The staff of the Academy, Ms Boitumelo Mabina (Study Director), Ms Rudzani Ramaite and Dr Xola Mati (Project Director) are acknowledged for their crucial support to the Study Panel. This report is the joint work of a 15-member study panel appointed by the Council of the Academy of Science of South Africa (ASSAf).
Individual sections
A comparison of existing guidelines from the World Health Organization (WHO), the South African Association of HIV Physicians (SAHCS) and the National Department of Health (NDoH) was originally prepared by EV. The key interpretations obtained from the workshop were included in the relevant chapter of the final report.
The Study Panel concludes from its studies that
There are also considerable variations in the nutritional composition of the experimental and control interventions, the use of dietary guidance, disease stage and treatment status of the participants across studies. In light of the findings in the present study, and in accordance with the principles 8.
Concise description of the Brief
Why should this topic be addressed?
It is therefore essential that a thorough review of all the evidence on the issues listed above is carried out by an independent, impartial, multi-disciplinary and authoritative body such as the Academy, in order to transform the relevant national policy framework and public understanding into a productive, effective and efficient direction. The outcome of the study should provide clear guidance on the key issues, and a set of recommendations based on the best evidence and the most integrated understanding of the ways in which nutrition affects people suffering from infections such as tuberculosis and HIV-induced immunodeficiency. states.
Why should the topic be addressed by the Academy and not by another body?
Particularly significant background factors
A preliminary survey of the review literature related to the topic has revealed a paucity of comprehensive, relevant and recent reviews of the topic in the mainstream literature of the relevant disciplines and a relative lack of focus in this area. For example, among approximately 500 review articles in the last 10 years published in the Authoritative Annual Reviews of Nutrition, Immunology, Microbiology, Medicine, and Physiology respectively, not a single article was devoted even indirectly to the subject in question.
Previous efforts and their outcomes
ASSAf will have access to this capability in establishing and supporting a study committee to review the full body of evidence in the area concerned. There are a small number of monographs that cover the nutritional aspects of human immunity in a systematic way, but any search of the literature with relevant keywords produces a large number of articles that do not provide a convincing, conceptually integrated picture regarding the above. the stated short.
International comparisons and similar studies done outside South Africa
The ASSAf Consensus Study should obviously not duplicate the above work or contribute to community confusion in this area. More attention is paid to the functioning of the immune system in relation to iii.
How is the study to be approached?
Design and lay-out
Randomized controlled trials that have evaluated the effects of different nutritional interventions on at least one of the primary outcomes listed below. Outcomes in the secondary category include correlates of morbidity, nutrition or immune function (including nutritional status/markers, markers of altered immune function, efficiency of nutrient absorption, viral load, CD4 count, etc.) recorded and contextually used in the analysis of primary outcomes.
Likely outputs, outcomes and impacts of the proposed study
The ASSAf report should influence public policy in the area of prevention, support and therapy of the now current pandemic infections, such as those with M.tb. This study has investigated the role nutritional support may play in individuals and populations at this time and place against these two pandemic microbial enemies of Homo sapiens in light of the above macro considerations.
Basic science of immunonutrition – basic concepts
Thus, pathogenic organisms are depicted as foreign invaders, with the cells and molecules of the immune cells being cast in the role of "home army soldiers" and their "weapons" respectively. Much of the nutritional need of the immune system relates to the safe supply of chemical energy for this purpose.
Immunopathogenesis of HIV/AIDS and TB – essential concepts
The main reason for this failure is undoubtedly the result of the loss of CD4+ T cells as part of the pathogenesis of HIV infection. Furthermore, the GALT's new focus on HIV infection provides a scenario for failed immune activation that at least contributes to the immunodeficiency state of HIV-infected individuals.
Interpreting Clinical evidence
However, the complexity of the field of nutrition is such that direct evidence to support generalizations is often fraught with confounding circumstances. A consequence of too narrow a definition of population is that the evidence base inevitably becomes proportionately limited, necessitating the application of the process of deduction from the basic science-generated hypothesis in many cases.
Scope of the Consensus Study
The important intersection of nutrition and antiretroviral therapy (ART) has not been addressed in the current Academy of Science of South African consensus study because it has been extensively reviewed recently and was included in the recent World Health Organization Reports on Nutrition and HIV infection . Microbial safety of food, food preservation and/or preparation is not addressed in this report, but food safety has been given considerable attention in the revised national guidelines referred to in the chapter on policy guidelines.
The epidemiology of nutrition in South Africa
Research results from these studies have been compiled by Vorster et al.16 and more recently by Steyn17. The more recent report17, which included studies conducted after 1996, confirmed observations and predictions of future trends from the earlier report16. Both these reports indicate that at a population level, the nutritional status of South Africans is far from optimal. It is therefore not surprising that urbanization of Africans is also associated with an increase in the incidence of many of the chronic diseases of lifestyle.
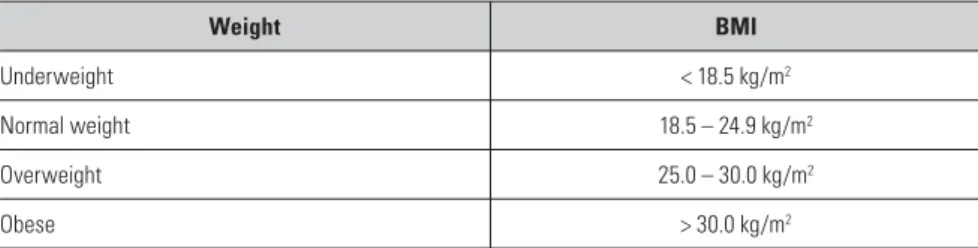
Under- and over-nutrition in South Africans adults: anthropometric data
Therefore, it appears that the nutritional transition among black South Africans is currently characterized by increases in animal protein and fat intake, decreases in carbohydrate and dietary fiber consumption, and improved, but still not optimal, intake of micronutrients. Using BMI as an indicator and combining men and women, less than half of adult South Africans maintain a normal body weight for their height, reflecting imbalances in energy intake and expenditure.
Determinants of nutritional status for malnutrition in South Africans adults
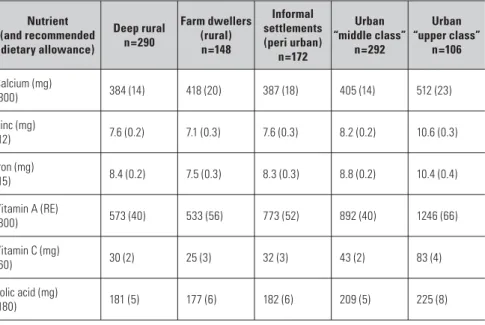
As mentioned earlier, urbanization, modernization, acculturation or westernization of black South Africans is characterized by changing dietary intakes that increase the risk of overweight and obesity without correcting micronutrient malnutrition. However, many South Africans in transition still live in informal settlements in conditions that are not conducive to optimal nutrition18.
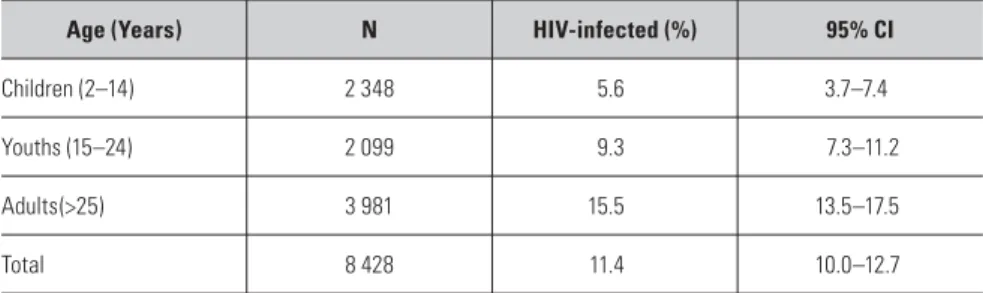
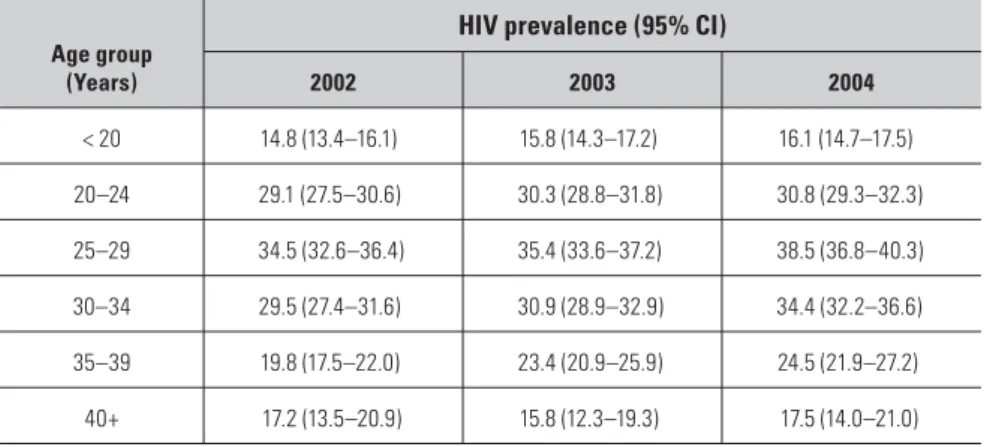
The epidemiology of HIV/AIDS in South Africa
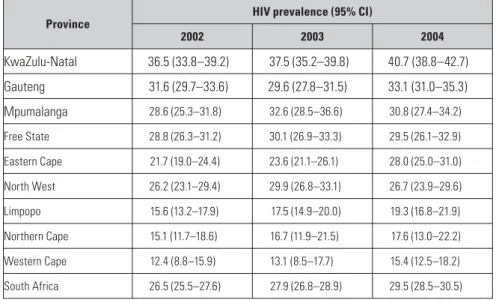
This peak is strongly associated with the increase in HIV seroprevalence observed in antenatal surveys. Disappointingly, however, the rate of HIV infection in this group in SA has remained relatively stable in recent years, perhaps demonstrating a plateau in the number of new infections 24 , 30 .
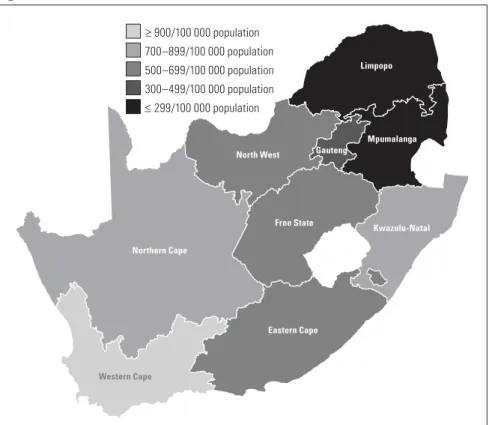
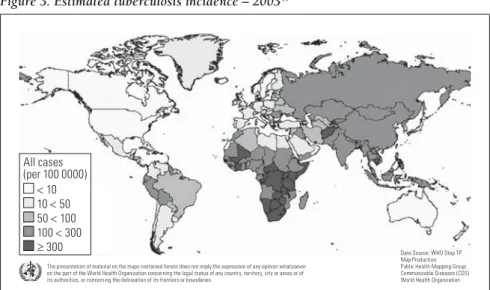
The epidemiology of TB in South Africa
A major reason for the escalation of the TB epidemic in South Africa is the development of the AIDS epidemic. MDR TB is defined as resistance to at least two of the most effective anti-TB drugs, rifampicin and isoniazid.
Introduction
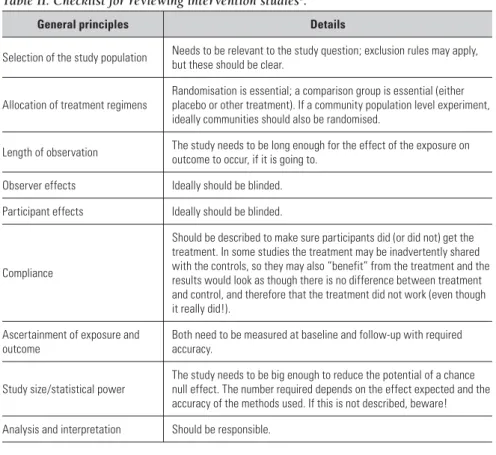
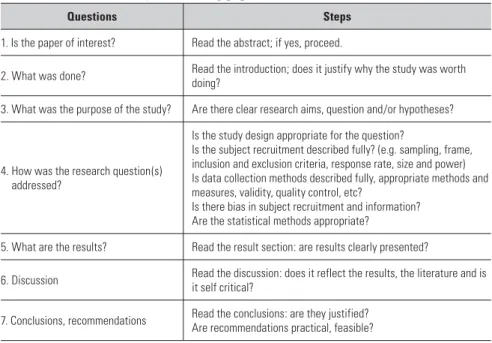
The objectives of this chapter, a narrative review, are primarily to define the concept of scientific, evidence-based policy and practice (evidence-based medicine, nutrition, and/or health practice); second, to briefly discuss the different types of nutritional studies that could and should be considered and used in gathering the available evidence or standard of evidence, indicating both the strengths and weaknesses of such studies; and third, to show how the quality of evidence from different types of sources can be evaluated, assessed and assessed to determine the strength of recommendations for formulating policy and practice.
Evidence-based health policy and practice – definitions
How to search and evaluate or assess the available literature, and how to assess the quality of the evidence, is discussed in the remainder of this chapter. The implementation of this evidence into recommendations for policy and practice is the subject of the final chapter of this document.
Reviewing the literature
Some sources add funding or sponsorship as a final item to these checklists because of the possibility that funding or sponsorship of a particular study may introduce bias, which must be taken into account in the evaluation of studies. Nevertheless, meta-analyses have specific advantages for policy makers, providing a single number summary of the overall estimate of an effect.
Types of nutritional studies
If information on other population characteristics (such as age, sex, income, education, etc.) is collected, the effects of these factors on the exposure-outcome relationship can also be estimated. These factors may be considered more important than the representativeness of the sample.
Evaluation of dietary (nutrient) intake reports
Selection of the study population Must be relevant to the study question; exclusion rules may apply, but these should be clear. The study must be large enough to reduce the potential for a random null effect.
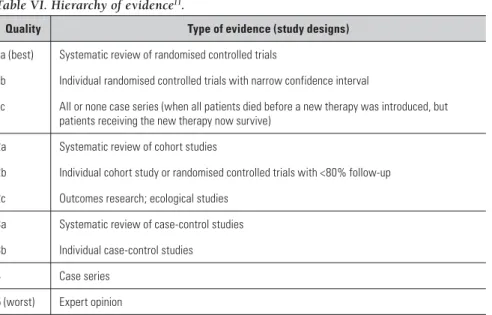
Grading (rating) evidence
- Convincing evidence
- Probable evidence
- Possible evidence
- Insufficient evidence
In rating the scientific evidence "as a basis for dietary recommendations designed to prevent cancer," the panel used uniform methods and terminology. All reasonable alternative explanations for observed associations must be ruled out (that is.. the relationship found specifically for the particular exposure and outcome).
Discussion, conclusions and recommendations
Atkins and colleagues5, part of the GRADE working group, concluded that all of these systems had significant shortcomings. This chapter of the report provides important background information necessary to contextualize the subsequent chapters describing nutritional interventions in persons infected with HIV or affected by clinical tuberculosis.
Food consumption patterns 1 – 5
Because much of the information is the result of many years of a wide range of studies and conceptual contributions, one or a smaller number of general references are cited at the title level for each section or chapter section, rather than compiling a large number of original citations. Obviously, it should be emphasized that nutritional deficiency can arise over time not only from inadequate intake (which itself is variously due to absolute lack of food, the availability of only low-nutritional food, and/or poor appetite), but also from poor food retention (e.g. . in bulimia) or due to poor digestion in the gastrointestinal tract and/or poor absorption from it.
Digestion and absorption of the macro-constituents of foods
Small amounts of fat are used to restore tissue components, such as membrane phospholipids, lost during the body's metabolism. After processing the last meal, adipose tissue releases fatty acids into the blood as the primary fuel for many organs and tissues.
Plasticity of the intestinal tract in macro-nutritional deprivation
Contribution of (large) intestinal bacterial populations to host macro-nutrition
Common disturbances of gastrointestinal function associated with nutritional perturbations
Massive loss of water and accompanying electrolytes, with frequent and urgent watery stools, is usually associated with severe loss of appetite and often with nausea and vomiting; the diet essentially ends, as all or most of the previously ingested food is lost with partially digested products due to severe "gut rush", dysfunctional absorption mechanisms, and temporary suspension of new intake. Mild, occasional but chronic diarrhea is found in subacute diseases of the small and large intestines, liver and pancreas, and also in HIV infections (see Chapter 7).
Whole-body energy metabolism – energy balance
The ingestion, digestion and absorption of a typical mixed meal cause an increase in energy expenditure equivalent to approximately 10% of the kilojoules consumed. Babies and children need energy to synthesize and deposit tissue so that their bodies can grow; in the first months of a person's life, the energy required for growth is approximately 35% of the total energy required by the body.
Activation of the immune system and inflammation
The body will also continue to require energy after the activity has ceased, in proportion to the degree of effort (post-exercise thermogenesis). During prolonged and intense exercise, the body's heat content will increase, mainly due to the inability to lose heat quickly enough.
Energy balance when food intake falls
The body's primary adaptation to starvation is the preferential use of ketone bodies (a byproduct of the rapid and energy-intensive oxidation of fatty acids) instead of glucose; this adaptation halves the rate of body protein loss.
Energy balance in chronic infections
Resting energy expenditure (see above) is an indicator of the body's basal metabolic activity. A number of studies have shown that HIV-infected individuals are not hypermetabolic in terms of total energy expenditure (TEE), although one might expect them to show an increase in TEE as a result of increased resting energy expenditure, this was not the case.
A possible reason to look again at obesity
In HIV infections, resting energy expenditure is expected to be elevated due to increased cytokines associated with ongoing viral replication activity, as well as increased protein turnover and de novo hepatic lipogenesis. A recent meta-analysis examining resting energy expenditure in HIV-infected subjects found that resting energy expenditure per kg of fat-free mass (REE/FFM) was significantly higher (~11%) in subjects infected with HIV than in healthy HIV-negative controls19.
Micronutrients: Vitamins 20
Such alleles may be systematically associated with different rates of gene transcription in different challenge situations if the substitution is in the promoter region; alternatively, there may be a structural (and functional) difference between the products of the alternative genes. Since dietary intake is a primary determinant of whether a state of vitamin deficiency may develop in any person, the stability of the vitamins present in the food before it is eaten is important.
Vitamin requirements
Assessment of vitamin deficiency status of individuals and populations 20, 22
Another confound in laboratory measurements to assess the nutritional value of many vitamins is the fact that vitamin-derived coenzymes are present in normal working tissues and organs as a certain optimal percentage of the relevant cell mass. While major tissue components are broken down into small molecules and redistributed to the cells and tissues they need to defend the body (eg glutamine from protein catabolism for energy production in lymphocytes and fatty acids for energy production in bodies that show an increased metabolic rate ), the excess of compounds derived from vitamins that are released by "reducing" tissue mass is mostly lost from the body through urine, sweat, and feces.
Food-derived vitamins versus synthetic (single or multiple) supplements
In HIV-infected subjects, all plasma concentrations and partial and absolute synthetic rates of various positive APPs were increased, but the plasma concentration of negative APPs was not consistently reduced and the overall patterns were similar to those in other chronic viral infections25 (see Chapter 5). While this is happening, the concentrations of vitamins and metabolites in the body fluids may not reflect the "real" ones.
Micronutrients: inorganic elements 26
Assessment of nutritional status with respect to inorganic micronutrients
The "acute phase" of infections (systemic "inflammation"), as in the case of several vitamins, involves disturbances in the relative concentrations of plasma proteins and tissue catabolism, which can lead to the collection of data related to certain metals or other inorganic elements that are misleading. in terms of the "true" nutritional status of the persons concerned. Genetic microheterogeneity in the complex systems responsible for handling inorganic micronutrients is likely to prevail in human populations, although little is known about this factor other than the dominant genetic conditions of iron overload, which have been well defined.
Specific effects of some vitamins and inorganic micronutrients on human immunity
The physiological role of this trace element (Se) is to become part of a number of important enzymes in the form of active site-located selenocysteine
Incorporation of these particular residues occurs through a specific process and is encoded in the mRNA for the enzyme in question. Many body proteins also contain selenium in the form of selenomethionine and selenocysteine, which are incorporated into methionine- and cysteine-encoded sites by simple, concentration-dependent competition with these unselenated residues; these selenoamino acids, being more abundant, are the main natural source of selenium in the diet. After digestion, some of this selenium is made available (in a highly regulated demand/supply mechanism) for the important functional involvement of selenocysteine in the enzymes mentioned above. .
Some additional relevant topics in human immunonutrition
The nutritionally essential sulfur-containing amino acids methionine and cysteine/cystine, which are released during muscle protein breakdown, play a modulatory role in the coordinated antioxidant defense after infection, in part through their role in the generation of the major intracellular reducing agent, glutathione49. Urinary sulfur loss resulting from intensive metabolism of these amino acids is increased in infected individuals in states of systemic "inflammation", but less than nitrogen loss, as they are conserved due to their important roles in various defense mechanisms.
Overall design of the defences against pathogenic organisms 1–4
To overcome these pathogens, the body must kill them en masse, remove the resulting debris, and restore the affected tissue architecture through healing.
Innate immune responses 4
Coating certain bacteria (usually of the so-called Gram-negative variety) with C3b also releases the complement membrane attack complex (C5b and C6–9) that causes lysis of the walls and death of the bacteria in question. One of the APP is C-reactive protein (CRP), which is an efficient initiator of the alternative complement activation pathway briefly described above, and which also appears to be present at elevated levels in chronic viral infections such as HIV10.
Adaptive (acquired) immunity
Mast cells and platelets contribute to these very early changes at the site, as described above; among the drugs that work at different times are histamine, various prostaglandins and leukotrienes. Some in the latter group will retain the memory of the specific invasion, as memory cells, and will be able to mount a rapid and powerful adaptive immune response if the same pathogen is encountered again.
Anatomical arrangement of the inductive immune system
The lymph node microenvironment allows B and T cells to present whole or parts of invading pathogens (see below for presentation mechanisms involving antigen-presenting cells), ensuring that the inductive phase of immune responses can occur and active, specifically generated targeted effector B and T cells of both the CD4+ and CD8+ series. Some cells are also equipped with "homing signals" that will ensure their collection in certain tissues, such as the lamina propria in the lining of the gut (see below). Disturbances in the structure of lymphoid tissue (gradually occurring, for example, in HIV-infected individuals) affect the way in which B and T cells can prepare to deal with new invading pathogens.
Effector functions of immune cells
The T-cell stimulation also allows affinity maturation to occur, so that the antibodies formed at the peak of the infection and "remembered" in memory cells are most effective. However, in chronic infections such as HIV and tuberculosis, the effector CTLs fail to clear the body of the infecting organism and gradually decrease in number and effectiveness – they become exhausted.
The “hormones” of immunity, acting locally and systemically 9, 19
However, some survive and continue to live as CD62+ memory cells, which can grow into a proliferating population of specifically targeted effector cells once the offending antigen/pathogen is re-encountered in the body. A surface protein called PD-1 accumulates under these conditions and responds to a circulating cytokine PD-1L to produce the 'exhausted' phenotype.
Biomarkers of immune function for nutritional studies and interventions in human subjects
Technical confounding factors were identified as study design, sample collection times (circadian rhythm), seasonal variations, meal and/or exhaustive washout periods, and the length of the intervention period. The question of lifelong programming of the immune system by fetal or perinatal experience.
The issue of life-long programming of the immune system by fetal or perinatal experience
In this chapter, the current understanding of the critical steps in the pathogenesis of pulmonary TB will be reviewed. There are many strains of the organism distributed in different geographic regions, and useful genetic markers have been developed to detect local infection patterns3.
Susceptibility to active TB varies in the human population
Remarkable progress has been made since that time in elucidating the mechanisms by which Mycobacterium tuberculosis causes human disease1, 2. As more such factors are expected to be discovered, the likely genetic heterogeneity of populations used to study nutritional interventions must be taken into account are in study designs.
Pulmonary TB
After induction and expansion of CD4+ Th1 effector cell populations in the pulmonary lymph nodes, these effector cells leave the nodes and home to the inflamed sites of active infection in the lungs and other tissues. Successful modulation of the intense inflammatory response in the granulomas with anti-inflammatory cytokines such as TGF-α and IL-10 allows the host to control mycobacterial replication without compromising lung function.
HIV-1 infection of cells of the human immune system 1
Other proteins formed by cleavage of the primary polyprotein are either packaged with the virus RNA molecules into released virions (e.g. reverse transcriptase) or remain in the infected cell as "viral support agents" (protein helper), primarily working to evade host immunity. attack in different ways. The subtypes of HLA molecules that through their presence prevent cell destruction by NK cells (see Chapter 4) are not affected, so the chances of infected cells to avoid killing by the main killer cells of innate and adaptive immunity are greatly increased.
Early events in a typical HIV infection (vaginal route) 3
The RNA molecules of the virus are the messenger RNAs themselves, each of which is translated by the host's ribosomes into polyproteins, which are then neatly and specifically cleaved by a specific protease derived from the virus to form a set of proteins , including gp120 and its stem protein gp41, which polymerize to form studs on the surfaces of new virions after each has been fully assembled through release from the cell membrane, taking parts of the latter with it. One of these ways is to reduce the amount of specific subtypes of HLA class I molecules on cell surfaces, effectively attenuating the signal indicative of virus infection normally associated with peptide fragments presented to targeting CTLs (" hunt ”) cells presenting those epitopes.
The immune response to HIV infection
Direct killing of CCR5+ CD4+ T cells within the gut12, 13 and memory CD4+ T cells in multiple tissues14 by HIV has been postulated as the primary mechanism for depletion of these cells during SIV infection in monkeys. This situation also applies to the depletion of CD4+ cells caused by HIV in the human intestine15.
The micro-evolution of HIV in a single human body 30
Virus subpopulations capable of infecting new hosts appear to be more susceptible to neutralizing antibodies in vitro than the dominant populations in the infected donor, but subsequent mutational changes in the virus in its new host largely negate this factor 29 . Thus, vaccination-derived neutralizing antibodies may in principle be important for preventing viral infection, but the antibodies are relatively ineffective in combating new HIV infection once it occurs.
Humans are differentially susceptible to HIV infection and its rate of progression 32
Originally, it was thought that HIV directly killed CD4+ T cells, which caused the loss. This is controversial; however, because there was always much more virus detectable than the actual number of HIV-infected CD4+ cells or the percentage of infected CD4+ cells in the blood.
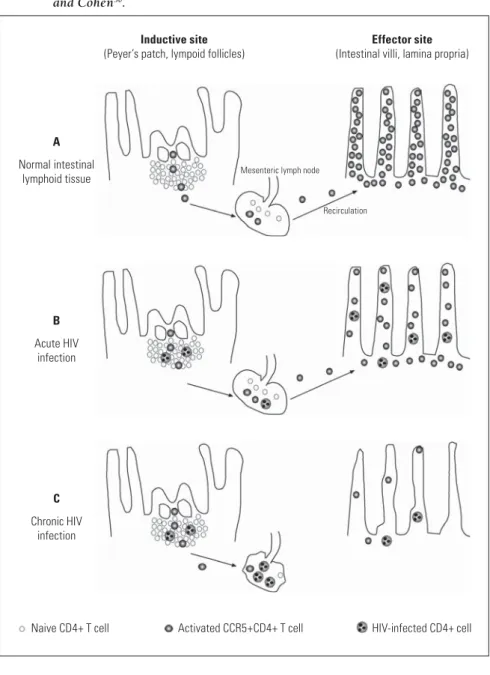
HIV infection and changes in gut-associated lymphoid tissue (GALT)
That this is a constant 'battlefield' is evident from the fact that the effector arm of the immune system is extensively distributed throughout the submucosal space of the entire intestine, in the lamina propria. In this way, almost two-thirds of the body's entire immune system is defensively arranged along the entire intestinal wall36.
GALT events and progression of HIV infection
One of the main functions of the intestinal immune system is therefore to distinguish between harmful and harmless/beneficial organisms and antigens on the part of the host body. The effector cells eventually "home" to the lamina propria of the gut, where the B cells secrete IgA and IgM antibodies, and engage the CD4+ and CD8+ T cells with such organisms and antigens as may have succeeded in entering the submucosa. to urge
A synthesis of HIV infection and impaired intestinal immunity
This is a key concept for understanding the role of memory T cells in chronic HIV infection and in the context of associated intestinal disorders and nutrition (see below). Nutritional deficiencies may play a role in the pathogenesis of HIV infection, in part due to the role of some micronutrients as antioxidants and/or in immune function (see Chapter 7).
Nutrition, infection and immunity in infants and children
The pathogenesis of HIV infection may depend on both virological factors (viral strain and phenotype) and host factors (genetic and nutritional).
Breast-feeding and mucosal/adaptive immunity 7
Passive immune protection provided by residual maternal antibodies (lost by catabolism in the first two months) is key to protecting the newborn infant at this stage. Colonization of the gut by microbial flora contributes greatly to the development of well-functioning gut-associated lymphoid tissues.
HIV acquisition in infants and children
Infants become highly dependent on breastfeeding after loss of the mother's IgG stock, particularly the rich supply of secretory IgA (SIgA) and IgM (SIgM) (12g/l and 0.6g/l respectively in colostrum, and about a quarter of this) in breast milk). Small numbers of immune cells of various types are also secreted in breast milk and may play a role in the immune stabilization of the intestinal mucosa of the infant, possibly by secreting cytokines, some of which are present in the secreted milk, along with growth factors.
Role of nutrition in MTCT
Role of breast-feeding in HIV transmission
The risk of transmission through breastfeeding depends on the age of complete cessation of breastfeeding, the stage of the mother's disease, the health of the breast and the way of feeding. In the International Breastfeeding and HIV Transmission Study (BHITS), 42% of HIV-infected children were infected through breastfeeding by the time they reached 4 weeks of age38.
Factors affecting disease progression in children
Vitamin A plays a central role in children in the growth and function of T and B cells, antibody responses and maintenance of mucosal epithelia, including those of the respiratory, gastrointestinal and genitourinary tracts46. Zinc plays an important role in the growth and development and function of neutrophils, macrophages, natural killer cells and T and B lymphocytes47.
The effects of infant feeding on survival
Vitamin E affects the function of T cells, B cells and phagocytic cells, and may also protect immune effector cells against oxidative stress48. Vitamin B649, selenium50 and folate51 may also affect immune function, but further work is needed on the role of these micronutrients in the pathophysiology of pediatric HIV infection (see Chapter 4).
Infant feeding in the context of HIV
In a study conducted in Soweto19 among a population of HIV-infected mothers, 2.2% of all breastfed infants and 3.8% of all formula-fed infants died before 12 weeks of age (no statistical difference). The infant mortality rate for breastfed babies was also half that of formula-fed babies.
Natural history of paediatric HIV infection
A pooled analysis from Africa found that by one year of age, 35.2% of HIV-infected children and 4.9% of HIV-exposed but uninfected children had died66. Data on the survival of HIV-infected children in South Africa are available from detailed birth cohort studies.
The role of nutrition in childhood HIV infection
In Malawi, the death rate per 1000 person-years of observation in HIV-infected children was 339.3 compared to 46.3 among uninfected children born to HIV-infected women62. Newborns born to HIV-infected women had an increased mortality rate compared to newborns born to uninfected women (40/1000) in Abidjan64, and a reduced 12-month survival rate in Brazzaville65.
Mechanisms for malnutrition in HIV-infected children
Psychosocial factors96–98 may also contribute to malnutrition in HIV-infected children, who often live with ill parents or elderly relatives with limited access to social services and support. An unstable home environment and inadequate emotional and social support have been shown to negatively affect growth in both HIV-infected and uninfected children through many mechanisms, including growth hormone deficiency.
Growth patterns in HIV-infected children 99–115
Infected children born to HIV-infected women have early and persistent stunting and are malnourished but not wasted. A study conducted in Cape Town prospectively examined the anthropometric and micronutrient indicators of 60 stable, HIV-infected children (mean age 25 months) in an economically deprived setting115.
The effects of tuberculosis on HIV infection 116–134
In a study conducted in clinics in Johannesburg and Cape Town, the overall incidence of TB among HIV-infected children was found to be 3.2/100 person-years (95% CI 2.0–4.9). Tuberculosis was the second most common pathology in children dying between 12 and 17 months and was identified in 31.6% and 36.8% of HIV-infected and uninfected children, respectively.
Background
In this chapter we review the evidence from human studies on the effects of nutritional intervention on clinical outcomes in HIV-infected people. We emphasize findings from randomized controlled trials, as these provide the most reliable evidence on treatment effects, emphasizing other types of studies where relevant (See Chapter 3: Evidence-based policy and recommendations).
HIV-associated weight loss and wasting
Whole body protein turnover is up to 25% higher in untreated HIV-infected individuals than in HIV-negative controls4. Nevertheless, if TEE decreases, or at least does not change, the cause of the weight loss and wasting in HIV-infected people requires explanation.
Nutrition and immunity in HIV-infected individuals
Malabsorption and diarrhea, secondary to disruption of intestinal architecture and function, are also frequently encountered in people with HIV infection (see Chapter 7). These individuals may further decrease food intake to minimize the episodes and severity of diarrhea14, 15.
Evidence for the benefits of macronutrient supplementation
Randomised, placebo-controlled trials
The generalizability of the Cochrane review findings to subjects in developing countries should also be considered with caution. Two randomized, placebo-controlled trials that did not meet the inclusion criteria of the Cochrane Review investigated the effect of specific amino acid supplementation on immune parameters of HIV-infected individuals21, 22.
Controlled trials with active controls
No significant change in body weight was observed in any of the participants in either study. No change in immune or viral parameters was observed in any of the groups at six months34.
Intervention trials without controls
Fifty-six percent of children achieved 100% weight-for-height (based on weight-for-height Z-score norms, based on the child's height at admission), with those fed ready-to-use therapeutic foods gaining weight faster. gained weight and became significantly heavier. more likely to reach 100%. In a previous quasi-randomized, controlled trial, imported and locally produced ready-to-eat therapeutic foods were comparably effective in treating severe malnutrition (weight-for-height Z-score: ± −2.1 to −2.2) in HIV-infected people (N= 78) and uninfected children (N=182)32.
Cross-sectional studies
Four of the five participants who lost weight developed secondary infections after enrolling in the study. In a group of HIV-infected outpatients (N=54) who received intensive oral nutrition intervention, weight maintenance and weight gain were achieved in 57% and 33% of the group, respectively40.
Cohort studies
Conclusions and recommendations
Supplementation with a complete protein diet has been found to increase body weight and fat-free mass in HIV-infected adults. Among children under 5 living in developing countries, malnutrition is associated with half of the 10.8 million deaths caused mainly by neonatal disorders, diarrhoea, pneumonia, malaria and HIV/AIDS2.
Importance of micronutrients in general
More than 60% of the estimated 43 million people with HIV/AIDS worldwide live in sub-Saharan Africa, where poverty, social insecurity, food shortages and malnutrition are major problems. AIDS and discusses recent research findings that may have important public health implications for managing the HIV/AIDS pandemic.
Micronutrients and HIV/AIDS
Vitamin A deficiency has been associated with increased morbidity and mortality in children21, increased mother-to-child transmission of HIV-122 and subsequent infant mortality23, and increased mortality in HIV-infected injecting drug users24. Zinc deficiency was associated with increased mortality in a cohort of HIV-infected American men26.
Effects of micronutrients supplemented in HIV/AIDS
Zinc supplementation for 6 months in a randomized trial of 120 HIV-infected children in Durban, South Africa was safe and reduced the incidence of acute diarrhea detected during clinic visits (RR = 0.51; p = 0.001)54. In another trial among HIV-infected South African children in Cape Town, 3 mg zinc daily for 6 months reduced the frequency of acute respiratory infections and episodes of diarrhea.
Potential adverse effects of micronutrient supplements
Vitamin A may increase the risk of vertical transmission in HIV-infected pregnant and lactating women, and the risk of mortality in infants of completed mother-child pairs. HIV-infected pregnant women reduce the risk of disease progression, AIDS-related mortality, and adverse pregnancy outcomes.
Tuberculosis causes malnutrition
Although less well studied, the consequences of the availability to the pathogen of other essential nutrients in a malnourished individual may provide a non-immunological mechanism by which nutritional deficiencies alter the progression from infection to disease in TB. Another way in which nutritional deficiencies can affect TB is by interfering with appropriate chemotherapy in diseased individuals.
Ecological studies
Tuberculosis morbidity has fallen to the prevailing level for free-living young adults in the same population34. Finally, McKeown suggested that the decline in TB deaths in England and Wales from 1770 to 1900 was probably due to the improvement in the nutritional status of the population36.
Case series
During most of the First World War, neutral Denmark exported the bulk of its meat, fish, poultry and dairy products to the extent that the local diet suffered. In the malnourished prisoners, the onset of the disease was faster, the clinical course was more severe and mortality was common35.
Cross-sectional and case-control studies
In addition, several studies have identified genetic polymorphisms of vitamin D receptors that are associated with vitamin D deficiency and increased incidence of tuberculosis. Increased vitamin C and fruit and vegetable intake was associated with an adjusted relative risk for tuberculosis of 0.4 (95% confidence interval 0.2–0.7).
Intervention trials
The percentage of patients with cough was significantly (p<0.05) reduced in the arginine-supplemented group (25%) compared to the placebo group (65%). The percentage of patients with negative sputum smears was significantly higher in patients receiving the supplement (100%) compared to the placebo group (85%) (p<0.05).
Nutritional deficiencies and TB chemotherapy – a bidirectional interaction
Respiratory symptoms improved in both groups: however, the sterilization rate of sputum cultures increased significantly and saliva production decreased significantly in patients consuming a high-cholesterol diet. In the absence of vitamin B6 supplementation, a significant proportion of TB patients treated with INH-containing regimens will experience peripheral neuritis, especially persons predisposed to peripheral neuropathy such as those with diabetes and those who consume excessive alcohol113.
Nutritional deficiencies interfere with the protective efficacy of BCG vaccine