Excluded' type results in exclusion of the product of the mutant allele from the mature collagen molecule (non-deforming OI). These patients have relatively large skulls but underdeveloped facial bones, leading to a characteristic triangular facial appearance. Calcification of the interosseous membrane between the radius and ulna limits rotation of the forearm and can cause dislocation of the radial head.31 Women with OI Type 5 who are expecting a pregnancy should be screened.
OI type 8 is characterized by severe growth retardation and extreme skeletal undermineralization. The differential diagnosis for suspected OI depends on the severity of the condition and the age at which it manifests. The goals of treatment for OI are to reduce pain, prevent fractures and improve mobility.
Treatment depends on the severity of the disease and the age of the patient. Infants with OI are prone to fracture with trivial trauma, so one of the most important aspects of treatment is gentle handling from the infant. Physiotherapy, rehabilitation and occupational therapy are important elements in the interdisciplinary approach to managing OI.
Purpose: The purpose of this collaborative review was to analyze the diversity of orthopedic manifestations of OI through a systematic review of the literature.
Results
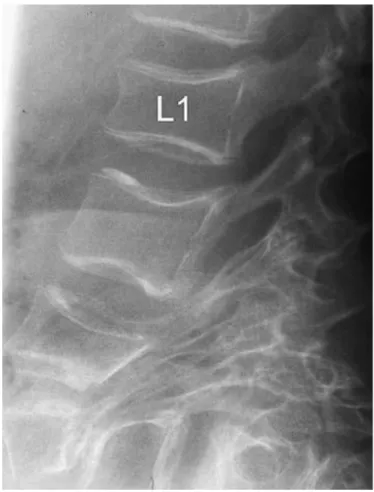
Multiple compression fractures of the spine and reduction in vertebral height lead to increased thoracic kyphosis or decreased lumbar lordosis. These progress to a global imbalance of the sagittal trunk.66 With age, spinal deformity worsens and complications such as back pain, respiratory distress, and nerve root compression may develop. Due to bone fragility and multiple vertebral compression fractures, an increased incidence of spondylolysis and spondylolisthesis is observed.
67 postulated that hyperlordosis of the lumbar spine was caused by lengthening of the lumbar pedicles and consecutive spondylolisthesis (Figure 6).
Upper and lower extremities
Typically, there may be anterolateral bowing of the femur and anterior or anteromedial bowing of the tibia (saber tibial deformity). Multiple long bone deformities of the limbs are caused by angulation and disregard of healed fractures, growth disturbances at the physes, and marked kyphoscoliosis resulting in short stature. A case of associated developmental dysplasia in the hip has been described.71 Adults are predisposed to rupture of the patellar ligament or the Achilles tendon.72-73.
In patients with OI type 5, Silence has shown that calcification of the interosseous membrane between the radius and ulna limits forearm rotation. Bending and curvature of the upper limbs is attributed to weight bearing through the upper limbs while sitting in a rack position in bed for extended periods. The characteristic appearance of the pelvis in OI is referred to as the "wine glass pelvis".
The occiput becomes prominent ("Darth Vader" appearance) or flattening of the cranial vault with a transverse fold of the skull base ("Tam O'Shanter skull"), (Figure 10).
Summary
Osteogenesis imperfecta: a study of clinical features and heredity based on 55 Danish families: consisting of 180 affected individuals. Is it necessary to screen for hearing loss in pediatric patients with osteogenesis imperfecta? Perinatal lethal osteogenesis imperfecta (OI type II): a biochemically heterogeneous condition usually due to new mutations in the genes for type I collagen.
Adult Brtl/+ mouse model of osteogenesis imperfecta demonstrates anabolic response to sclerostin antibody treatment with increased bone mass and strength. Isolated allogeneic bone marrow-derived mesenchymal cells engraft and stimulate growth in children with osteogenesis imperfecta: Implications for cell therapy of bone. Allele-dependent silencing of collagen type I using small interfering RNAs targeting 3'UTR Indels - a novel therapeutic approach in osteogenesis imperfecta.
Obstruction of the colon due to protrusio acetabuli in osteogenesis imperfecta: treatment by pelvic osteotomy. Increase in BMD and grip strength after one year of pamidronate treatment in 132 children with osteogenesis imperfecta.

Hyperextension at the cervicodorsal junction in osteogenesis imperfecta - a case report
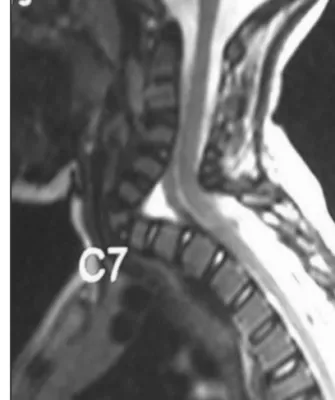
Follow-up images showed serration and impingement of the posterior vertebral body at the C7 level with associated hyperextension. Although OI is a well-known skeletal disease, there have been few reports of spondylolisthesis of the lumbar spine.7 Knowledge of normal developmental anatomy and radiographic features, as well as knowledge of common manifestations of hereditary and systemic diseases, is a prerequisite for understanding disorders affecting the pediatric cervical spine.13. The C-spine is free to rotate around the CD junction due to the relative immobility of the torso during head movement.
Pathologies affecting the bone or soft tissue component around the spine can lead to deformity in different planes. OI disrupts the musculoskeletal matrix, resulting in change in the morphology of the vertebral bodies, which can result in a spinal deformity. In our patient, the hyperextension deformity may be associated with a C7 vertebral microfracture with posterior wedging and compensatory forward bending moment to resist the weight of the macro-cephalic skull.
In addition, delayed milestones with the inability to raise the head may have caused persistent kyphosis of the cervical spine to maintain a mechanical axis with the thoracic spine. As shown by Basu et al14, lengthening of the pedicles with consequent rapid progression of spondylolisthesis leads to persistent hyperlordosis of the upper spine. Pathologies around the CD junction result in kyphotic deformity and are associated with neurologic deficits due to mechanical effects and smaller canal size and poor blood supply to the lower cervical region.11 Ronald et al reported three patients with OI who exhibited angular hyperlordosis caused by lumbar lengthening. pedicles and consecutive spondylolisthesis.7 Our patient had lengthening of the pedicles and thickening of the posterior elements with associated spondylolisthesis and subsequent hyperextension of the CD joint.
In childhood, with increased mechanical loading, pedicle lengthening and hyperlordosis show a rapid progression.3 This fits the hypothesis that osteopenia causes increased microdamage in OI bones, resulting in increased bone remodeling and, with increased mechanical loads, progressive deformations. Basu et al14 reported successful treatment of patients suffering from spondylolisthesis in OI due to lumbar pedicle lengthening with non-instrumented interbody fusion;. Because of the soft and fragile bony architecture encountered during surgery, posterior decompression and instrumentation with pedicle screws and rods was performed (Figure 3).
Although there are case reports on the management of severe kyphotic deformities of the thoracolumbar spine in The value of postural reduction in the initial management of closed spinal cord injuries with paraplegia and tetraplegia.
MMED PROTOCOL Collective review
The most striking abnormality is the tendency to fracture, generally after minor trauma and often without much pain or swelling. In reviewing the topic it becomes imperative to understand the pathophysiology, clinical variants and regions of skeletal involvement in order to treat the pathology. 1 The main clinical feature is increased bone fragility, which varies greatly in severity, ranging from intrauterine fractures and perinatal death to mild forms that remain asymptomatic until late in adult life.2,3.
OI is classified into different forms depending on the age of presentation, genetic abnormalities and clinical severity. The Silence 4 classification was used to classify OI according to its clinical severity into four different types. Orthopedic manifestations range from deformity and angular curvature of the bone, recurrent fractures, ossification of the interosseous membrane of the forearm, radial dislocations of the head, ankylosis of the hips, pelvic deformity, spondylolisthesis of the lumbar vertebrae, and spinal deformities that alter the balance of the back.
Treatment of OI depends on the severity of the disease and the age of the patient; in any case, a treatment strategy should ensure maximum long-term function and autonomy.7, 8, 9. A collective review of the literature will be undertaken via relevant search engines and search terms. An experienced medical librarian will be consulted to refine general approaches to conducting a comprehensive search of the above databases.
Academic books, journals and various publications on the subject will be used to collect relevant data. Information will be collected from studies including randomized controlled trials, review articles, case reports and systematic reviews. Literature published in the late 70s will be used for this review, as most of the initial work was done during this period.
Studies will be evaluated by content analysis, as meta-analyses will not be feasible due to the great diversity of study designs and variables. The study will rely exclusively on databases, electronic literature search resources, conference proceedings and literature prior to the mentioned study period, and the absence of two or more reviewers to independently collect and evaluate the data. This is not the case as the study is a literature review and does not include patient participation, use of pharmaceuticals or other treatment strategies.