The aim of the study was to describe the individual social capital and mental well-being of older people (60+) living in a residential care facility in Durban, KwaZulu-Natal, and the readiness of staff and residents for the expected introduction of technology-assisted communication (TAC). The findings of the study were intended to facilitate the planning and implementation of future interventions using technology-assisted communication aimed at improving individual social capital and mental well-being.
INTRODUCTION AND BACKGROUND OF STUDY
- BACKGROUND
- PROBLEM STATEMENT
- SIGNIFICANCE OF THE STUDY
- SUMMARY OF THE CHAPTER
Various strategies, including technologically assisted communication, have been suggested for increasing the social contact of older persons (Dickinson & Gregor 2006; Fokkema & Knipscheer, 2007; White et al., 2002). There are no South African studies that measure the contribution of individual social capital to the mental well-being of older people (Petersen et al., 2012).
LITERATURE REVIEW
LITERATURE SOURCES
INTRODUCTION
The literature reviewed is viewed through a lens of social capital and mental health promotion, with a focus on individual social capital (as opposed to collective capital) in its influence on the benefits that the individual can derive from being included in social networks. This includes a systematic examination of social networks and the relational dynamics within them, and of social and mental health outcomes, addressing the potential for technologically enhanced communication in promoting mental health.
OLDER PERSONS IN THE SOUTH AFRICAN CONTEXT
Contrast this with the black racial group, where the single largest category among the elderly in 2009 was people with no schooling (40.5%). It should be pointed out that the health facilities visited by older people vary according to racial group.
LONELINESS AND DEPRESSION IN OLDER PERSONS
- Measurements of loneliness
It consists of twenty items, some positively worded (i.e. pointing in a non-lonely direction), others pointing in the opposite direction (de Jong Gierveld et al., 2006). It has been translated into many languages and is believed to be understandable by the less educated (de Jong Gierveld et al., 2006).
MENTAL WELLBEING AND RELATED POSITIVE INDICATORS
- Self-efficacy
- Trust
- Reciprocity
- Measurement of mental wellbeing
It is worth noting that the reaffirmation of the elderly person's sense of worth as a counterbalance to the setback appears to have greater value when it comes from non-relatives (Drageset et al., 2009). Those most likely to be involved in frequent volunteering are the elderly, women, the highly educated, the childless and the previously married (Cornwell et al., 2008).
SOCIAL CAPITAL
- Social networks
- Social support
To start with network size relative to older people: Van Kemenade et al. 2006) point out that social networks decrease as members age. Current literature discusses the importance of family and friends as a source of support for older adults (Drageset et al., 2009; Keating et al., 2004).
TECHNOLOGICALLY ASSISTED COMMUNICATION
In summary, access to a telephone or mobile phone or communication via the Internet can facilitate social connectedness and to the extent that it can contribute to mental well-being. Both of the above studies are weakened by limitations related to study duration or sample size.
CONCLUSION
There is therefore no purpose in burdening the elderly with discarded mobile phones or computers that ignore these limitations (van Biljon & Renaud, 2009). Although there are disagreements among researchers about the extent to which technologically enhanced communication can contribute to the formation of social capital, there appears to be general agreement that communication can contribute something; that as a form of bridging capital it promotes connections between and among social and support networks, giving older people access to resources they would otherwise not be able to access and allowing them to maintain for a while longer their independence, the loss of which is often accompanied by mourning ( Keating et al., 2004).
AIMS AND OBJECTIVES OF THE STUDY
- AIM OF THE STUDY
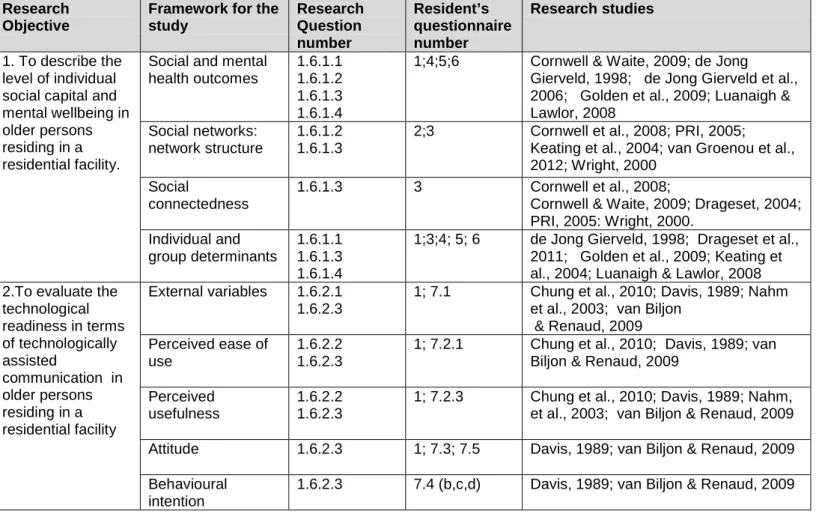
- RESEARCH OBJECTIVES, QUESTIONS AND HYPOTHESES
- Research objective one
- Research objective two
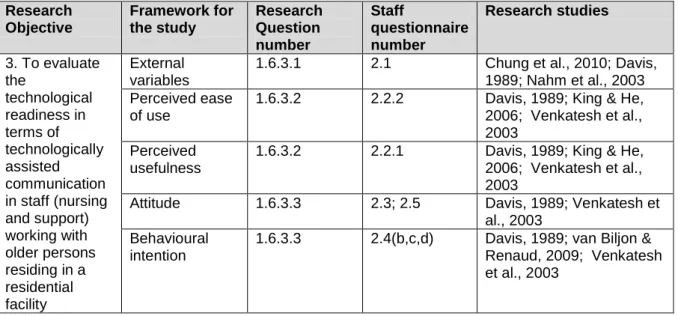
- Research objective three
- Hypothesis
- OPERATIONAL DEFINITIONS OF TERMS
- CONCEPTUAL FRAMEWORK
- Introduction
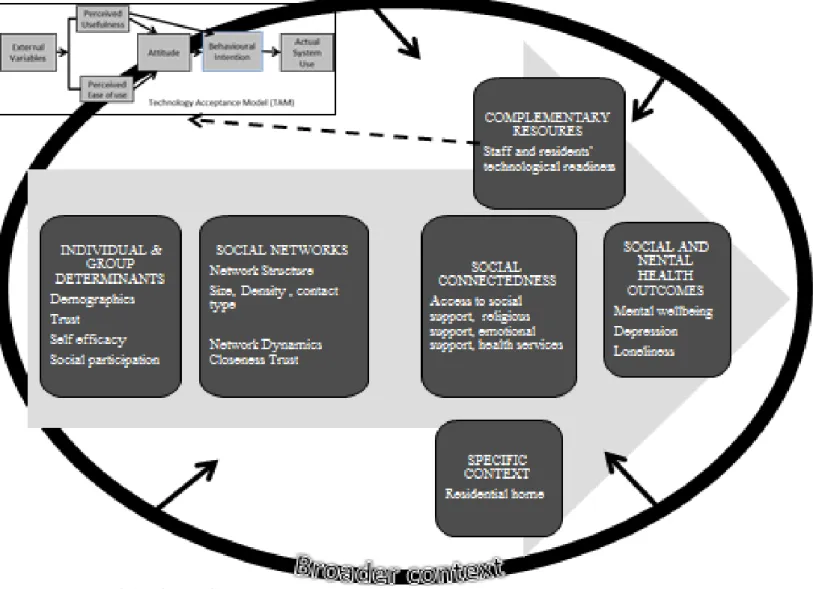
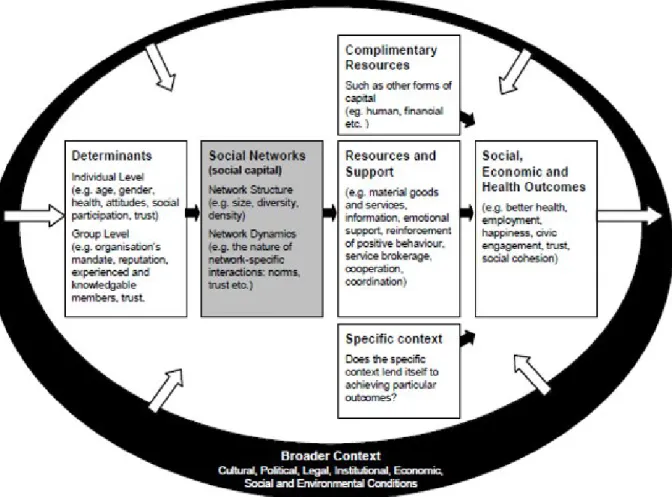
- Policy Research Initiative (PRI) framework
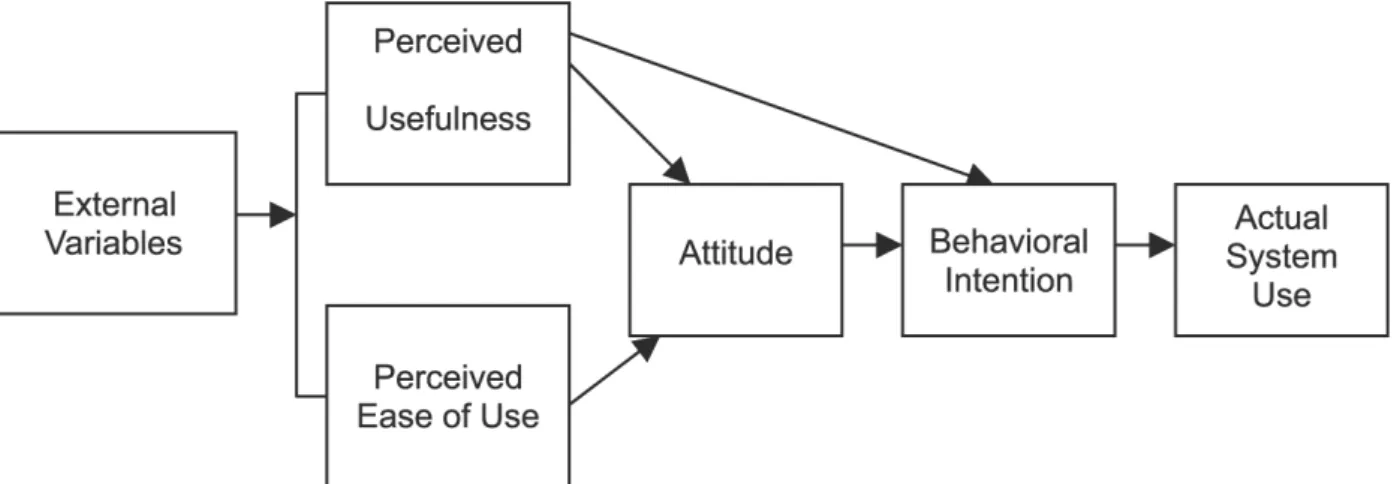
- Technology Acceptance Model (TAM)
- Application of models within this study
- SUMMARY OF THE CHAPTER
What is the level of social connectedness of the residents, as reflected in social participation, inside and outside the residential facility. Operational definition: The network structure includes the density of the social network (number of people in the social network), the frequency of contact of the respondent with network members (ranging from less than annual to daily) and the type of contact (direct or non-direct contact ).
METHODOLOGY
INTRODUCTION
PARADIGM AND RESEARCH DESIGN
RESEARCH SETTING
A district surgeon from the Department of Health has been assigned to the institution, who visits it once a month. The organization has assigned a social worker from its social agency department who visits the facility once a week.
POPULATION AND TARGET POPULATION
- Resident Population
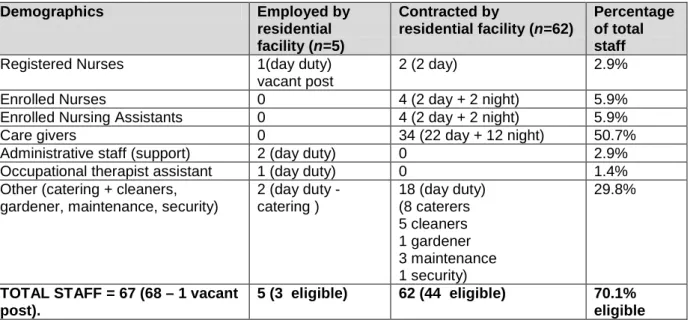
- Staff Population
Social workers can be reached from the central office at any time through the institution manager or nurse. However, the residential facility noticed a change of residence by different population groups, because when the researcher obtained the first list of establishments three months before the data collection, there were no residents from the "black" population group; however, there was one black resident at the time of data collection.
SAMPLE AND SAMPLING PROCEDURE
- Sample one: Residents (older persons)
- Sample two: Residence Staff
There was no sampling and the total residents (N=103) who met the inclusion criteria were invited to participate. All of the direct care staff population for the facility (minus the two who participated in the pilot study (N=45), either permanent employees or contract agency staff) were invited to participate.
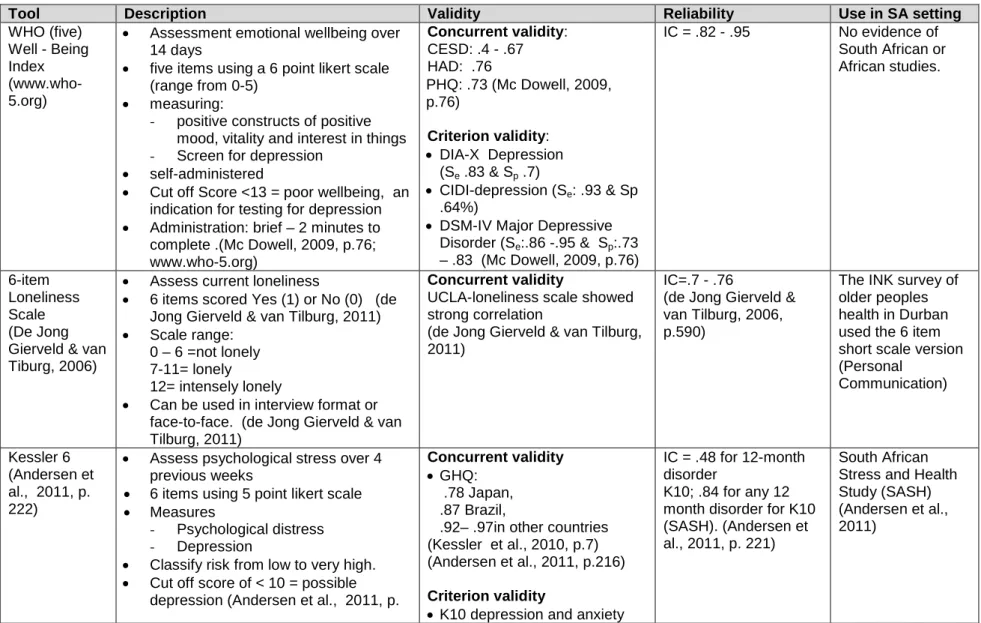
RESEARCH INSTRUMENTS
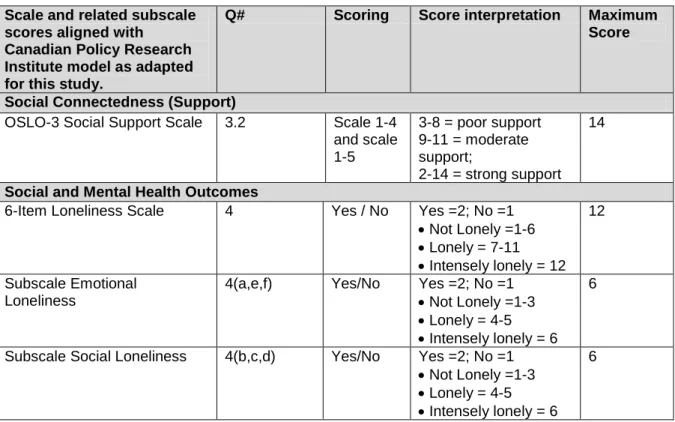
- Scales used in residents’ questionnaire
- Validity and reliability of the questionnaires
These data enable the future study of the possibilities for strengthening the mental health of residents in the selected residential facility and also in other residences. Validity: face validity was achieved to the extent of the agreement of the research supervisor with the items included in the questionnaire and with the experts' review.
DATA COLLECTION PROCEDURE
- Preparation for data collection
- Data collection from residents
- Data collection from residential facility’s direct care staff
In preparation for data collection from the residents, the researcher designed posters and displayed them in prominent places three days before the start of the survey (See Appendix 16: Invitation poster). Before the start of the survey, the Nursing Service Manager requested all 44 healthcare providers to attend the orientation sessions.
DATA ANALYSIS
- Data analysis of residents’ questionnaire
- Data analysis of staff questionnaire
Current access to technologically supported communication was described with frequencies and percentages of residents with landlines, mobile phones and computers and each of the selected activities. Technology readiness scores were calculated for each of the independent variables (PEU, PU, attitudes towards technology and behavioral intention to use technology).
SUMMARY OF THE CHAPTER
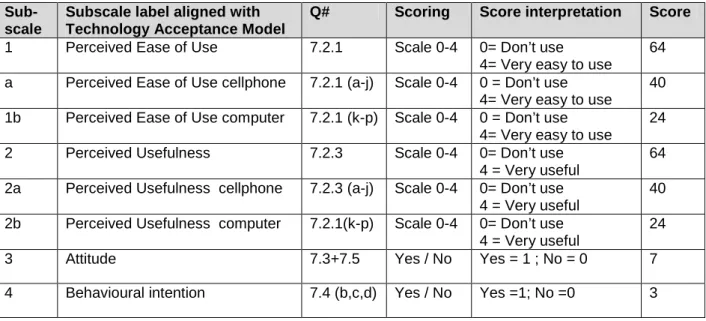
The formation of the subscales took place according to the residents' questionnaire, except for subscale four (Behavioral intention), since all respondents already used technology-supported communication. Scoring of the subscales was as in the above chapter on residents' technological readiness.
RESULTS
INTRODUCTION
DEMOGRAPHICS
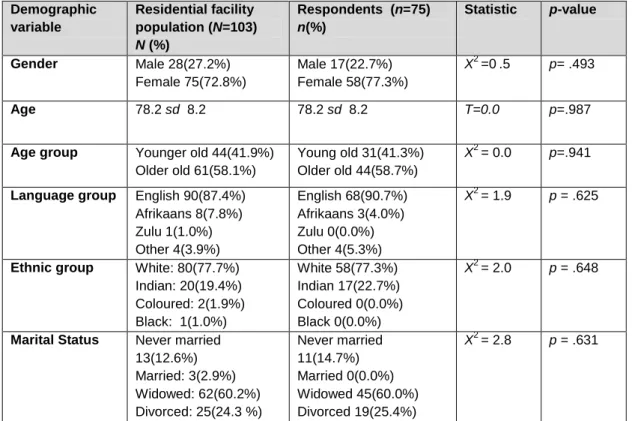
- Demographic profile of residents
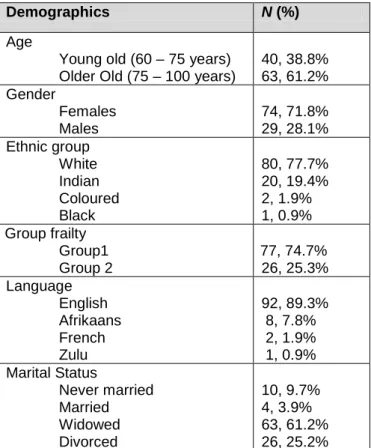
- Demographic profile of the sample (respondents)
Of the 75 respondents, respondents indicated that English is their home language, with five (5) respondents of the remaining seven coming from the older age group. In both the age groups, the greatest length of stay in the facility was in the category of two to five years See Table 10: Demographics of the respondents [residents]).
PSYCHOSOCIAL STATUS
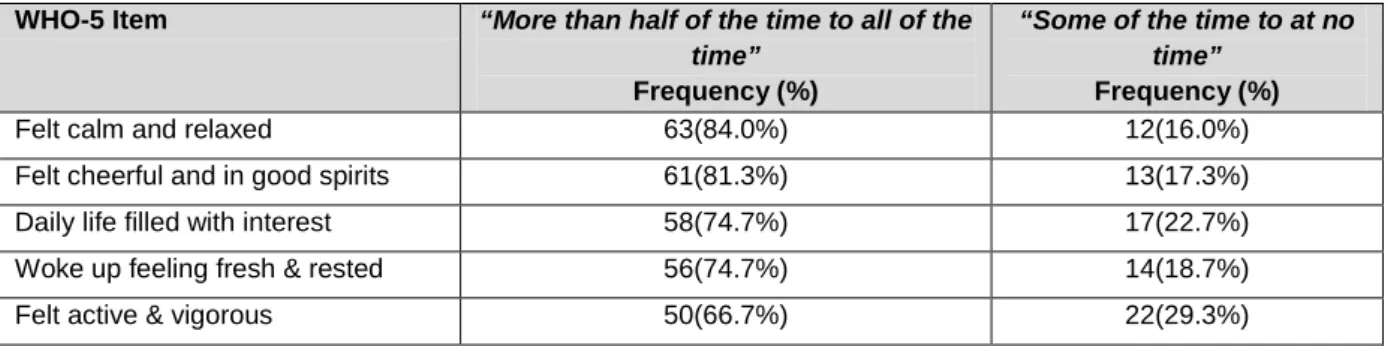
- Mental wellbeing
- Psychosocial distress
- Loneliness
Of the 75 residents respondents reported no psychosocial distress (scores between 6 and 11), while they reported mild psychosocial distress (indicative of a mild to moderate mental health disorder), and five respondents reported experiencing severe distress psychosocial (indicative of a serious mental disorder). This correlation was again driven by a positive correlation between K6 and emotional loneliness (r=-.533, p=<.001), with high levels of increased emotional loneliness associated with high increases in psychological distress and 28.4% of variation in psychological. the result of concern is explained by the presence of loneliness.
SOCIAL CAPITAL
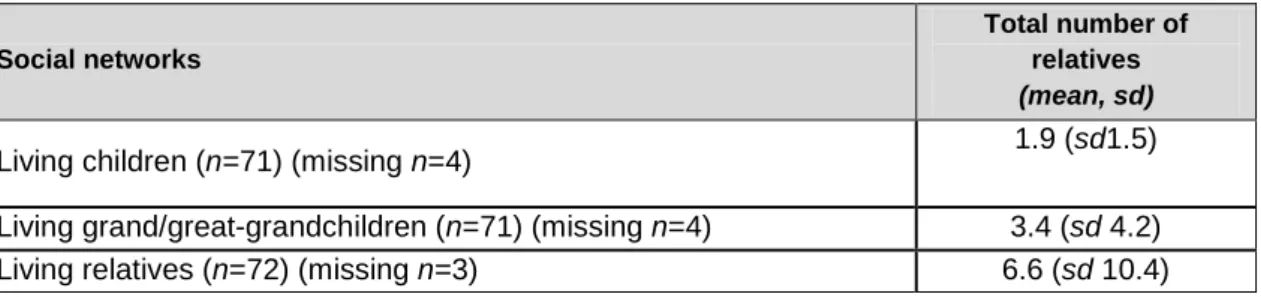
- Network structure – size and density
- Network dynamics
- Associations between social capital and mental wellbeing
The average number of living relatives was higher in the older group (8) compared to the younger group (4). Differences in mental well-being (measured by any negative category) were tested using the nonparametric Mann Whitney U test.
TECHNOLOGICAL READINESS
- Technological readiness of residents
- Staff technological readiness
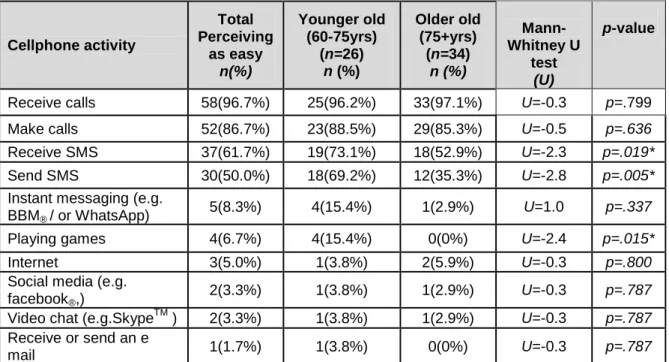
Age groups: There were significant differences between the younger and the older in the frequency of mobile phone use. Just as identified in the perceived ease of use, the perceived usefulness of the computer and mobile phones was low.
SUMMARY OF THE CHAPTER
In relation to the failure of the respondents to select social media as attractive, the software program that offered the least appeal was social media (e.g. Facebook.
DISCUSSION
- INTRODUCTION
- SOCIAL CAPITAL AND MENTAL WELLBEING
- Mental wellbeing
- Social Connectedness
- TECHNOLOGICAL READINESS OF THE RESIDENTS
- Attitudes and Behavioural Intention
- TECHNOLOGICAL READINESS OF DIRECT CARE STAFF
- SUMMARY OF THE CHAPTER
Overall, residents reported good levels of social support (43% reported strong support and 44% moderate support); only 13% of respondents reported poor support. The main findings and recommendations will be described in the next and final chapter of the study.
CONCLUSION AND RECOMMENDATIONS
- KEY FINDINGS
- RECOMMENDATIONS
- Recommendations for consideration by the residential facility
- Areas where additional research is recommended
- LIMITATIONS OF THE STUDY
- CONCLUSION
The emancipatory character of action research, its history and the current state of the art. Increased prevalence of depression in cohorts of the elderly: an 11-year follow-up in the general population - the HUNT study.
RESIDENT QUESTIONNAIRE
What is the most common form of contact you have with each of the following people? KESSL ER 6 Please mark an X in the appropriate box for each of the 6 items below.
STAFF QUESTIONNAIRE
Which technologically assisted communication generally has the greatest appeal to you (Please put 5 in the box next to your choice). Which technologically assisted communication generally appeals to you the least (please mark 1 in the box next to your choice).
CHANGES TO QUESTIONNAIRES FOLLOWING PILOT STUDY
Have you been involved in cultural groups outside the residence in the last three months. Have you been involved in cultural, social or community groups outside the residence in the last 3 months.
PERMISSION TO USE PRI MODEL
FACE VALIDITY
REQUEST FOR APPROVAL BY RESIDENTIAL FACILITY
I look forward to receiving your written permission and on completion providing you and the board with a written report and participants (residents and staff) feedback in two informal tea and cake sessions.
LETTER OF REQUEST TO SENIOR NURSING SERVICES
I look forward to receiving written approval and a convenient date for us to meet, followed by your and your staff's continued support for the survey. It would give me great pleasure to provide you and the participants with a written report (recognizing anonymity) on the outcome of the survey upon completion.
INFORMATION SHEET: RESIDENT
As stated earlier your participation is voluntary and you may withdraw at any time before discarding the questionnaire in a locked box upon completion. I will also notify you of the date (within the next two days) and time, as well as the place where you will meet to fill out the questionnaire.
INFORMATION SHEET: STAFF
There is time for you to consider your participation and ask questions of myself or my supervisor using the contact details below. Should you choose to participate, I will make arrangements for the signing of the consent and notify you of the date (within the next two days) and time, as well as where to meet to complete the questionnaire.
INFORMED CONSENT AND CONFIDENTIALITY
I provided the above participant with an information sheet and an opportunity to ask questions to facilitate understanding of informed consent.
GATEKEEPER PERMISSION: RESIDENTIAL FACILITY
APPROVAL LETTERS: TAFTA CEO, DIVISIONAL MANAGER
I Ellanette Booyzen, Senior Nursing Services Manager, TAFTA hereby grant my approval to Mary Anne Jarvis to conduct a study on the individual social capital and well-being of older people living in a residential facility in Durban KZN and the readiness of the environment for technology-driven healthcare Promotion.
UKZN HSS ETHICAL APPROVAL
INVITATION TO SET UP FEEDBACK SESSIONS
INVITATIONAL POSTER
CERTIFICATE OF UKZN RESEARCH POLICY V RESEARCH
PERMISSION TO USE QUESTIONS IN QUESTIONS USED
CONFIRMATION OF EDITING
TURNIT IN REPORT