Kenaikan Berat Badan Ibu Hamil dan Hubungannya Dengan Berat Badan Lahir Bayi
Sarma N. Lumbanraja, Delfi Lutan, Makmur Sitepu,M. Rhiza Z. Tala, Sarah Dina, Ismail Usman
Departemen Obstetri and Ginekologi, Fakultas Kedokteran Universitas Sumatera Utara,
Medan, Indonesia, Januari 2013
______________________________________________________________________
ABSTRAK
Tujuan Penelitian: Untuk mengetahui penambahan berat badan ibu hamil pada trimester pertama, kedua dan ketiga dan hubungannya dengan luaran berat badan bayi.
Metode: Studi kohort dilakukan pada RSUP.H. Adam Malik Medan dan RS. Sundari pada bulan Agustus 2012 dan selesai pada Januari 2013. Besar sampel adalah 104 ibu hamil yang melakukan kunjungan antenatal rutin sejak kehamilan trimester pertama sampai ketiga, serta yang melakukan persalinan di RSUP. H. Adam Malik Medan dan RS. Sundari.
Hasil: Karakteristik sampel berumur 20-35 tahun (80.8%), umur lebih dari 35 tahun (12,5%) dan umur kurang dari 20 tahun (6,7%). Paritas multigravida 56,7% dan hanya 1% grande multigravida. Karakteristik dari 104 sampel diperoleh berat badan sebelum hamil pada rentang 40,0-68,0 kg dengan rata-rata berat badan sebelum hamil 53,06 kg ± SD 7,09 dan tinggi badan 140-166 cm dengan nilai rata-rata 155,85 cm ± SD 5,8. Kenaikan berat badan ibu pada trimester I rata-rata 1 kg pada kelompok umur 20-35 tahun dan usia>35 tahun, sedangkan pada usia dibawah 20 tahun rata-rata 0,43 kg ± SD1,13. Tidak terdapat hubungan yang bermakna antara umur ibu dengan kenaikan berat badan pada trimester I (p>0,05). Pada trimester II, kenaikan berat badan ibu berdasarkan kelompok umur rata-rata 5 kg. Tidak terdapat hubungan yang bermakna antara umur ibu dengan kenaikan berat badan pada trimester II (p>0,05). Pada trimester III, kenaikan berat badan ibu paling tinggi pada kelompok umur 20-35 tahun yaitu rata 5,75 kg ± SD 2,19 dan terendah pada usia dibawah 20 tahun yaitu rata-rata kenaikan berat badan 4,64 kg ± SD 2,17, terdapat hubungan yang bermakna antara umur ibu dengan kenaikan berat badan pada trimester III(p<0,05). Berdasarkan data yang didapatkan dari pertambahan berat badan ibu per trimester, didapati pada trimester I berat badan ibu bertambah pada rentang 0–3,5 kg dengan nilai rata-rata 0,90±SD 0,92. Pada trimester II berat badan ibu mengalami penambahan lebih besar yaitu sebesar 0-10 kg dengan rata-rata 5,21 ± SD 2,14. Pada trimester III penambahan berat badan ibu relatif sama dengan pada trimester II yaitu 0,5-10,5 kg dengan nilai rata-rata 5,45 ± SD 2,24. Secara keseluruhan usia kehamilan dijumpai total kenaikan berat badan 5-20 kg dengan rerata 11,56 ± SD3,50. Rerata kenaikan berat badan ibu hamil tertinggi pada ibu dengan usia kehamilan 37 minggu (13 kg) dan yang terendah pada usia kehamilan 40 minggu (10,75 kg).
relatif sama ± 1 kg. Secara statistik menunjukkan tidak ada perbedaan yang bermakna (p>0,05). Kenaikan rata-rata berat badan ibu pada trimester II paling tinggi pada primigravida dan multigravida yaitu ± 5 kg dan paling rendah pada grande multigravida yaitu 2 kg namun tidak terdapat perbedaan bermakna (p>0,05). Kenaikan rata-rata berat badan ibu pada trimester III paling tinggi pada primigravida 6,08 kg ± SD 2,18, multigravida 5,03 kg ±SD 2,18, sedangkan paling rendah pada grande multigravida yaitu 2 kg. Terdapat perbedaan yang bermakna (p<0,05). Karakteristik berat badan sebelum melahirkan 48,0–83 kg dengan rata-rata 64,75 ± SD 8,85 dan berat badan ibu pada masa 24 jam post partum mengalami penurunan menjadi 42,0- 78,50 kg dengan nilai rata-rata 59,92 ± SD 8,81. Luaran berat badan bayi 2.500-4.000 gr dengan rerata 3119 ± SD 399,86 gr. Terdapat hubungan yang bermakna antara total kenaikan berat badan ibu dengan berat lahir bayi (p<0,05),dengan korelasi lemah (r=0,2).
Maternal Weight Gain And Corellation With Birth Weight Infants
Sarma N. Lumbanraja, Delfi Lutan, Makmur Sitepu,M. Rhiza Z. Tala, Sarah Dina, Ismail Usman
Department of Obstetrics and Gynecology, Faculty of Medicine University of Sumatera Utara,
Medan, Indonesia, Januari 2013
ABSTRACT
Objective: Knowing maternal weight gain during the first, second and third trimester of pregnancy and correlation with birth weight infants.Methods: Cohort studies was conducted at the Hospital H. Adam Malik Medan and Sundari Hospital in August 2012 and finished at January 2013. Sample were 104 pregnant women who do routine ANC from the first to the third trimester and delivery at term H Adam Malik Hospital and Sundari. Results: Maternal characteristics are generally aged between 20-35 years (80.8%), followed by the age group over 35 years (12.5%) and lowest in the age group less than 20 years (6.7%). Parity multigravida (56.7%) and only 1 person (1%) with grandemultigravida. Most mothers into labor at 38 weeks gestation (51.9%) and the lowest at 37 weeks (4.8%). Characteristics of 104 women found prepregnancy weight in the range of 40.0 to 68.0 kg with an average weight before pregnancy SD 7.09 ± 53.06 kg and height in the range of 140-166 cm with a mean value The average 155.85 cm ± 5.8 SD. Body mass index (BMI) was 18.03 to 25.00 with an average value of 21.78 ± 2.06 SD. Maternal weight gain trimester I average about 1 kg in the age group 20-35 years and age> 35 years, while under 20 years of age on average 0.43 kg ± SD1, 13. In the second trimester, maternal weight gain by age group unchanged at an average of about 5 kg. In the third trimester, maternal weight gain was highest in the age group of 20-35 years on average 5.75 kg ± 2.19 SD and the lowest
gain in pregnancy grandemultigravida lower than the primi and multigravida.
Keywords: Maternal weight, infant birth weight, body mass index
Introduction
The gestation period is the period
that determine the quality of human
resources. Growth and development of a
child, is determined by the condition during
in the womb. Pregnant women were healthy,
with good nutrition will certainly produce a
healthy baby. The low nutritional status of
the mother during pregnancy can result in a
negative impact. Among others, the high
maternal mortality rate and infant mortality.
Besides maternal risk of having low birth
weight babies (babies with low birth
weight). LBW rate in developing countries
four times higher than developed countries.
During the years 1990-2000 shows a variety
of sources ranging from 2-17% proportion
of LBW. If the proportion of pregnant
women 2.5% of the total population,
estimated 355000-710000 of 5 million
babies will be born with a low birth weight.
More than 9 million babies die each year,
98% occur in developing countries, and one
cause is low birth weight.
Therefore, maternal weight gain
optimum is essential for perinatal morbidity
and mortality. In 1987 The Global Safe
Motherhood Initiative was launched with the
aim of improving antenatal care and
counseling throughout the world. This
movement concentrates on nutrition and
weight gain during pregnancy, as are the two
important things that affect mothers and
baby outcomes.
1
Institute of medicine (IOM), in 2009
issued a recommendation maternal weight
gain recommendations are revising earlier in
1990. A new recommendations for total and
rate of weight gain during pregnancy
according to body mass index before
pregnancy.
2,3
According to Beyerlin to recent
research conducted Nohr showed an
increase in weight
4
lessbodyincreases the risk
oflow birth weight,but theweight
gainduringpregnancywill
causeexcessiveopposite effect, such
asobesity inchildhoodandinfantlarger.2
According toOlsonfromresearch
conducted byLowlerandChaturverdihave
foundevidence to support
theexcessiveintrauterinenutritionwillpromote
obesityafter birth. Meanwhile, according
toresearch conductedClaessonfromKiet,
showed that the degree ofweight gain
duringpregnancy isassociated with increased
riskof preeclampsia, cesarean saesarea, large
pregnancy. Andseveralother studieshave
shown arisingincidence ofweight andbody
mass indexduring
pregnancywithobstetriccomplicationsand
neonatus outcomes.5
Based on the above background, the authors
are interested in doing research on
relationship of increase weight gain during
pregnancy with the baby's outcomes, with
the hope we will get a real picture of the
weight gain of pregnant women and their
relationship with the baby's outcomes.
, 6
Method
This is a cohort study assessing the
weight gain during the first trimester of
pregnancy, second, third, and total increases
and relationship (correlation) with birth
weight infants. Assessment of maternal
weight gain correlation with birth weight
infants using Pearson correlation. The study
was conducted at the Hospital H. Adam
Malik Medan and Sundari Hospital in
August 2012 until the sample met. The
population in this study were all pregnant
women who perform routine ANC from the
first to the third trimester and at birth at term
gestation RS H. Adam Malik Hospital in
Medan and Sundari. The sample is
representative of the population that is
affordable pregnant women perform routine
ANC from the first to the third trimester in
pregnancy and delivery at term RS H. Adam
Malik Hospital and Sundari Hospital in
Medan. Sampling was conducted in
consecutive sampling in pregnant women
who gave birth to the ANC and RS H. Adam
Malik Medan and RS. Sundari. In this study,
the sample obtained is 104 people.
The way it works is that whole
pregnant inpartu that met the inclusion
criteria and were willing to follow the study.
Do mothers weighing before and 24 hours
post partum and infant birth weight. Then do
the recording of weight gain during the first
trimester of pregnancy up to three so
unknown total maternal weight gain during
pregnancy, the data is taken from state
control (ANC Card) patients. Statistically be
searched relations total maternal weight gain
weight babies born.
This study used primary and
secondary data were obtained from the
results of the weighing of pregnant women
and inpartucontrol statusof pregnant
womenin the hospitalwhere the study
wasconducted. The data obtained
wereprocessed witha computerprogram, then
the data ispresented in tabular
Result
Characteristics ofmotherswho are the
subjectof researchthat included age,
parityand gestational agecan be seenin the
tablesbelow.
Table 1. Characteristics ofthe
studymothersby age
Age
( years )
N %
< 20 7 6,7
20-35 84 80,8
>35 13 12,5
Total 104 100
Maternal characteristicsof the study
sampleare
generallyagedbetween20-35years(80.8%), followed bythe age
groupover 35 years(12.5%) and lowestin the
age groupless than 20 years(6.7%). It canbe
explainedthat theageis lessthan 20
Table 2. Characteristics of the study
subjects based on parity
years of
age is not recommended for a marriage by
the Marriage Law in Indonesia, while the
age of over 35 years, including high risk. As
quoted Rasmussen of Cleary-Goldman et al
that a pregnant woman over the age of 35
years at risk of developing chronic diseases
such as Type 2 diabetes can lead to
complications and increased morbidity post
partum.
Paritas N %
Primi 44 42,3
Multi 59 56,7
Grande 1 1,0
Total 104 100
Based on the characteristics of the
most parity is obtained with parity
multigravida (56.7%) and only 1 person
(1%) with grandemultigravida. The low
grandemultigravida can be explained due to
the easy obtainfamily planning servicesand
has beenwidely acceptedby the public.
Table 3. Karakteristikresearch
subjectsbygestational age
Minim um
Maxi mum
Mea n
SD
Prepregn ancy weight (kg)
40,0 68,0 53,0 6
7,09
Height (cm) 140,0 166,0 155, 85
5,8
Body Mass Index
(BMI)
18,03 25,00 21,7 8
The above tableshows
thatmostmothersdolaborat38 weeks
gestation(51.9%) and the lowestat 37
weeks(4.8%).
Age
Pregnancy
(weeks)
Table4.Characteristics ofthe study
subjectsbased onnutritionalstatus
N %
37 5 4,8
38 54 51,9
39 31 29,8
40 14 13,5
Total 104 100
Characteristicsofthe study sampleof 104
womenfoundprepregnancy weightin the
range of40.0 to 68.0kgwith an
averageweight before
pregnancySD7.09±53.06kgand heightin the
range of140-166cmwith amean value.The
average155.85cm±5.8SD. Foundbody mass
index (BMI) of104 womenwas18.03 to
25.00withan averagevalue of21.78±2.06SD.
Maternalweight gainduring pregnancycanbe
apicture ofthenutritional status of
mothersand birth weightbabieswillbe born.
This studymatchesthat duringpregnancythere
isincrease inmaternal weight. This weight
gain willmore
specificallydescribeunfoundedtrimester,
parityand gestational ageon
thesubsequenttables. Pregnant
womenwithanormalbodymass
indexmorewillproduce offspring
withabetteroutcomethan women witha body
mass indexoutsidethe recommended.
Table5.Relationsmaternalweight gainwith
agePertrimester
Age
(years)
N Mean SD P
Trimest
er I
<20
20 - 35
>35
7
84
13
0.43
0,93
0,92
1,13
0,91
0,93
0,150
Trimest
er II
<20
20 - 35
>35
7
84
13
5,00
5,33
4,50
2,84
1,93
2,96
0,415
Trimest
er III
<20
20 - 35
>35
7
84
13
4,64
5,75
5,45
2,17
2,19
2,05
0,014
The table above showsthat, the
picture of maternalweight
gaintrimesterIaverage about1 kgin the age
whereastheage below the20 yearaverage
of0.43kg±1.13SD. Statisticallyshowed
nosignificant associationbetweenmaternal
ageweight gainbytrimesterI (p>0.05).
In thesecondtrimester,
maternalweight gainby age groupunchanged
atan average of about5 kg.
Statisticallyshowed nosignificant
associationbetweenmaternal agewithweight
gain in thesecondtrimester(p>0.05).
In thethirdtrimester, maternalweight
gainwas highest intheage group of20-35
yearson average5.75kg±2.19SDand the
lowestunder the ageof 20 yearsbeing the
averageweight
gain4.64kg±SD2.17statisticallyshowednosig
nificant associationbetweenmaternal
agewithweight gain in
thethirdtrimester(p<0.05).
In termsof maternal weightby ageof
pregnant womeneachtrimester,
thenItrimesterweight gainwas highest inthe
age group20-35 yearswith an average
of0.93±0.91kgand the lowestin the age
group<20 year with an average of 0.43 ±
1.13 kg, but showed no statistically
significant difference in maternal weight
gain during trimester I by age group (p>
0.05). Similarly in the second trimester
weight gain was highest in the age group
20-35 years with an average of 5.33 ± 1.93 kg,
but statistics show no significant difference
in maternal weight gain during the second
trimester by age group (p > 0.05). In the
third trimester weight gain was also highest
in the age group 20-35 years with an average
of 5.75 ± 2.19 kg and showed a statistically
significant difference in weight gain of the
mother during the third trimester, by age
group (p <0, 05). It is clear that maternal age
between 20-35 years old is a good age for
pregnancy weight gain because it gives a
higher and suitable for pregnancy compared
with other age groups.
Table 6. Maternal weight gain per
trimester
Body weight
(Kg)
Mini
mal
Maxi
mal
Mea
n
SD
Trimester I
Trimester II
Trimester III
Total increase in
Weight Loss
0
0
0,5
5
3,50
10,00
10,50
20,00
0,90
5,21
5,45
11,56 0,92
2,14
2,24
3,50
Kruskall-Wallis test p=0,0001
Based on the data obtained from the
mother's weight gain per trimester, I found
trimester maternal weight gain in the range
from 0 to 3.5 kg with an average value of
0.90 ± 0.92 SD. In the second trimester
increase in the amount of 0-10 kg with an
average of 5.21 ± 2.14 SD. In the third
trimester maternal weight gain is relatively
the same as in the second trimester is from
0.5 to 10.5 kg with a mean value of 5.45 ±
2.24 SD. Overall total pregnancy weight
gain encountered 5-20 kg with a mean of
11.56 ± SD3, 50. Based on test statististik
with Kruskall-Wallis test obtained p
<0.0001 indicating a significant difference
maternal weight gain per trimester. In first
trimester, weight gain is quite slow with a
maximum weight gain of 3.5 kg. In the
second trimester, weight gain increases
faster with a maximum of 10 kg. Similarly,
the third trimester, the maximum increase in
weight up to 10.5 kg. And total weight gain
up to 20 pounds during pregnancy. If we
refer to the IOM recommendations in 1990
and 2009, the average weight gain was
found with this. Research conducted by Ota
also found the average weight gain of the
same. Significant weight gain in the second
trimester has been described in the study by
Yang in 2005 due to the increased appetite
pregnant after passing the 12th week
because of complaints of nausea vomiting
has begun to decrease, coupled with the
uterus and other organic tissue began to
increase the size and volume. If returned to
the theory, the weight gain was also affected
by the compounds leptin, which is a protein
produced by adipose tissue, regulatebody
weight,especiallyappetite.
Table7.The meanincrease
infull-termWeight LossMotherandBirth
Weightchildren based ongestational age
atdelivery
Gestati
onal
Ages
BB
Preg
nanc
y
Incre
ase
(Kg) Ano
va
Test
P
valu
e
Birth
weight
(gr)
Anova
Test
P value
37
week
Mean
13
0.35
1
3430.0
0.113 Std.
Deviatio
n
2.72 426.614 58
Minimu
m 9.5 2850.00
Maximu
m 17.0 3800.00
38
week
Mean 11.2
3 3068.52
Std.
Deviatio
n
3.43 316.570 11
Minimu
Maximu
m 20 3800.00
39
week
Mean 12.2
6 3127.74
Std.
Deviatio
n
3.32 327.350 06
Minimu
m 6 2650.00
Maximu
m 19 4000.00
40
week
Mean 10.7
5 3185.71
Std.
Deviatio
n
4.27 388.007 02
Minimu
m 5 2500.00
Maximu
m 18 3800.00
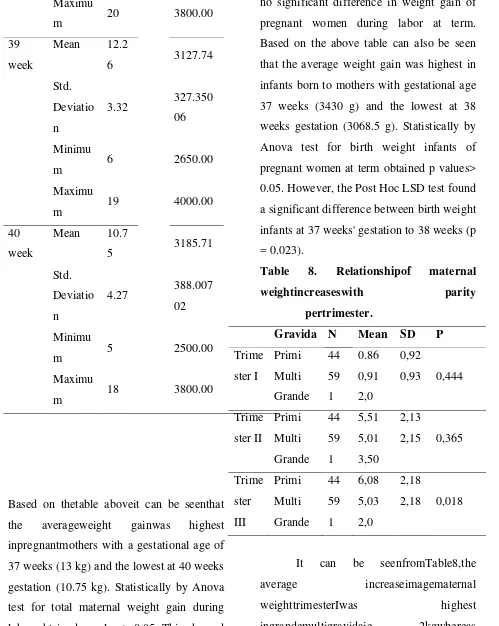
Based on thetable aboveit can be seenthat
the averageweight gainwas highest
inpregnantmothers with a gestational age of
37 weeks (13 kg) and the lowest at 40 weeks
gestation (10.75 kg). Statistically by Anova
test for total maternal weight gain during
labor obtained p values> 0.05. This showed
no significant difference in weight gain of
pregnant women during labor at term.
Based on the above table can also be seen
that the average weight gain was highest in
infants born to mothers with gestational age
37 weeks (3430 g) and the lowest at 38
weeks gestation (3068.5 g). Statistically by
Anova test for birth weight infants of
pregnant women at term obtained p values>
0.05. However, the Post Hoc LSD test found
a significant difference between birth weight
infants at 37 weeks' gestation to 38 weeks (p
= 0.023).
Table 8. Relationshipof maternal
weightincreaseswith parity
pertrimester.
Gravida N Mean SD P
Trime ster I Primi Multi Grande 44 59 1 0.86 0,91 2,0 0,92
0,93 0,444
Trime ster II Primi Multi Grande 44 59 1 5,51 5,01 3,50 2,13
2,15 0,365
Trime ster III Primi Multi Grande 44 59 1 6,08 5,03 2,0 2,18
2,18 0,018
It can be seenfromTable8,the
average increaseimagematernal
weighttrimesterIwas highest
inprimiandmultigravidasame
relativeincrease±1 kg. Statisticallyshowed
nosignificant difference(p>0.05).
Picture ofthe average increase inweight of
the motherat thesecondtrimesterwas highest
intheprimigravidaandmultigravida
Picture of the average increase in
weight of the mother at the highest in the
third trimester primigravidaie 6.08 SD 2.18
kg ± 5.03 kg followed multigravida SD ±
2.18, while the lowest in the
grandemultigravida 2 kg. Statistically
showed no significant difference (p <0.05). ± 5 kg
and lowest in grandemultigravida is 2 kg.
Statistically showed no significant
difference (p> 0.05).
Based on parity, the first trimester
weight gain was highest in the group
grandemultigravida is 2 kg and the lowest in
the primigravida group, with an average of
0.86 ± 0.92 kg, but statistics show no
significant difference in maternal weight
gain during I trimester by parity (p> 0.05).
In the second trimester weight gain was
highest in the primigravida with an average
of 5.51 ± 2.13 kg and lowest in the group
grandemultigravida only 3.5 kg, but showed
no statistically significant difference
maternalweight gainduring
thesecondtrimesterbyparity(p>0.05). And in
thethirdtrimesterweight gainwas highest
intheprimigravidawith an average6.08±2.18
kgand the lowestin the
groupgrandemultigravidais only2 kg, but
statisticsindicate asignificant differencein
weight gainbythe mother during
thethirdtrimesterof parity(p <0.05). The
results ofthis studyexplainthat
ingrandemultigravidamaternalweight
gainduring pregnancyis relativelysmall and
stayabout 2kg.
Table9.Weight of the motherbefore
deliveryand 24hourspost partum
Body
weight
Mini
mal (Kg)
Maxi
mal
Mea
n
SD
48,0 Before the
birth
83,0 64,7
5
8,85
42,0 24
hourspost
partum
78,50 59,9
2
8,81
pairedt-test
Maternal characteristics by prenatal
weight is in the range of 48.0 to 83 kg with
an average value of 64.75 ± 8.85 SD and
maternal weight at 24 hours post-partum
period decreased to 42.0 to 78.50 kg with an
average value of 59.92 ± 8.81 SD. Based on
statistical tests to obtain paired t-test p <0.05
indicating a difference in weight of the
mother before and 24 hours post partum
Table 10. Birth weight infants
Weight
(gr)
Minimum Maximum Mean SD
Baby's
birth
weight
2500.0 4000.0 3119 399,86
Based on research data obtained, birth
weight infants in 2500-4000 range 3119 g
with a mean ± SD 399.86.
Table 11.
Weight (kg) r p
The correlationbetween
thetotalincrease inmaternal
weightBirthweightbabies
Total increase In maternal body weight 0,213 0,03
With a birth weight infants
As shown in the table above shows
there is a significant correlation between
total maternal weight gain, infant birth
weight (p <0.05), with the correlation (+)
weak (r = 0.2). Infant birth weight obtained
from this study were within the normal
range is the range of 2500 g - 4000 g and
mean ± 399.86 gr 3119gr. Statistically
showed a significant association between
total maternal weight gain with birth weight
infants (p <0.05), with the correlation (+)
weak (r = 0.2). This suggests that maternal
weight gain during pregnancy period can be
a predictor for birth weight infants.
However, total maternal weight gain is not
entirely influenced by the weight of the baby
but also influenced by the amniotic fluid,
placental weight, and also increased
maternal organ and tissue edema.
References
1. Chairunita, Model
PendugaBeratBayiLahirBerdasarkan
PengukuranLingkarPinggangIbuHam
il. ITB, Bogor; 2006.
2. Beyerlien A, Schiessl B, Lack N,
Kries R V Optimal Gestational
weight Gain Ranges For the
Avoidance of Adverse Birth Weight
Outcomes : a Novel Approach. AM J
ClinNutr 2009-90 :1552-8, USA :
2009.
3. Ota E, Haruna M, Suzuki M, Anh D
D, Tho L H, Tam N T T et al.
Maternal Body Mass Index and
Gestasional Weight Gain and Their
Association With Perinatal
Outcomes in Viet Nam. Bull World
Health Organ 2011; 89: 127-136.
4. Anonymous, Weight Gain During
Guidelines, Report Brief. Intitute Of
Medicine Of The National
Acedemies May: 2009.
5. Olson M C, Strawderman S M,
Dennison BA. Maternal Weight Gain
During Pregnancy and Child weight
at Age 3 Years. Matern Child Health
J 13 : 839-846. USA. 2009
6. Claesson I M, Brynhildsen J,
Cedergren M, Jeppsson A, Sydsjo A,
Josefsson A. Weight Gain
Restriction During Pregnancy is Safe
For Both The Mother And Neonate.
ActaObstetricia et Gynecologica ; 88
: 1158-1162. Sweden. 2009.
7. American College of Obstetrics and
Gynecology Committe on Obstetric
Practice. Obstetric and Gynecology
106. 2005, pp: 671-75
8. Bodnar L M, Wisner K L, Kolko E
M, Sit D K Y, Hanusa B H,
edPrepregnancy Body Mass Index,
Gestational Weight Gain and The
Likelihood of Major Depression
During Pregnancy. Department of
Obstetrics, Gynecology, and
Reproductive Sciences, Pittsburgh;
2008.
9. Kinnunen TI. Prevention of
Excessive Pregnancy-Related
Weight Gain, [dissertation],
Tampere: University of Tampere.
2009.
10.Commitee to Reexamine IOM
Pregnancy Weigth Guidelines Food
and Nutrition Board and Board on
Children, Youth, and Families.
Rasmussen K N, Yaktine A L,
Weight Gain During Pregnancy : Re
Exemaining the Guidelines.
Washington D C : The National
Academies Press. 2009.
11.Jenifer Ng, Magee L A, Yarker E K.
Maternal Overweight and Excess
Gestational Weight Gain:
Identification of Maternal and
Perinatal Implications and Primary
Maternity Caare Providers’
Opportunities for Interventions to
Improve Health Outcomes.
Departements of Medicine, Obstetric
and Gynecology and Population and
Public Health, University of British
Columbia, Vancouver, BC. 2009
12.Kiel DW, Dodson EA, Artal R,
Boehmer TK, Leet TL. Gestational
Weight Gain and Pregnancy
much is enough?. American College
of Obstetricians and Gynecologist.
Vol 110 (4), October 2007, pp:
752-758.
13.Derbyshire E, Davies J, Costarelli V,
Dettmar P. Prepregnancy Body mass
Index and Dietary Intake in The First
Trimester of Pregnancy. J Hum
NutrDietet 2006, 19;267-273
14.Sahu MT, Agarwal A, Das V,
Pandey A. Impact of Maternal Body
mass Index on Obstetrics Outcome. J
ObstetGynaecol Res 2007,
33(5);655-659
15.Seligman LC, Duncan BB,
Branchtein L, Gaio DSM, Mengue
SS, Schmidt MI. Obesity and
Gestational Weight Gain : Caesarean
Delevery and Labor Complication.
Rev SaudePublica, 2006: 40 (3):
457-65.
16.Abrams B, Altman SL, Pickett KE.
Pregnancy Weight Gain : Still
controversial. Am J ClinNutr2000 ;
71 ( Suppl ): 1233S-41S.
17.Arkkola T. Diet During Pregnancy.
[dissertation], Tampere, University
of Tampere. Oulu University Press.
2009.
18.Naeye RL. Maternal Body Weight
and Pregnancy. Am J ClinNutr.
1990, 52. pp: 273-9.
19.Yang M J. Interrelationship of
Maternal Serum Leptin, Body Mass
Index and Gestational Age. J Chin
Med Assoc 2005, 68(10); 452-457.
20.Nohr EA, Vaeth M, Baker J L,
Sorensen T I A, Olsen J, Rasmussen
K M, Combined Association of
Pre-Pregnancy Body Mass index and
Gestational Weight Gain With the
Out Come of Pregnancy. AM J Clin
Nutr,2008;87 : 1750-9.
21.Chen Z, Du J, Shao L, Zheng L, Wu
M, Ai M, Zhang Y. Pre pregnancy
Body Mass Index , Gestational
Weight Gain, and Pregnancy
Outcomes in China. International
Journal of Gynecologic and
Obstetrics, 109 (2010), pp
41-44.
22.Anonymous. Epidemiology of
Gestational Weight Gain and Body
Weight Changes After Pregnancy.
[Epidemiologic Reviews].
EpirevOxfordJournals, 1999,
23.Upaydhyay S, Biccha RP, Sherpa
MT, Shrestha R, Panta PP.
Association between Maternal Body
Mass Index and The Birth Weight of
neonates. Nepal Med Coll J 2011,
13(1);42-45
24.Yazdani S, Yosofniyapasha Y,
Nasab BH, Mojaveri MH, Bouzari Z.
Effect of Maternal Body Mass Index
on Pregnancy Outcome and
Newborn Weight. BMC Research
Notes 2012, 5;34
25.Kalk P, Guthmann F, Krause K,
Relle K, Godes M, Gossing G et al.
Impact of Maternal Body mass Index
on Neonatal Outcome. Eur J Med
Res 2009, 14;216-222
26.Fraser A, Tilling K, Wallis C M,
Hughes R, Sattar N, Nelson S M et
al. Associations of gestational weight
gain with maternal body mass index,
waist circumference, and blood
pressure measured 16 years after
pregnancy ; the Avon Longitudinal
Study of Parents and Children. Am J
ClinNutr 2011,
doi:10.3945/ajcn.110.008326
27.Duggleby SL, Jackson AA.
Relationship of Maternal Protein
Turnover and Lean Body Mass
during Pregnancy and Birth Length.
Clinical Science 2001, 101;65-72
28.Han W H, Chen LM , Li C Y.
Maternal Weight ( BMI ), pregnancy
Weight Gain, and Risks of Adverse
Pregnancy Outcomes in Chinese
Women. Graduate Institute of Health
Polic and Management, College of
Public Health, National Taiwan
University, Taipei, Taiwan, R. O. C.
2010.
29.Crane JMG, White J, Murphy P,
Burrage L, Hutchens D. The Effect
of Gestational Weight Gain by Body
mass Index on maternal and neonatal
Outcomes. JOGC Janvier, 2009;
29-35.
30.Cunningham Gary F, et al, Obstetri
Williams, PenerbitBukuKedokteran
EGC,
RekomendasiPertambahanBerat,
Edisi 21, Vol 1, 2006; 252-4.
31.Islam A, Khan NA, Ehsan A.
Complications of Raised BMI in
Pregnancy. Professore Med J 2010,
17(3);498-504
32.Chang M, Kuo C, Chiang K. The
Index and Gestational Weight Gain
on Neonatal Birth Weight in Taiwan.
International Journal of Nursing and
Midwifery 2010, 2(2);28-34
33.Goli L. The Relationship Among
Pre-pregnancy BMI, Pre Pregnancy
Weight Gain, and Self Reported Post
Partum Depression. 2009
34.Suitor CW. Maternal Weight Gain ;
A Report of an Expert Work Group,
1997. Arlington, VA: National
Centre for Education in Maternal and
Child Health.
35.Viswanathan M, et al. Outcomes of
Maternal Weight Gain, Evidence
Report/Technology Assessment No
168. AHRQ Publication No. 08.
E009. Rockville, MD; Agency for
Healthcare Research and Quality.