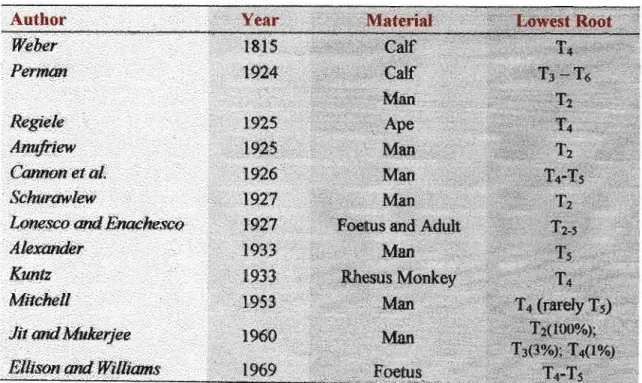
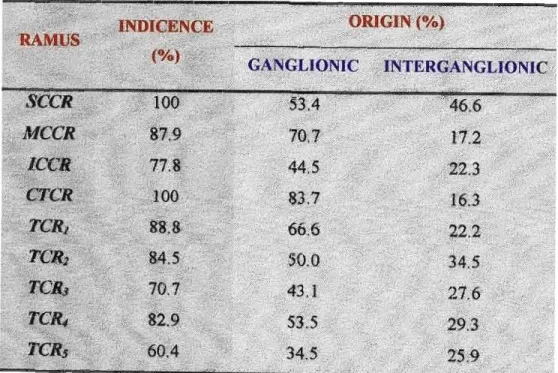
Summary of Incidence and Origin of Cardiac Sympathetic Nerves Incidence of origin of SCCR (n=58). Antero-lateral view of the right cervical sympathetic chain demonstrating CTG relationships in a fetus.
INTRODUCTION
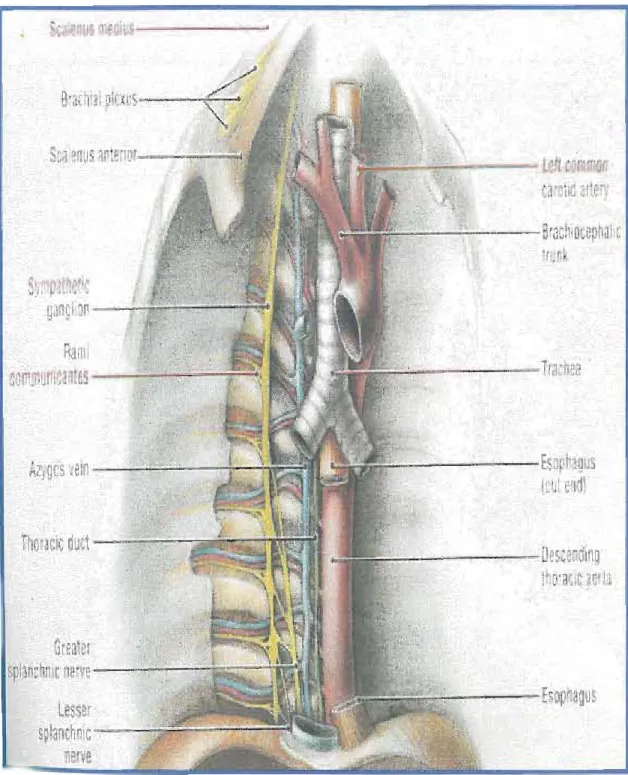
Document the appearance and bony relationships of the superior cervical (SCG), middle cervical (MCG), inferior cervical (ICG), and cervicothoracic (CTG) ganglia. In addition, the origin and occurrence of other branches arising from the medial aspect of the cervical and thoracic chain (including the splanchnic nerves and vascular rami in the neck) will be documented.
REVIEW OF LITERATURE
These reveal that he had a clearer conception of sympathetic trunks and their branches than that of his predecessors. By the end of the 18th century, it was clear with Bichat (1800), that what he called the 'sympathetic nervous system' controlled visceral functions while somatic functions were under the direct control of the brain and spinal cord (this idea still prevails ).
CERVICAL SYMPATHETIC CHAIN
- SUPERIOR CERVICAL GANGLIA (SCG)
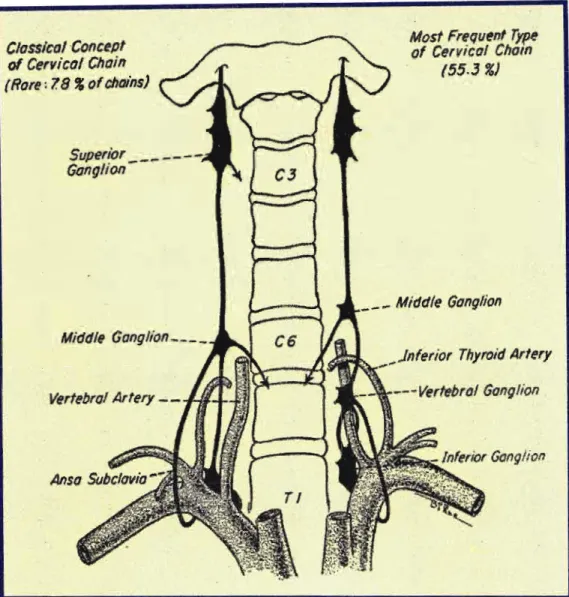
- MIDDLE CERVICAL GANGLION (MCG)
Jamieson et al (1952) reported that the junction of the inferior thyroid artery and the cervical chain occurs at or below the level of the 7th. CTG lies at the junction of the cervical and thoracic portions of the sympathetic trunk.
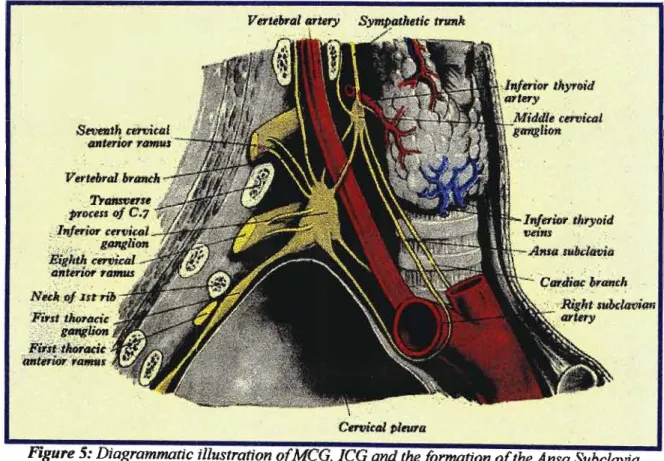
The Ansa Subclavian (AS)
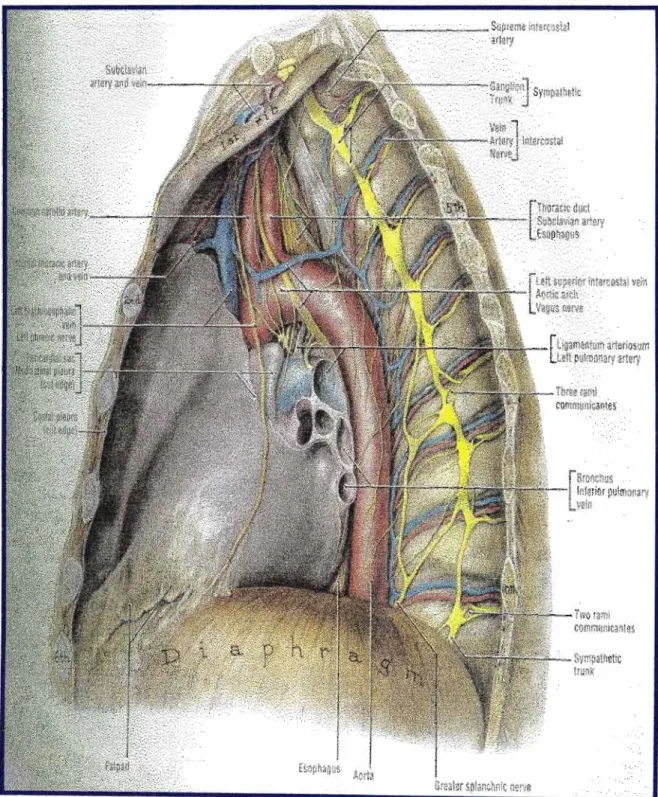
THORACIC GANGLIA (TG)
Rami communicantes to the upper thoracic portion of the chain vary more than anywhere else in the thorax (Hollinshead, 1956). Twigs from the 2nd to the 5th ganglia go to the deep part of the cardiac plexus (Hollinshead, 1956).
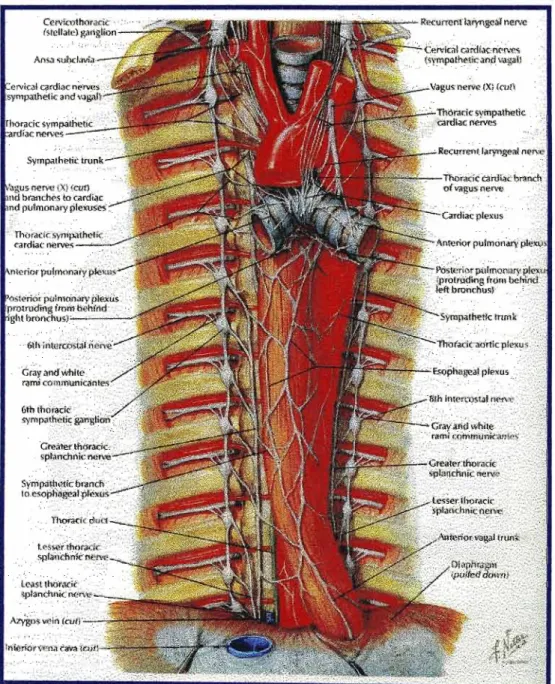
CARDIAC SYMPATHETIC NERVES
Cervical cardiac nerves dominated the cardiac sympathetic nerve literature until the mid-20th century (Kuntz and Morehouse, 1953). It descends behind the subclavian artery and along the anterior part of the trachea to join the deep part of the cardiac plexus.
OTHER MEDIAL BRANCHES
- SPLANCHNIC NERVES
- VASCULAR BRANCHES
- PULMONARY BRANCHES
- OESOPHAGEAL PLEXUS
According to Pearson and Sauter (1971), the branch of the phrenic nerve joins the extension of the subclavian plexus, which passes into the internal thoracic artery. The medial branches of the upper five thoracic ganglia are very small: they supply filaments to the thoracic aorta and its branches. These communicate plexiformly on the connective tissue of the external pharyngeal constrictors.
The efferent sympathetic fibers are postganglionic fibers from the 2nd to 5th thoracic ganglia in the sympathetic trunk. The posterior part of the pulmonary plexus is formed by the rami cardiac plexus and 2ndto the 5thhor 6ththoracic ganglia (Williamsetal., 1995).
![Figure 16: Origin ojsplanchnic nerves from the thoracic sympathetic chain [Agur, 1991]](https://thumb-ap.123doks.com/thumbv2/pubpdfnet/10631445.0/64.849.108.769.110.766/figure-origin-ojsplanchnic-nerves-thoracic-sympathetic-chain-agur.webp)
EMBRYOLOGY
A fourth arrangement would result from the persistence of one or both parts of the original mass as a separate ganglion, thereby producing additional ganglia or complete duplication. In most areas of the cord - at all 12 thoracic levels, at lumbar levels (Ll-3) and at the sacral areas (S2-4) - the neuroblasts in more dorsal regions of the basal columns differentiate and form distinct intermedio-Iateral cell columns [Figure 19 ]. The thoracic and lumbar intermedio-lateral cell columns contain central autonomic motor neurons of the sympathetic nervous system, whereas the intermedio-lateral cell column of the sacral region contains central autonomic motor neurons of the parasympathetic system.
The peripheral ganglia of some specialized sympathetic pathways develop from neural crest cells that cluster adjacent to large branches of the dorsal aorta. A pair of these prevertebral and pre-aortic ganglia originate from the cervical neural crest and form at the root of the celiac trunk.
![Figure 19: Schema illustrating the development ofpossible variations ofthe ganglionated chainfrom the primordial cell column [Pick, 1970]](https://thumb-ap.123doks.com/thumbv2/pubpdfnet/10631445.0/72.840.163.714.514.1054/figure-illustrating-development-ofpossible-variations-ganglionated-chainfrom-primordial.webp)
MATERIALS AND METHODS
- MATERIALS
- GROSS ANATOMICAL DISSECTION
- THORACIC DISSECTION
- CERVICAL DISSECTION
- HISTOLOGY
- NOMENCLATURE
- IDENTIFICATION OF GANGLIA
- IDENTIFICATION OF CARDIAC RAMI
- STATISTICAL ANALYSIS
Two transverse skin incisions were then made: .. i) From the notch of the neck to the tip of the shoulder; .. ii) From the xiphoid process of the sternum along the lower border of the ribcage fur laterally as the mid-axillary line. In the fetuses, the stomach was then removed from the viscera, while in the adults the sample was divided at the level of the umbilicus (for ease of use). A midline skin incision was made from the midpoint of the body of the mandible to the midpoint of the first transverse cut of the thoracic dissection.
The rami arising from the inter-ganglionic segments of the sympathetic chain were named after the nearest ganglion located in the sympathetic chain. Interganglionic chain length (in adult specimens) between: SCG and MCG, SCG and CTG, MCG and CTG.
RESULTS
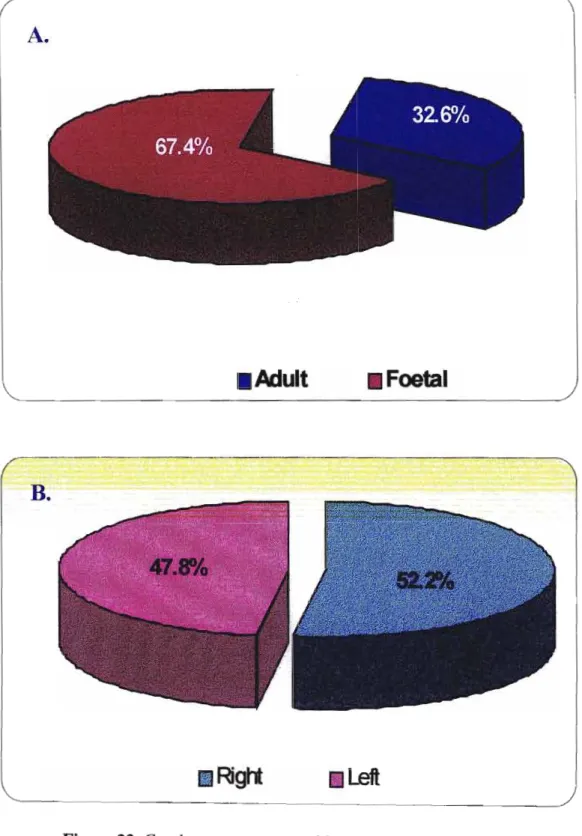
SAMPLE
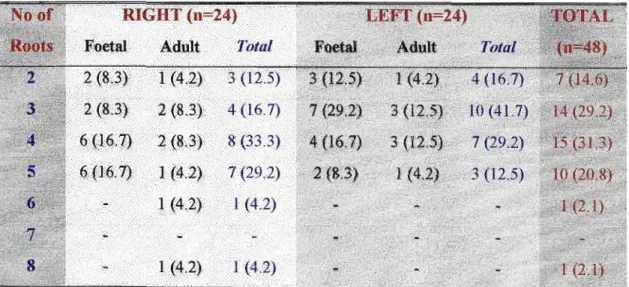
Thirty-one fetuses and seventeen adults with a total of eighty-nine sides (right, 43 and left, 46) were included in this study, as shown in Table 2 [Figures 22 and 23].
CERVICAL SYMPATHETIC CHAIN
- COURSE AND RELATIONS
- SUP ERIOR CERVICA L GANGLION
The subclavian loop was formed by cords that pass before and behind the subclavian artery, joining these two ganglia. The relationship of the SCG to the cervical vertebrae is shown in Table 4. The SCG was found to be located between the Cl-C4 vertebrae; with a position between Cl-C) which is the most dominant (48.3%). The SCG was found posterior to the carotid sheath and anterior to the prevertebral fascia in the long capitis muscle [Plates 1 and 2].
In the fetal specimens, the lower pole of SCG was located immediately above the bifurcation of the common carotid artery [Plate 3]. Communicating rami from SCG to the last four cranial nerves (glossopharyngeal, vagus, spinal accessory and hypoglossal nerves) were also found.
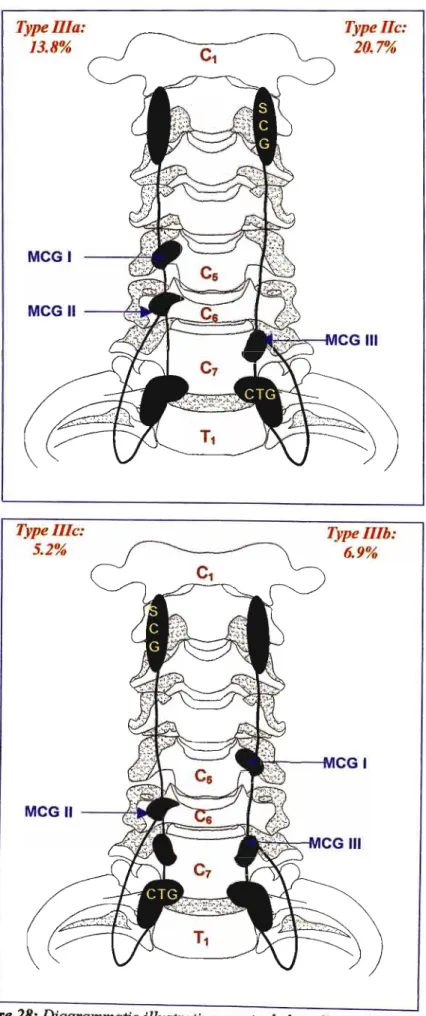
Type JIb
- INFERIOR CERVICAL GANGLION (ICG)
- CERVICO-THORACIC GANGLION (CTG)
- THORACIC SYMPATHETIC CHAIN
- COURSE AND RELATIONS
- THORACIC GANGLIA (TG)
The origin of the vertebral artery, from the subclavian artery, was located immediately posterior tolCG. The lateral branches consisted of rami communicantes to the intercostal nerves (ventral rami), while the medial branches consisted of numerous visceral rami, including cardiac rami, splanchnic nerves, and vascular branches [Plate 12]. The lower part of the chain lies on the vertebral bodies and the intermediate intercostal space.
At the level of the diaphragm, the chain deviates medially, to extend to the bodies of Tll-. The ganglia of the lower part of the thoracic sympathetic chain were situated just above the level of the spinal nerve, so that the rami ran down to the intercostal nerve.
PERCENTAGE
Rami were also distributed to the antero-Iateral aspect of the vertebral bodies and the intervertebral disc [Plate 14]. Cardiac sympathetic rami were differentiated according to their ongms from the cervical and thoracic parts of the sympathetic chain into three groups: cervical cardiac sympathetic rami (CCR), cervicothoracic cardiac rami (CTCR), and thoracic cardiac rami (TCR). The origin of cardiac ischemia from the sympathetic chain was found to be highly variable and asymmetric.
In these, the distance from the inferior pole of the SCG to the origin of the SCCR ranged from 4.8 mm to 19.3 mm (mean distance: 17.3 mm). It passed posterior to the common carotid artery and descended behind the subclavian artery to enter the cardiac plexus at the arch of the aorta.
Percentage
THORACIC CARDIAC SYMPATHETIC RAMI
The origin of these cardiac rami was from both the ganglion and from the interganglionic segment. In2/9 sites (22.2%) TCR1 arose from the upper half of the interganglionic segment of the chain during TIG. In 20/58 sites (34.5%), TCR2 arose from either the lower half of the interganglionic segment of the chain above or the upper half of the chain below the ganglion.
![Figure 38: Origin and incidence ofreR]](https://thumb-ap.123doks.com/thumbv2/pubpdfnet/10631445.0/134.834.113.752.111.435/figure-38-origin-and-incidence-ofrer.webp)
Incidence
CARDIAC PLEXUS
All sympathetic contributions from the cervical and thoracic sympathetic chains were found to be distributed directly in the deep cardiac plexus. This plexus is located posterior to the arch of the aorta and anterior to the left bronchus at the bifurcation of the pulmonary trunk. Fibers from this cardiac exudate were seen to pass forward to the anterior surface of the aortic arch and postero-laterally to the bronchi.
The 'superficial' cardiac plexus and the pulmonary plexus thus received indirect branches from the sympathetic chain via the 'deep' plexus.
SPLANCHNIC NERVES
Thoracic Sympathetic Thoracic Ganglia Greater Splanchnic Small Splanchnic Plate 20: Antero-Iateral view of right sympathetic chain demonstrating the splanchnic nerves in a fetus with accompanying schematic diagram. There was no correlation between number of roots of GSN with the absence of the LSN and lsn [plate 22].
Vertebral Artery
Where the ICG and T1 ganglion were unfused, a ramus from the right T1 ganglion was recorded to the subclavian artery. The ansa subclavia was clearly separated from the above branches and was observed in 100% of cases and included anterior and posterior limbs forming a loop around the subclavian artery. In the case of unfused ICG and T1 ganglion, no rami to the ICA were recorded at this level.
Brachiocephalic Trunk
Intercostal Arteries
Aorta
These were numerous from the upper part of the cervical chain and arose the SCG and the chain below this ganglion [Plate 26]. Pulmonary branches were noted to arise from the cardiac plexus and pass anteriorly to the arch of the aorta and posteriorly to the bronchus.
HISTOLOGICAL ANALYSIS
CI-IAPTER 5 DISCUSSION
CERVICAL SYMPATHETIC CHAIN
- Course and relations
- Superior Cervical Ganglia
- Middle Cervical Ganglion
- Inferior Cervical Ganglion
- Thoracic ganglia
In this study, such a 'double chain' was observed in the formation of the subclavian ansa in all specimens. The literature reviewed showed inconsistencies regarding the spinal levels of the 'high' and 'low' MCG. The course and relationships of the thoracic sympathetic chain were consistent with those described in the literature reviewed.
The thoracic part of the chain is continuous with the cervical sympathetic chain at the root of the neck. Unfortunately, they vary more in the upper thoracic part of the chain than anywhere else in the thorax.
CARDIAC SYMPATHETIC NERVES
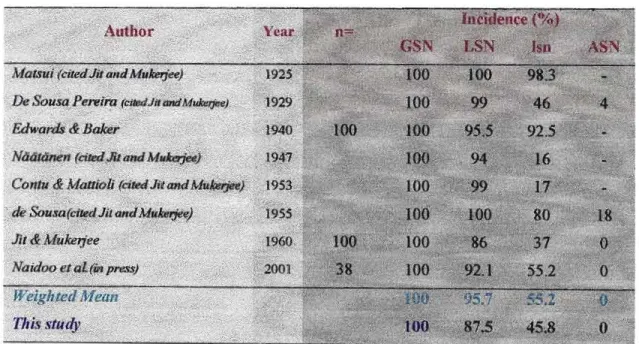
Variability in cardiac nerve origin was also seen in the thoracic region. There was no correlation between the number of GSN roots with the absence of LSN and lsn. The advent of minimally invasive and video-assisted surgery has revived interest in variable splanchnic nerve patterns.
In view of the described GSN variations, it is suggested that the procedure to perform splanchnicectomy be performed from the level of the T3 ganglion (Naidoo et al, in press). In light of the sympathetic contributions to the pharynx noted, it is suggested that the innervation of the pharynx and larynx be investigated.
CONCLUSION
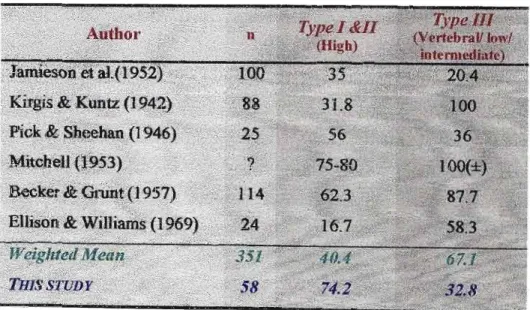
This study also agrees with Axford (1928), Jamieson et al. (1952), Mitchell (1953) and Becker and Grunt (1952) in that there is sufficient evidence to include the 4 ganglia as a constant entity in the cervical sympathetic chain. It should be noted that this study reports the highest incidence of normal/typical MCG (according to the textbook definition), i.e. this study further reports the origin of the TCR from the thoracic sympathetic chain to the interganglionic segment between TsG and T6-~ ganglia.
This study further records branches of the chain between MCG and T1 ganglion, including, to the brachiocephalic trunk in 17% of specimens. The intricate anatomical relationships presented in this study are testament to the complex anatomy of the sympathetic nervous system.
ALLAN F D (1958) An analysis of the visceral cervicothoracic branches of the vagus and sympathetic trunk in the presence of an anomalous right subclavian artery. AzAKIE A, McELHINNEY D B, THOMPSON R W, RAVEN R B, MESSlNA L M, STONEYR J (1998) Surgical management of effort thrombosis of the subclavian vein as a result of thoracic outlet compression. BALJET B, DRUKKER J (1981) Some aspects of the innervation of the abdominal and pelvic organs in the human fetus.
CLAES G, GonmERG G, DROTI C (1993) Endoscopic electrocautery of the thoracic sympathetic chain: a minimally invasive method to treat hyperhidrosis. 43.McLAcHLAN EM - The fonnation of synapses in the sympathetic ganglia of mammals innervated with preganglionic or somatic nerves.
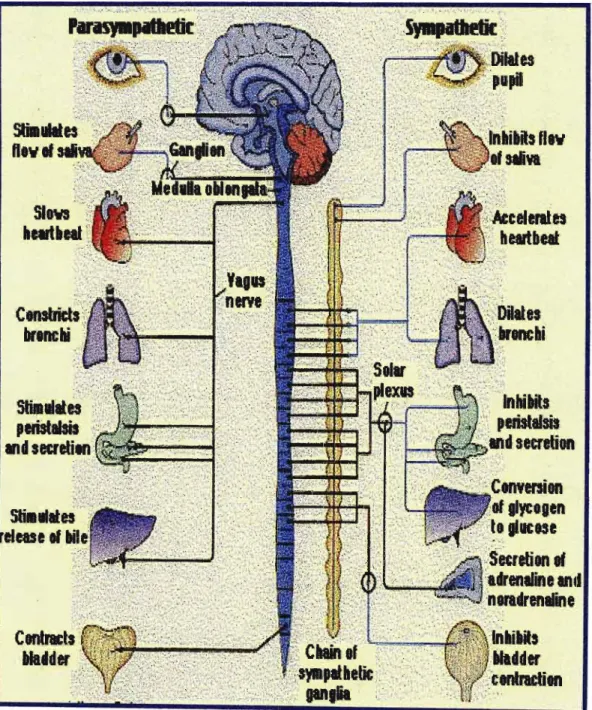
![Figure 2: The thoracic and abdominal sympathetic trunks displaying thoracic and abdominal autonomic plexus {AdaptedfromMartini and Timmons, 1996]](https://thumb-ap.123doks.com/thumbv2/pubpdfnet/10631445.0/27.841.113.761.128.882/thoracic-abdominal-sympathetic-displaying-thoracic-abdominal-autonomic-adaptedfrommartini.webp)
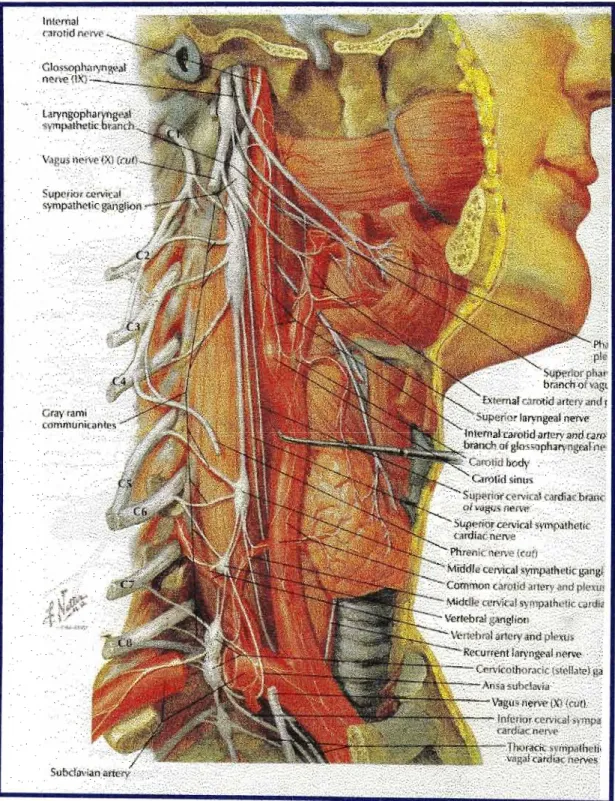
![Figure 8: Relations ofCTG [Adaptedfrom Netter, 1990]](https://thumb-ap.123doks.com/thumbv2/pubpdfnet/10631445.0/45.831.103.761.699.1095/figure-8-relations-ofctg-adaptedfrom-netter-1990.webp)