The influence of malnutrition on the prevalence, frequency and duration of chemotoxicity in South African children with nephroblastoma has not been well studied. To determine the influence of malnutrition measured using specific anthropometric and biochemical parameters on the occurrence of chemotoxicity.
INTRODUCTION, THE PROBLEM AND ITS SETTING
- Importance of the study
- Statement of the problem
- Research objectives The objectives of this study were
- Hypotheses
- Study parameters
- Assumptions
- Definition of terms
- Summary
- Dissertation outline
- Referencing style
Mid-upper arm circumference – The circumference of the arm measured halfway between the acromion and olecranon process on the non-dominant side of the body and used to define nutritional status (Murphy, White & Davies 2009). Triceps skinfold thickness – The skinfold measured at the midway point between the acromion and olecranon process on the non-dominant side of the body and is used to define nutritional status (Murphy et al 2009).
REVIEW OF THE RELATED LITERATURE
Nephroblastoma in children
- Global and local incidence of nephroblastoma
- Diagnosis of nephroblastoma
- Medical and clinical management of nephroblastoma
- Changes in nutritional requirements of children with nephroblastoma
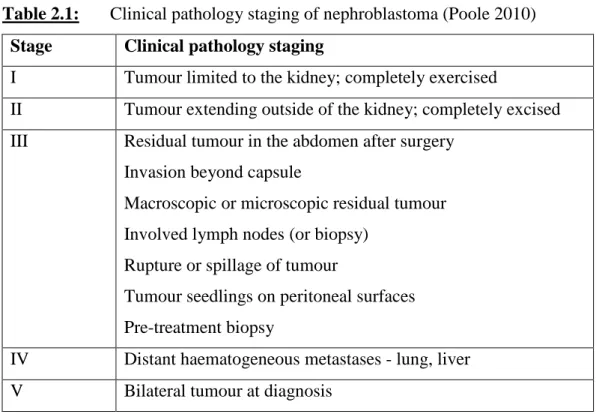
Treatment of nephroblastoma is based on the surgical stage and histological evaluation of the tumor (Poole 2010). II Tumor spreading outside the kidney; completely excised III Residual tumor in the abdomen after surgery.
Nutritional status of children with nephroblastoma
- Assessment of nutritional status
- Anthropometric measures used to assess nutritional status
- Biochemical markers used to assess nutritional status
- Prevalence of malnutrition in children with cancer
- Consequences of malnutrition in children with cancer
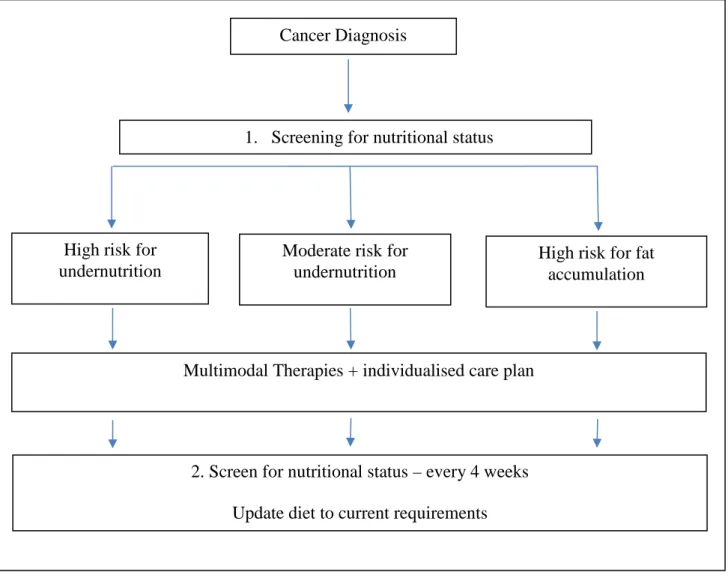
- Nutritional management of malnutrition in children with cancer
The expected need for nutritional support of children with cancer is based on the nutritional status at diagnosis. The mass of a tumor does not affect arm anthropometry, making it an ideal tool for assessing nutritional status in children with cancer (Smith et al 1991). Biochemical values can be used to help estimate nutritional status in children with cancer (Mosby et al 2009).
Two studies, one by Donaldson et al (1981) and one by Elhasid, Laor, Lischinsky, Postovsky & Arush (1999), both assessed the relationship between nutritional status and serum albumin at admission in children with cancer and children with solid tumours, respectively. . However, Elhasid et al (1999) found that pre-albumin on admission and throughout chemotherapy was a good marker to evaluate the nutritional status of children with solid tumors. As a result, the prevalence of malnutrition in children with cancer has been reported to range from common to non-existent at diagnosis.
The prevalence of malnutrition at diagnosis in children newly diagnosed with cancer presenting to a pediatric oncology ward in Morocco was comprehensively assessed. Now that the assessment of malnutrition and the prevalence of malnutrition in children with cancer have been described, the consequences and management of malnutrition are discussed next. Malnutrition in children with cancer is an under-researched topic within pediatric oncology and should not be accepted at any stage of the disease or accepted as an inevitable process.
Chemotoxicity in children with cancer
The success of an enteral nutrition program for children with nephroblastoma is influenced by several factors, including nutritional status at diagnosis, treatment protocol, stage of treatment, and tumor response (Rickard et al 1980). Nutritional strategies should be included as an essential part of pediatric oncology to prevent adverse effects caused by malnutrition (Bauer et al 2011). No specific dietary guidelines are available for children with cancer, despite the well-documented need for adequate nutrition in long-term outcome.
The degree of chemotoxicity experienced by the patient is classified according to the Common Toxicity Criteria (CTC) shown in Table 2.3.
Grade 1 (mild) Grade 2 (moderate) Grade 3 (severe) Grade 4 (life-threatening)
Prevalence of chemotoxicity in children with cancer
However, very few studies have assessed the role, if any; that diet plays a role in toxicity in the pediatric oncology population. A Malawian study of patients with nephroblastoma aimed to evaluate the pharmacokinetics of vincristine in these patients, who are generally malnourished and have large tumors, and to compare them with patients diagnosed and treated in the United Kingdom. Malnourished patients in Malawi had lower vincristine clearance rates than a comparable patient population with better nutritional status (Israëls et al 2010).
Patients with localized disease were assigned to a 4-week two-drug schedule and those with metastatic disease to a 6-week three-drug schedule. Of the 60 patients who received preoperative chemotherapy, 58% (n=35) had CTC grade 3 neutropenia and 27% (n=16) had CTC grade 4 neutropenia. A recent study evaluated whether BMI at diagnosis or weight change during therapy predicts toxicity in intermediate-risk rhabdomyosarcoma.
Four hundred sixty-eight patients aged 2–21 years were evaluated for grade 3 and 4 chemotoxicities, hospital days, and their number. At week 42, there was a trend toward more grade 3 and 4 toxicities in patients who lost more than 10% of their weight from baseline to week 24. This study and the other two mentioned all suggested that dose reductions should be considered in malnourished patients. to prevent an increase in the incidence and severity of toxicity (Burke, Lyden, Meza, Ladas, Dasgupta, Wiegner & Arndt 2013).
Factors that influence nutritional status and chemotoxicity
- Absorption
- Drug-protein binding
- Hepatic metabolism
- Renal function
The pharmacokinetics of antipyrine, an analgesic and antipyretic, was studied in malnourished children in India. The plasma half-life was increased (10.4 hours) in the malnourished group, compared to 6.3 hours in the control. The metabolic clearance rate was decreased in the malnourished group (47.1 ml/hr per kg), compared to 70.1 ml/hr per kg in the control group.
The plasma antipyrine half-life decreased to 6.6 hours and the metabolic clearance rate increased to 66.5 ml/hour per kg. This study looked exclusively at the effect of antipyrine on improving nutritional status and liver metabolism. This again indicates that drug metabolism is impaired in malnourished children and with an improvement in nutritional status comes improved hepatic drug metabolism (Homeida, Karrar & Roberts 1979).
The effect of malnutrition on renal function is another important determinant of the pharmacokinetic behavior of many drugs (Murry et al 1998). Alleyne (1967) investigated the effect of severe malnutrition on the renal function of severely malnourished Jamaican children. Careful modification of the dosage regimen in malnourished children is necessary to achieve effective therapeutic levels while avoiding toxic effects (Mehta 1990).
Conclusion
METHODOLOGY
- Type of study
- Background information on study site
- Study design
- Study population and sample
- Study methods and materials .1 Anthropometry
- Serum albumin
- Chemotoxicity
- Statistical analysis
- Reduction of bias
- Anthropometry
- Biochemical
- Reliability and validity
- Data quality control
- Ethical considerations
The study population consisted of newly diagnosed pediatric patients with nephroblastoma admitted to the Department of Pediatric Surgical Oncology (B3W) of IALCH between 2004 and 2012. Anthropometric data were collected before treatment initiation by the registered dietitian assigned to the Pediatric Surgical Oncology department. Height was measured using the stadiometer attached to the scale, and infants (under 2 years of age) were measured on an infantometer.
Tumor weight was obtained from patient records and rounded to the nearest 0.01 kg. These are more relevant to the various nationalities of SA and are used internationally (Dinsdale et al 2011). Blood samples were taken from each patient on admission to the hospital and sent to the National Health Laboratory Service at IALCH for analysis of serum albumin.
A chi-square goodness of fit test was applied to the indices WFA, HFA and WFH. A chi-square test of independence was applied to the categorical indices (MUAC, TSFT, WFA, HFA, and WFH). For the purpose of this study, the reduction of bias is explained with respect to the anthropometric and biochemical measurements.
RESULTS
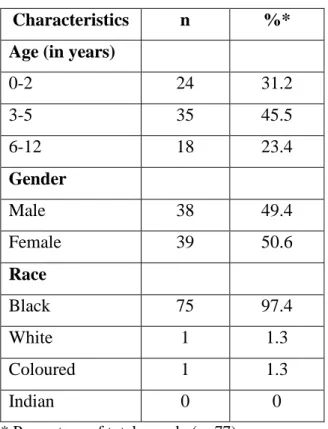
Sample characteristics (n=77)
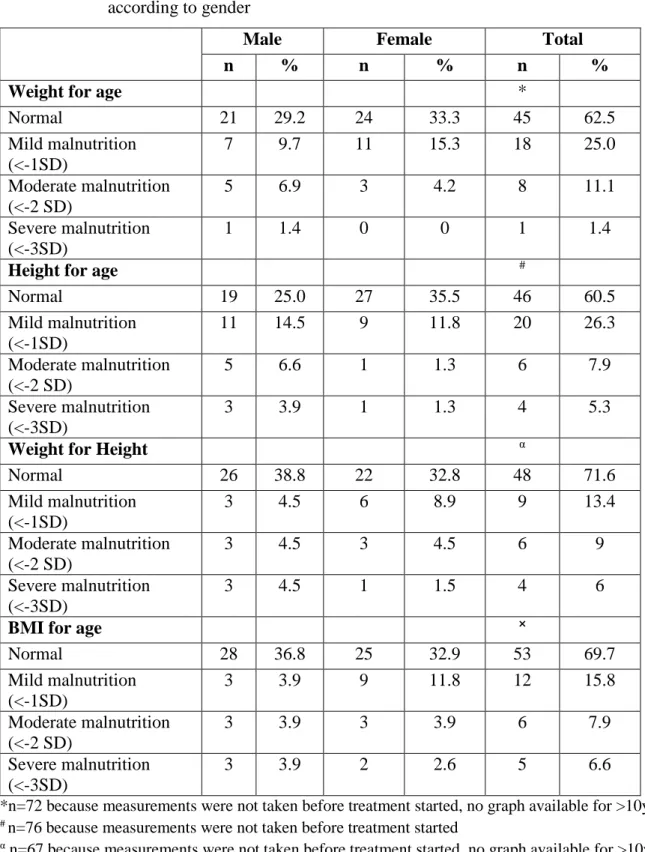
The incidence of malnutrition in children with nephroblastoma on admission as measured using specific anthropometric parameters
Race
The influence of malnutrition on the prevalence of chemotoxicity
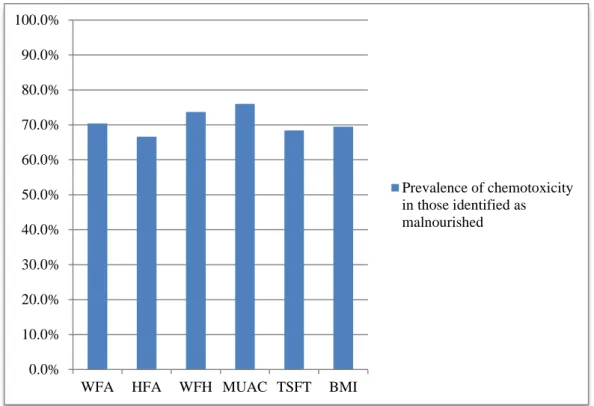
To investigate this aim, an analysis was performed on each parameter 'nutritional status' to detect any differences between patients with and without chemotoxicity. A clinically significant relationship was found between each of the parameters and the chemotoxicity experienced in patients classified as malnourished. More than two-thirds of patients classified as malnourished (based on any of the parameters) experienced chemotoxicity.
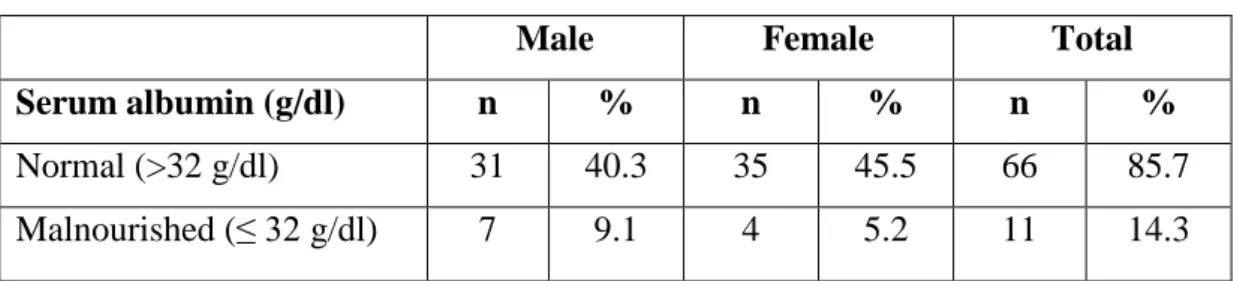
There was no significant difference in serum albumin measurements between those with and without chemotoxicity (p>0.05). However, the mean serum albumin value for those who experienced chemotoxicity and those who did not was 37.76 g/dl and 40.11 g/dl, respectively.
The influence of malnutrition on the frequency and duration of chemotoxicity The frequency of chemotoxicity was measured as the number of times the subject experienced
There was a clinically significant association between those identified as malnourished using BMI for age and the duration of chemotoxicity experienced. The group with normal nutritional status experienced chemotoxicity for an average of three days while those classified as malnourished experienced chemotoxicity for an average of six days. The other nutritional status measures (WFA, HFA, WFH, TSFT and albumin) showed no significant correlation with frequency and duration of chemotoxicity.
Summary of results
DISCUSSION
- Sample characteristics
- Assessment of nutritional status .1 Anthropometry
- Serum albumin
- The influence of malnutrition as determined by anthropometry and serum albumin on the prevalence of chemotoxicity
- The influence of malnutrition as determined by anthropometry and serum albumin on the frequency and duration of chemotoxicity
- Summary
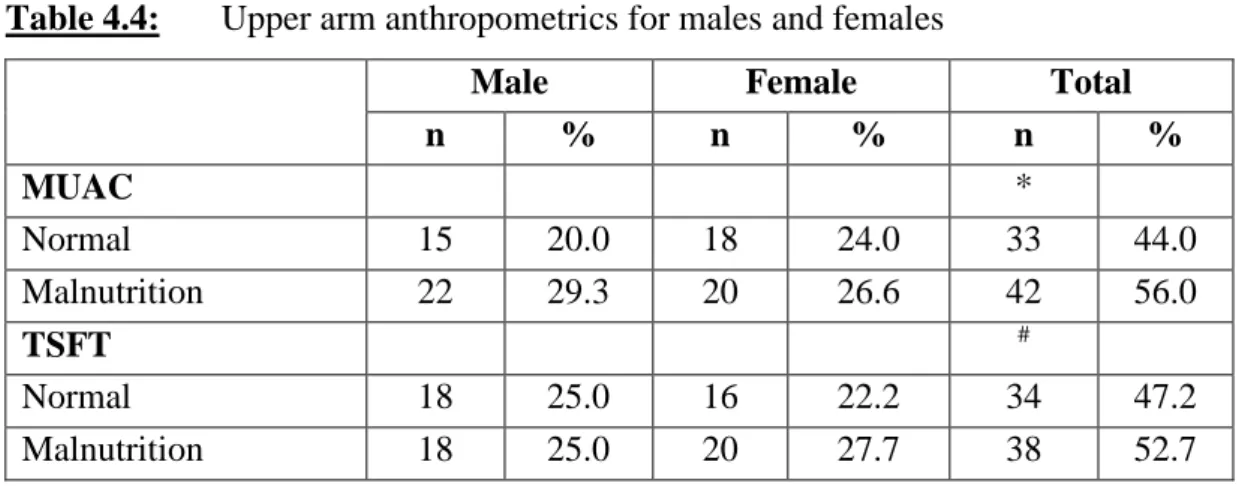
When arm anthropometry was used to classify nutritional status, the prevalence of malnutrition increased to more than half of the cohort. A clinically significant relationship was also found between each of the parameters and the prevalence of chemotoxicity in those identified as malnourished. This study found that the frequency and duration of chemotoxicity was significantly higher in patients classified as malnourished at MUAC admission.
As the frequency of chemotoxicity increased, the duration of chemotoxicity also increased. The duration of chemotoxicity was doubled in those who were malnourished according to BMI for age. This study also showed that patients with serum albumin above 32 g/dL on admission had a lower incidence and duration of chemotoxicity.
By implementing nutritional support at admission and throughout treatment and by assessing nutritional status to ensure adequate nutrition is provided, the frequency and duration of chemotoxicity can be reduced. The prevalence of malnutrition increased to more than half when MUAC (56%) and TSFT (53%) were used. Poor nutritional status, identified by MUAC, on admission may lead to an increased risk of experiencing chemotoxicity as well as increased frequency and duration of chemotoxicity.
CONCLUSION AND RECOMMENDATIONS
- Introduction
- Conclusion of the study
- Study limitations
- Recommendations for dietetic practice The following recommendations are made
- Implications for further research
However, IALCH treats patients from two provinces in South Africa and is therefore representative of a broader spectrum of the South African population. Comparison of the World Health Organization (WHO) Child Growth Standards and the National Center for Health Statistics/WHO International Growth Reference: Implications for child health programs. Dose calculation of anticancer drugs: a review of current practice and introduction of an alternative.
Efficacy of central parenteral nutrition versus peripheral parenteral nutrition and enteral nutrition in reversing protein-energy malnutrition in children with advanced neuroblastoma and Wilms' tumor: a prospective randomized study. Effectiveness of enteral and parenteral nutrition in the nutritional treatment of children with Wilms tumor. Nutritional status at diagnosis in children and adolescents with cancer in the Asociacion de Hemato-Oncologia Pediatrica de Centro America (AHOPCA) countries: preliminary results from Guatemala.
Nutritional status at diagnosis is related to clinical outcomes in children and adolescents with cancer: A perspective from Central America. The South African National Health and Nutrition Examination Survey, 2012: SANHANES-1: The Health and Nutrition Status of the Nation.