Vol 7, No 1, January - March 1998 Fine needle aspiration biopsy on thyroid nodules and breast tumors
Evaluation
of the results of
fTne needle
aspiration biopsy cytology
on
thyroid
nodules
and breast
tumors
at the Hasan Sadikin
Hospital
Bandung
Pisi
Lukitto
Abstrak
Telah pernah dilakuknn dua penelitian, baik biopsi aspirasi jarum halus pada nodul tiroid, maupun pada tumor payudara. Tujuan penelitian ini adalah untuk mengetahui sensitivitas dan akurasi BNH di Rumah Sakit Hasan Sadikin . Pada 167 di antara 250 kasus nodul tiroid, telah dilalaùan pembedaha4 dan 16 ternyata ganas. Pemeriksaan sitologik BNH memberikan hasil 12 negatif palsu, 1
positif palsu, 4 positif benar, dan 150 negatif benar. Hasil diagnostik tes adalah sebagai berikut: sensitivitas 25Vo, spesifisitas 99,jVo, nilai prediksi positif 80Vo, nilei prediksi negatif 92,6Vo, dan alarasi92,2Vo. Pada penelitianyang lain terhad.ap 41 kasus tumor payudaro, ditemukan hasil 2 negatifpalsu, tidak ada positifpalsu, 35 positifbenar, dan4 negatifbenar. Hasil diagnosîik tes adalah sebagaiberikut: sensitivitas 94,6Vo, spesifisitas 700Vo, nilai prediksi positif 100Vo, nilai prediksi negatif 66,7%, dan akurasi 95,lVo.
Abstract
Two studies ol FNAB have been performed on thyroid nodules and breast tumors respectively. The aim of the studies was to test tbe sensitivity and aocuracy of FNAB in the Hasan Sadikin HospitâI. Among 250 cases of thyroid nodules, 167 underwent surgery, and 16 revealed malignancy. The FNAB cytology results were 12 false negative, one false positive, 4 true positive, and 150 true negative.
Thecytologyresultsof FNAB
wereasfollows: 25Vosensitivity, gg,3Vospeciticity, SO%.PI/,92,6VoPY-,and 92,2Voaccuracy. In another study of 41 cases of breast tumors we found 2 false negative, no false positive, 35 true positive, and 4 true negative. The FNAB cytologyresultswereasfollows: g4,62osensitivity,lN%specificity, IC/J,VoPIy',66,7%PV-,aad
95,lVou".uru.y.Keywords
:
FNAB, thyroid nodules, breast tumorsFine
needle
aspiration biopsy (FNAB) cytology,
theminimal-invasive procedure as
a
diagnostic tool in
human malignancies
have been usedworldwide
sinceits introduetion
in the early 1950's
in
Scandinaviancountries.
Theutility
of
FNAB have been
highly used,
andnearly
becomes atrend in
the
world
sinceit
is
asimple, quick,
and inexpensive method
to
biopsy
su-perficial
masses,usually
in
theoffice
or
clinic
setting.It
causesminimal trauma to the
_patientand
carriesvirtually
norisk of
complications.r
The
principal indication for FNAB of
thethyroid
is
asolitary
thyroid
nodule.
A
classic
multinodular
gland
israreiy
suipicious
for
carcinomu.2FNAB has
becomean extremely
popular
technique
for
the evaluation
of
solitary thyroid nodules. Most papillary
carcinomasand other types
of
malignancy other than follicular
carcinoma can be easily identified.
Beside
the
poor
cellularity
of
the
specimen
as a
general
problem in
Division of
Surgical Oncology, Head and Neck Surgery, Department of Surgery, Faculty of Med,icine, Padjad,jaranU niversity lHasan Sadikin Hospital, B andung, I ndonesia
FNAB due
to an inexperiencedphysician
as aprovider,
the main difficulty (and
this is specific problem for
thyroid
nodules)
is in
the
identification of
awell
dif-ferentiated
follicular
carcinoma
that may
be
impos-siblewith
this method. Theidentification
of afollicular
type
of
thyroid carcinoma, largely
depends
on
the presenceof
invasion
of
the
capsule,blood
vessels,or
adjacent
normal
thyroid
tissue.
Foci
of
capsular
in-vasion should be distinguished
from
capsular rupture
resulting from
a
fine-needle aspiration
procedure.Cytological interpretation of
a follicularneoplasm
aredistinguished
from
abenign nodule only by
thehigher
cellularity
of
normal
follicular
cells, which may
bevery
subjective.3Lukitto
To
know whether
FNAB
cytology could be
usedroutinely according to its sensitivity
and accuracy
in
the
Hasan
Sadikin Hospital, the two former
studieswhich have been performed
in
Bandung were
reevaluated.Fint
the study about itsutility
in diagnosisof
malignancies
of thyroid
nodules, and
second thestudy about
its utility
in
diagnosis
of
malignancies
of
breasttumors.
METHODS
TWo phases
of
studies
which
have beenperformed
in
the
Department
of
Surgery, Hasan
Sadikin
Hospital
Bandung, were
compared.During
thefirst
phase therewere 250 patients with
thyroid
nodules
which
were aspirated and sentfor cytological
examination,
âmongwhich
167 patientsunderwent thyroidectomy.
The lastspecimens
were sent for histopathological
examina-tion. The cytological findings and
histopathological
diagnoses
were
comparedblindly.
Thesurgical
proce-dureswere hcmithyroidectomy
for
unilateral
nodules andhemithyroidectomy
plussubtotal lobectomy
of thecontralateral side
in
bilateral
nodes.
If
the
his-topathological
finding
r"vçnlsdrma ligna ncy, thentotal
thyroidectomy
wasperformed.)
At
the second phase, 41 breast tumor
cases
were studiedby
FNAB
cytology.
The sampleinclusion
were new cases of breasttumorwhich
wereclinically
malig-nant
with a
diameter
of more
than
2 cm.
Inoperablecases underwent incisional biopsy,
while
operablecases
underwent
radical
mastectomy, and the
specimenswere
sentfor
routine histopathological
ex-amination.
Thecytological
andhistopathological
find-ingswere
compared
blindly.ÔThe
method
of
aspiration
technique
was the samefor
both
thyroid
nodules
aswell
as breast
tumors.
Thewritten informed
consent
for FNAB
was done before the procedure wasperformed
as recommendedby
theNational
CancerInstitute
Conferencein
USA.' With a
20ml
disposablesyringe
anda22-23
G needle,aspira-tion
was
performed
in thyroid
nodules
or breast
tumors
as onepuncture
at 3different
places.After
theneedle introduction
to the tumor, the plulger
wasretracted
to
create avacuum
in
the syringe.
With
theplunger
still
in
that position, the
needle was
movedback
and
forth in different
directions under
constantsuction
in
order to
detach the tissue fragments.In
thisposition the
needle was
withdrawn from the
nodule:The needle containing the
sample was detachedfrom
the syringe,
andthe content
of
the
needle wasblown
out on
a microscope slide by pushing down
theMedJ Ind.ones
plunger. By
using anotherslide
the specimen was then smearedthoroughly.
Sensitivity, specificity, positive predictive
value
(PV*),
negative
predictive
value
(PV-),
and accuracyof
the
two
studies
were
calculated, according
to
the standard formulas:8true-posi tives
Sensitivity =
x
1OO 4otrue positives+fa lse negatives
true-negatives
Specificity = xIOO%
true-nega tives+fal se-positives
true-positives
P\y'
= x IOOVotrue-positives + [a lse-posi ti ves
true-negatives
PV-
= x IOOVotrue-negatives + false-negatives
true-negatives
+
true-positiveAccuracy =
x
l0OVototal of cases
RESULTS
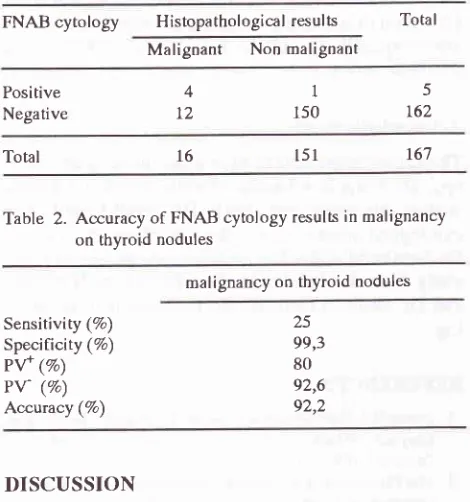
The
cytological findings
in 167
thyroid
nodule
caseswere
5positive malignant
and 162negative,
but
after
thyroidectomies the histopathological findings
were16 positive malignant and 151 negative. One
casewhich was
considered
malignant
on cytological
ex-amination,
turned out to be negative onhistopathologi-cal
examination (false
positive),
and 12
caseswhich
were considered negative on
cytological
examination
turned out to be
positive
onhistopathological
examina-tion
(false negative).
That
meansthe sensitivity
wasonly
257o,specificity
99,37o,PV+
SOEz,PV- 92,6%, and theaccuracy
was 92,27o.In 4l
breast tumor
cases
which
clinically
were
suspected
rnalignant,
thecytological findings
were
35positive, and
6
negative.
After
open
biopsy
for
in-operable cases andmastectomy
for
operable ones, thehistopathological examination revealed
37
positive
Vol 7, No 1 , J anuary - March 7998
Table 1. The outcome o[cytological (FNAB) and histopatho-logical (biopsy) tests of thyroid nodules
FNAB
cytology
Histopathologicalresults
TotalMalignant
NonmalignantFine neeille aspiration biopsy on thyroid nodules and breast lumors
Total
Table
2. Accuracy of FNAB cytology results in malignancy
on thyroid nodulesmalignancy on thyroid nodules
In
our
thyroid
series,FNAB cytology
had a
very low
sensitivity
(257o).That
mears
FNAB cytology in
theHasan
Sadikin Hospital is
not
sensitive
enough to
detect malignancy
in
a thyroid
nodule.
The high
ac-curacy (92,2%) obtained might
be due to thehigh
true negativeFNAB
cytology result (150/167).
Falsenega-tive in
this
series was 121167 (7,27o),which
washigh
enough
compare_d
to
2,27o
false
negative
in
Lowhagen's
series.ru Basedonly
on
theFNAB
cytol-ogy
results,
we
should
not perform
surgery
to
thosepatients according
to
the negative results. We
con-sidered that it
will
be
arisk for
the patients, because
they
will
still
have amalignancy
in their
body
which
was
not yet
detected.According
to
Caruso et a1,11 theaccuracy
of
cytologi-cal
diagnosis
of
thyroid
nodules
from FNAB
rangefrom
7O7oto 97Vo and was
highly
dependent
on
theskill
of
the
personperforming
the
biopsy
and that
of
the
cytopathologist interpreting it.
The result ofFNAB
were most commonly
divided
into the
following
categories: benign
or
negâtive, suspicious
or
indeter-minate (including all
follicular
neoplasms
or those
with
extensiveHurthle cell
changes),malignant
(papil-lary,
anaplastic,medullary,
andlymphoma),
andinsuf-ficient
sample.Their review of
thistechnique provided
insight into the
resultstypically
obtained at the
time
of
fine-needle
biopsy
of
the
nodules:
7O7o benign,4Tomalignant, 10%
suspicious,
and
l77o
as
insufficient
r"-p|".
Maxwell
et-all2 assessed
the
use and useful-nessof FNAB in their
hospital
in Chapel Hill,
North
Carolina, and found that
FNAB
in the workup
of
patients
with
thyroid
massesis
strikingly
underutil-ized,
while accurate
in
907o
of
cases
where
used,FNAB
appearsto play a minor role
in
the surgeon's
decision regarding
surgery.Our study showed that
FNAB on thyroid
nodulesresufted
in:
897o benign, 2,37omalignant,
0,57ofalse
positive,
and
7,27ofalse negative, and
the
accuracy 92,27o.According
to Carter,13 there are three typesof material
from
the breastwhich
can becytologically
examined.These
include nipple
secretions,
material
aspiratedfrom
cysts, andmaterial aspirated
from solid
tumors.Aspiration
of
solid
nodules of the
breast
is
highly
productive of rnaterial
that has goodresidual
morphol-ogy
colnparedto material
aspiratedfrom
nipple
secre-tion
andfrom
the cysts.This matter could
become theexplanation
of the second
phaseof our study in
breast(solid) tumors FNAB, where the cytological
resultswere
asfollows:
857omalignant,9,77o
berign,
4,87o false negative, and none falsepositive.
Positive Negative
4 12
1
150
5
t62
16',1
151
16
Sensitivity (7o)
Specificity (%) PV+ (%)
Pv' (%)
Accvacy (Vo)
25 99,3 80 92,6 92,2
DISCUSSION
FNAB cytology
alone as a diagnostic tool for athyroid
nodule was
unreliable in
detecting
thyroid
malignan-cies. Fraker
et
al9
suggested
ttrat tire
managementdecisions in thyroid
nodules
could be
based
on
theFNAB cytology
results as long
asit
is combined
with
the
clinical history.
The accuracy
of cytological
diag-nosis
is
highly
depeudent
on the
skill
of
the
personperforming
the
biopsy
and
the
cytopathologist
inter-preting
it.
Table 3. The outcome of cytological (FNAB) and histopatho-logical (biopsy) tests
ol breast tumors
FNAB cytology Histopathological resul ts Total
Malignant
NotmalignantPositive Negative
Table
4. Accuracy of FNAB cytology
results in malignancy of breast tumorsmalignancy in breast tumors 35
)
3560
4
4t 37
Tota
Sensiriviry (%) Specilicity (%) Pv+ (Vo)
Pv-(%)
Accuracy (%)
94,6
100 100
[image:3.595.48.283.113.364.2]Lukitto
A
main
issueof
FNAB
alone
in
detecting
breastcar-cinoma is
the falsenegative result.
Thelow
cellularity
and
poorly
preserved specimen have been responsiblefor falsely atypical
suspicious lesion in thente
of
1,27oto
1,67o..In areview of
theliterature,
the rangeof
false negative breastFNAB
in
palpable breast lesions variesfrom I7o
to
3I7o,
with
an
averagerate
of
l0%o.Trhis
rate
definitely
can be reduced bygaining
experiencein
the
technique
aswell
asinterpretation of breast
cytol-ogy.
False
positive findings
have reduced
the
rangefrom0-Il7oto0,l-O,2Vo
in an experienced hand,which
is
similar to
that reported
for
frozen section
examina-tion.14
Blichert-Toft
etall5
onbehalf
of
the EuropeanSociety
of
Surgical
Oncology (ESSO)
suggestedFNAB
as apart of
triple
assessmentin
detecting breastcarcinoma, together
with
the
clinical
findings
andmammography.
This
triple
assessment
of
breast
lesions was also recommended at theNational
CancerInstitute Conference
in
Bethesda,
Maryland,
USA,
September 1996,with
representatives of theAmerican
Sociely
of
Cytopathology,
Papanicolaou
Society
of
Cytopathology,
American
College
of
Radiology,
American College of
Obstetricians andGynecologists,
Society
of
Surgical Oncology, American Academy
of
Family
Physicians, College,of American
Patholo gists,National
Consortium
of
Breast
Centers,International
Academy of Cytology, American
Society
of Clinical
Pathologists, American Cancer Society, American
College
of
for Cyt
vedemons
atthe
Foundation
Curie-Institut
found
atotal
of
1529of
the
2772
(55%)
tumors were
diagnosed as carcinomaby aspiration biopsy.
After
incisional biopsy,
thediag-nosis
of
aspiration biopsy was confirmed
in
all
but
three.FNAB
therefore
missed carcinoma inLZToof
the
cases.From February 1992through
December
1994, at theMagee-Womens
Hospital
Breast CareCornult-ation Center,
therewere
1418 cases evaluated,during
which time
only
366
FNABs were performed.
Theaccuracy
for positive
diagnosis
was IO0%.rBOur series of
FNAB
in breast tumors showed quitehigh
in
sensitivity
and
accuracy
rate (94,67o and
95,ITo),even
this
was
still
a
small series
(41
cases).
Thespecificity and PV+ revealed
IOO%
iespectively
be-causeof
the sample
in this
serieswere
breast tumorswhich
were
clinically
malignant. According
to
Masoodl4
the diagnostic accuiacy
of
breast
FNAB
significantly improved
when a pathologist
examinedthe patients before the procedure was
performed.
Proficiency
in
the biopsy
technique, smear
prepara-tion,
aswell
asthe interpretation
of
thecytomorphol-ogy
are thekey factors
for
a successfulFNAB.
Med J Indones
Our
studies showed
that
FNAB
on thyroid
nodulesresqlted
in:
257osensitivity,
99,37o
specificity,
807oPi*),
92,67oPl-),
and
,iZ,ZEou..u.u"y,
while
theFNAB
on breasttumors resulted in:.94.6% sensitivitv.
lOOTospecificity,
tOO%op\y'*),
66,7%
p/-),
unj
95j%
accuracy.Acknowledgernent
The author is grateful
to
his trainee
in
surgical
oncol-ogy,
Dr.
Francisca Badudu,
for all
secretarial help
in
writing
this
paper, andalso
to Dr. Sjahir
Ismail,
as acytological
interpretator
in
thefirst
phasestudy
and toDr.
Sehabuddin, for datacpllecting
in the second phasestudy. I
am also indebted toProf.Dr.Sutisna Himawan,
andDr.
SantosoCornain,
for their
commentary
read-ing.
REFERENCES
1. Frable WJ. Fine Needle Aspiration Biopsy. In : Banks, pM, Kraybil l, WG,edl tors. Pathology for surgeon.. phi I adelphi a : Saunders, 1996:33-42.
2. Ttre Papanicolaou Society of Cytopathology Task Force on Standards of Practice. Guideline of the papanicol aou Society
of
Cytopathology for the examination of fine-needleaspira-tion
specimensfrom
thyroid
nodules. Modern pathol 1996;9:7IO-5.3. Rosai J. Ackerman's Surgical pathology. 8th ed. St. Louis: Mosby 1996: 493-567.
4. Rosai J. Ackerman's Surgical pathology. 8th ed. St. I-ouis: Mosby 1996: 1565-660.
5. Lukitto P, Ismail S, Iyad HA5 Rosadi R. Fine needle aspira. tion biopsy for deciding the malignancy of a thyroid nodule
in
Hasan Sadikin Hospital Bandung. In: Tjokronegoro A,Himawan S, Jusuf A, Susworo R, AzizMF, Djakaria M;êds. Cancer in Asia and Pacific: progress in clinical,
epiddmio-logical and biological aspects
of
cancer.Vol
1. Jakarta: Yayasan Kanker Indonesia, 1988:401 -8.6. Sehabuddin H. Nilai diagnostik biopsi aspirasi jarum halus
(BAIAH)
pada penderita tumor payudara yang secara klinis disangka ganas di RSU Dr. Hasan Sadikin Ba ndung (thesis). Bandung: Univ. of Padjadjaran, 1995.7. Final version: the unitorm approach
to
breast fine-needle aspi ra tion bi opsy. BreasrJ 1997
;3(4): I49 -6g.8. Greenberg RS. Medical epidemiology.
l't
ed. London: Appleton & l-ange, 1993:58479. Fraker DI, Skarulis M, Livolsi V. Thyroid tumors. In DeVita
VT,
Hellman S, RoSenberg SA, eds. Cancer principle&
practice ot oncology.Sth ed. phi ladelphi a : Li ppincot-Raven Publishers. 1997 : 1629 -52.
10. Lowhagen T, Gramberg PO, Lundell G, Shinnari p, Sunblad
R, Willem JS. Aspiration biopsy cytology
in
nodulesof
thyroid gland suspected to be malignant. Surg Clin N Am. Philadelphia: Saunders 1979; 59(t):3-18.
11. Caruso D, Mazzaferi EL. Fine needle aspiration biopsy in
Vol7, No
l,January
- March l9Q812. Maxwell JG, Scallion RR, White WC, Kotwall CAo Pollock H, Covington DL, et al. Fine needle aspiration cytology and
thyroid surgery in the community hospital.
Amer
J
Surg L996;I72:529-35.13. Carter D. Interpretati on of breast bi opsi es. New York: Raven Press 1984:7-18.
1.4. Masood S. Recent updates
in
breast fine-needle aspirationbiopsy. Breast J 1996;2(l):3-12.
15. Blichert-Toft
M,
SmolaMG,
CataliorriL,
O'Higgins N. European Societyof
Surgical Oncology. Principles and guidelines for surgeons -management of symptomatic breastcâncer. EurJ Surg Oncol
1997;23:l0l-9.
Fine needle aspiration biopsy on thyroid. nodubs and breast tumors
16. Harris J, Morrow
M,
NortonL.
Malignant tumorsof
thebreast. In DeVita VT, Hellman S, Rosenberg SAo editors.
Cancerprinciple & practice of oncology. 5thed. Philadelphia: Lippincott-Raven 1997: 155'7 -67.
I7.
T.ajdela A, Ghossein NA, Pilleron JP, Ennuyer A. Tbe valueof
aspiration cytologyin
the diagnosisof
breast cancer: experience at the Foundation Curie. Cancer 1975;35:499-506.18. Kanbour-Shakir
d
Harris KM, Johnson RR, Kanbour AI.Breastcare consultation center: role
of
the pathologist ina
multidisciplinary center.Diag
Cytopathol 19971,17(3):