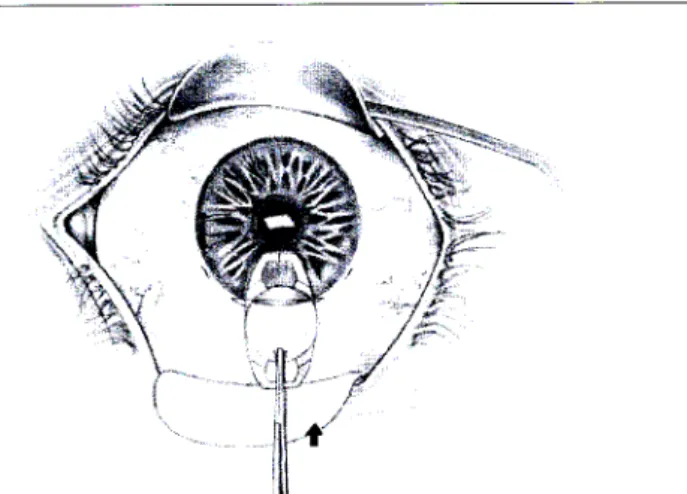
Endothelial cell count: Endothelial cell count equipment is not available in the province of KwaZulu-Natal. The lens was inserted into the anterior chamber (Figure 2.2) and turned into the correct position (Figure 2.3).
Statistical Analysis
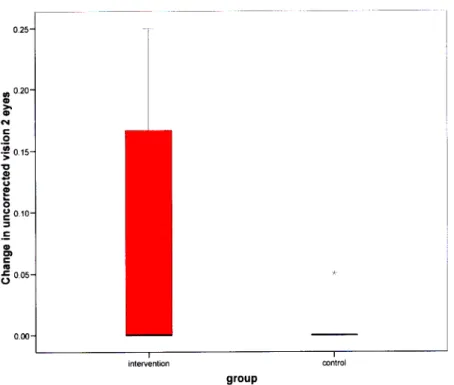
With binocular visual acuity outcome, the expected effect size was a mean decrease of 0.25 MAR in treated relative to control subjects. If control subjects had an expected mean MAR of 3 and SD of 0.4 in both groups, 18 subjects per group (36 in total) would have 83 % power to detect a significant difference between the groups based on the aforementioned assumptions. Monocular visual acuity was expected to increase even more dramatically than binocular visual acuity, so 18 participants per group was considered sufficient for all main outcomes.
Continuous outcomes will be compared between two groups using independent t tests or Mann Whitney tests where appropriate.
Study Termination
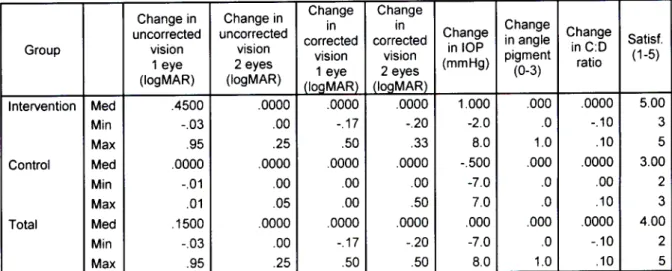
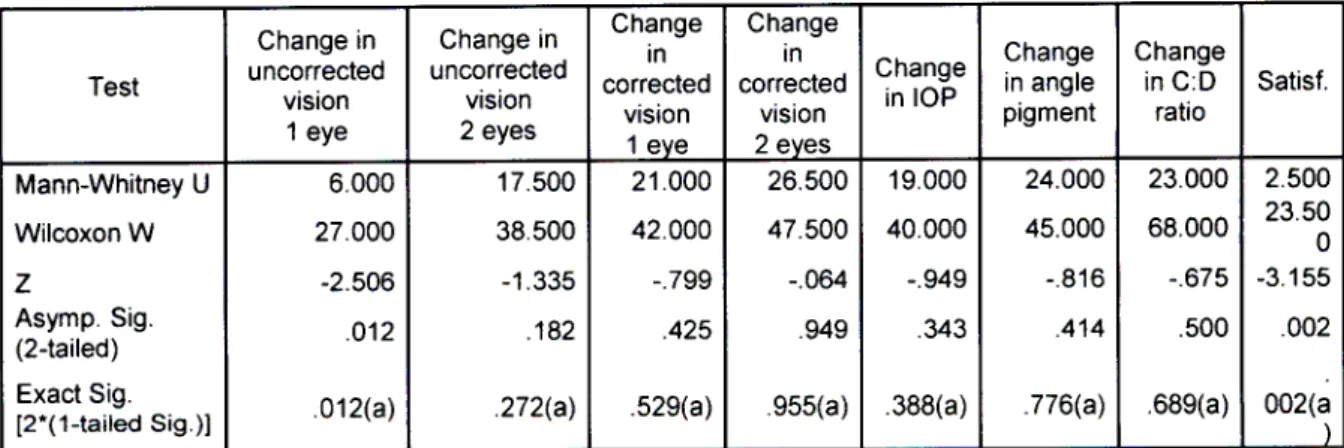
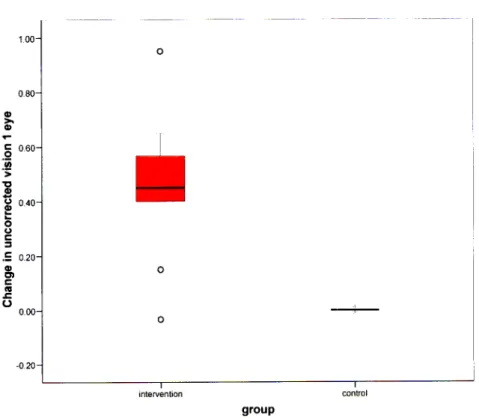
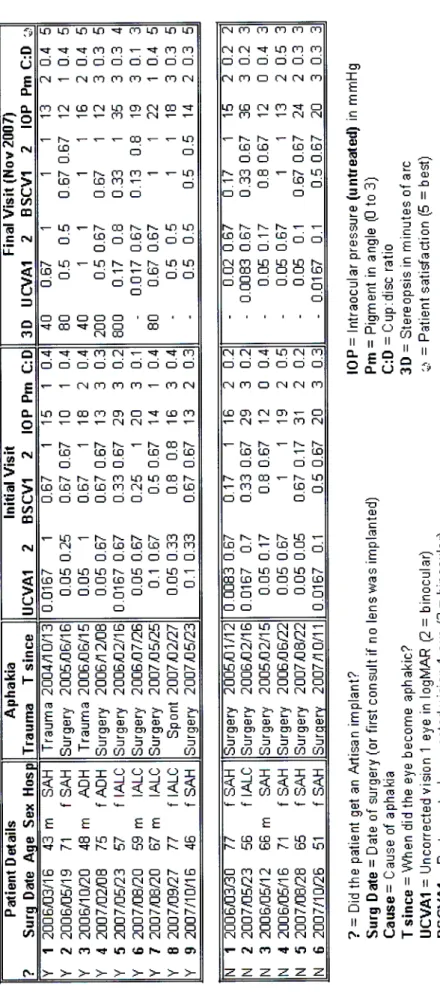
A comparison of the change in final outcomes between the two groups was made (non-parametric Mann-Whitney tests were used due to small sample size) for the major and minor outcomes (Tables 2 and 3). The change in monocular uncorrected visual acuity was significantly higher in the treatment group compared to the control group (p=0.012). Changes in other variables (intraocular pressure, angle pigmentation, change in cup to disc ratio, monocular.
Uncorrected vision was naturally assumed to be higher in the treatment group than in the control group since the control group has a large refractive error. The only reason the treatment group would do the same or worse is if treatment complications prevented good vision. The treatment group had significantly superior uncorrected monocular vision and this was highly statistically significant.
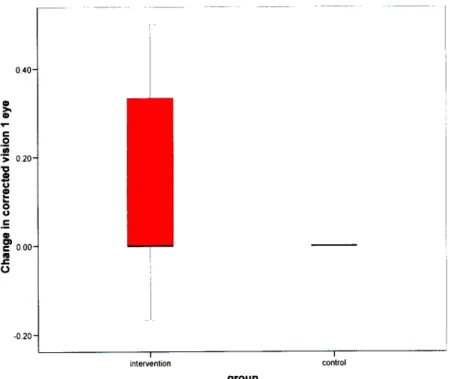
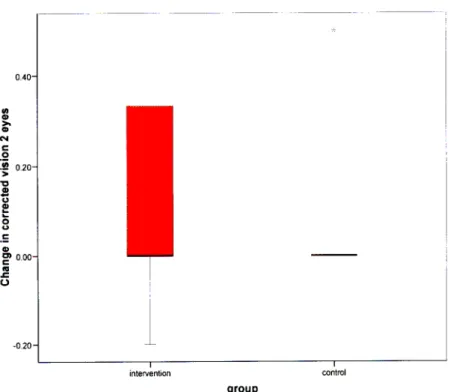
The Artisan group improved by a median of 0.45 logMAR compared to 0 logMAR of the control group. Best spectacle corrected visual acuity (BSCVA) is the best vision that can be achieved with correct refraction with spectacles. Because previous studies with angled lenses in black African patients often caused severe or chronic inflammation in the eye, this was an important aspect to observe.
No patient in the control group and no patient in the treatment group had stereopsis before implantation. This resulted in a pigmented angle and pigment superimposed on other structures in the anterior chamber. Artisan lenses in this study did not appear to cause more angle destruction, increased intraocular pressure, or glaucoma than the control group (Charts 5 and 6).
All of these patients also had elevated 10P at the final visit, but only after discontinuing the drops for several weeks. Thus, the change in 10P and cup were similar in both groups and all hypertension could be successfully treated with Timoptol® (Timolol 0.25%) or Xalatan® (Latanoprost 0.005%). The intervention group had a mean increase of 1013 by 1 mmHg and the control group a decrease of 0.5 mmHg.
The only iris pigment changes observed occurred at the enclavation site (Plate 4) and were most likely caused by trauma to that part of the iris during surgery. Patient satisfaction was very high in the treatment group and reflected the improvement in quality of life and the absence of symptomatic side effects of the implant.
Clinical Interim Interpretation
Study Outcomes
Although the improvement in monocular vision was large, the mean uncorrected vision was only 0.45 IogMAR (=6/l4), which is lower than the expected 1 logMAR (6/6) vision in a normal eye. We thought that the less than perfect vision was due to eye abnormalities caused by the initial insult that caused the aphakia. Worst uncorrected vision in the treatment group after Artisan implantation was only 0.017 IogMAR and corrected to 0.13 logMAR with glasses.
This patient was found to have irregular astigmatism due to a poorly constructed and sutured limbal wound (Plate 6) created during the initial complicated surgery. Although the final visions in the Artisan group were not all 1 logMAR (6/6), these final visions were expected due to the initially poor best spectacle-corrected vision. It was therefore assumed that the increased pressure was due to a pre-existing ocular disease such as pseudoexfoliation (Plate 7).
During the one-year follow-up, the mean disc size remained the same in the treatment group.
Surgery
Study Shortcomings
Although this randomized controlled trial was terminated early, it clearly demonstrated the benefit of implanting Artisan®/VerisyseTM lenses in monocular aphakic eyes without capsule support, even in patients with heavily pigmented irises. Is anterior lens implantation after intracapsular cataract extraction safe in rural black patients in Africa. Budo C, Hessloehl JC, Lzak M, Luyten GPM, Menezo JL, Sener BA, Tassignon MJ, Termote H, Worst JGF.
Information to Patients
I acknowledge that I understand the contents of this form, including the information provided in the Patient Information booklet, and as a subject, I freely consent to the above procedure being performed on me.
Visi are