178 Kosnadi Med J Indones
Creatinine
and Renal
Function
in
Children
Lydia Kristanti
Hartono Kosnadi
Abstrak
Pada utntnnnya laju sintesis kreatinin tetap dan ladar kreatinin plasma (PQ mencerminl<an laju eliminasinya melalui ginjal. Tiap anak sakit ginjal perlu diular faal ginjalnya untuk mengetahui berapa jauh penyakit itu telah merusak jaringannya. Tujuan penelitinn ini ialah menguJatr P1s danfaal ginjal atau
lajufiltrasi
glomerulus (LFG) yang dinyatalan oleh kliren inulin(Kiil
dan kliren kreatinin (K6) padaanak sakit ginjal, danmengetahuibagaimanahubunganantarakeduanya. Pada studibelah- lintang ini besar sampel dihitung dengan SarnpelTunggal untuk Esrtmasi Proporsi Suatu Populasi, dan analisk data dilakulan dengan Korelasi Produk Momen Pearson. Telahdilafukanpengukuran simultan Kindan Kw 112 anakdaribulanMaret 1991 sampai dengan Juli 1993. Hasil stuliinimenunjul<knn bahwa antara PIv dengan LFG yang dinyatalan oleh Kin dan Kw terdapat korelasi negatif hiperbolik pada semua anak denganfaal
ginjalcampuran(normald.anterganggu):Pur=4,34-0,03Kinft=-0,58;p<0,001;N=l12)d'anPw=4,72-0,0iKw(r=-0,60;
p<0,001;N=112).
Abstract
In most clinical conditions, the rate of creatinine synthesis remains constant and its plasma concentrarton retlects the rate of renal elimination. To lmow how
far
the kidneys have been damaged the renal function in children suffering f'rom renal diseases must be measured. The aim of this study was to measure plasma creatinine concentrations (Pc) and renal function or glomerularfiltration
rates (GFR) expressed by inulin clearance(Ciil
and cleatinine clearance (Cq) in children suffering from renal diseases, and to know how would be the correlation between them.In
this cross-sectional study sample size was estimated by the one-samplefor
estimating the population proporrton, and dan analyzing was done by the Pearson Product Moment Correlation. Simultaneous measurements of Cin andCctleyelsin 112 childrenwere done oyer theperiodfromMarch 1991n
JuIy 1993. Resultof this sudy showedtherewas ahyperbolic negative correlation between Pç1 and GFR in all children with mixzd (normal and decreased) renal functions ; Pcr-
4.34 - 0,03 Cin(r
= -0.58; p < 0.001 ; N =I
12) and Pcr = 4.72 - 0.03 C$ (r = -0.60; p < 0.001 ; N =I
12)Keyworils: Plasma creatinine, Inulin and creatinine clearances, Children
INTRODUCTION
Creatinine,
aproduct
of
creatine
and phosphocreatinemetabolism,
is synthesizedpredominantly in
theskele-tal
muscles.Creatinine
isexclusively
excretedthrough
the kidneys, predominantly
by
the
process
of
glomerular filtration
andto
a lesserextent
by
tubular
secretion.
In most
clinical
conditions,
the
rate
of
creatinine
synthesis remains constant
andits
plasmaconcentration reflects
the rateof
renal elimination.
IThe
importance of
measuringof
renalfunction
orGFR
in
children suffering
from renal
diseasesis to
know
how far
the
kidneys
havebeen
damaged,2 asGFR is
the aspectof
renalfunction
that correlatedclosely
with
Division
of
Pediatric Nephrology, Departmentof
Child Health, M edical Sc hool, Dipone goro Univ ersity/D r. Kariadi Ho spinl, S emaran g, In done siaability of
the kidneys
to
maintain the
composition
of
the bodyfluids within
the rangescompatiblé
with
life.3
Three methods
to
measureGFR
areinulin
clearance(Ci.)
(gold
standard),radioisotopic
clearance(C*)
(ac-curate) and
Ccr
(sufficiently
accurate).4'5There
arelimitations for
the
utility
of
theseclearance
methods.Cin takes a long time
to
perform,
the
procedure
isdifficult, very
expensive,
andit
is
not
practical
to
useit routinely in
theclinic.
Crais available
only in
awell
equipped
an
In
clinical
prac-tice GFR is
C"..5The aim
of
this study
was
to
measure
the levels
of
plasma
creatinine concentration (P".) dan GFR,
ex-pressedby
Cio and Ccrin
children suffering
from
renal
diseases,and
to know how would
be
the
correlation
between them.Creartnine and Renal Function 179 Vol 6, No 3, July - September 1997
2,3Vo
of
the hospitalized children,
of
which the
fre-quency
of
renal failure was
about
25Vo.6And
every
child in the community could suffer from
renal diseaseirrespective of the
socioeconomical class, education,
in
urban or
rural
area, and others.MATERIALS
AND METHODS
The procedures
of this
study were
in
accord
with
the"Pedoman
Etik
Penelitian Kedokteran
Indonesia".T
This
cross-sectional study
was performedin
children
suffering
from
renal diseases,admitted in
thehospitals
in
Semarang,boys
andgirls,
aged2-l4years. During
the
first
tïr/o years
of
life,
GFG continues
to
increaseand, based
on boy
surface
area, reachesadult
levels
between one to two yearsof
age.8Despite
the increasein
Pe'
GFR
corrected
for
body
surface area remains
nearly
constant and does
not
differ
significantly
be-tweenmale
andfemale subjects.e The sample
size was estimatedby
the one-samplefor estimating
thepopula-tion proporpopula-tion.'u
Measurements
of
the
standardGnll
andthe
conven-tional endogonous
Ccr5 were undertakensimultaneous-ly. A
solution
of
LÙVoinulin
as reagent was made by the methodof
CAS
9005-80-5.12Inilin
"on""ntration
in
plasma
(Pi")
(mg%o) andin
urine
(Uin)_\mgVo) were
assayed
by UV-method
for
D-fructose.rr
p",
(mgVo) andcreatinine concentration in urine
(Uç1) (mg7o) were assayed byAbbott
SpectrumAutoanalyzer. Urine
flow
was
V
ml
per
minute. Renal
clearance
formula
of
standar Cio
is
[(Uin
xV)
:Pin]
mllminlI.T3
m2 andthat
is
[(Ucr
x
V)
:
P"rJ as done by thePear-This
study was got
its Ethical
Clearance approvedby
the Research Teamof
Medical Faculty of Diponegoro
University
/Dr
Kariadi
General Hospiialin
Semarang.Written
informed
consent have been obtainedfrom all
the pediatric
patients'
parents.RESULTS
Simultaneous
measurementsof
standard Cin andcon-ventional
endogenous
Ccr wêre performed
in
L72
children
suffering
from
renal
diseases,admitted
in
theChildren Wards
of
al
Hospital,
Telogorejo
Hospital
Hospital in
Semarang,
age2-I4
68
(60.7Vo)boys and 44 (39.3Vo),over the
period from
March
1991to July
1993
(29
months).
Rangeof
the standard
Cin wasfrom
3to
I77 mllmintl.T3
m2 andof
theconven-tio,nal endogenous Cç1was
from
4to
196mllminll.73
m'.
Rangeof
Pcr wasfrom
0.23
to
15.g3 mg%o.There was a
hyperbolic
negative
correlation
between Pcr and GFR expressedby
Cin and Ccrin
children
with
mixed renal
functions (normal
and decreased) showedby the regression
equations I Ps1= 4.34 - 0.03
Cin(r
=
-0.58;
p
0.001;
5
=
112)
(Figure
l)
and Pcr=
4.72
-0.03 Ccr
(r = -0.60;
p
< 0.001;N
=
112) (Figure 2).DISCUSSION
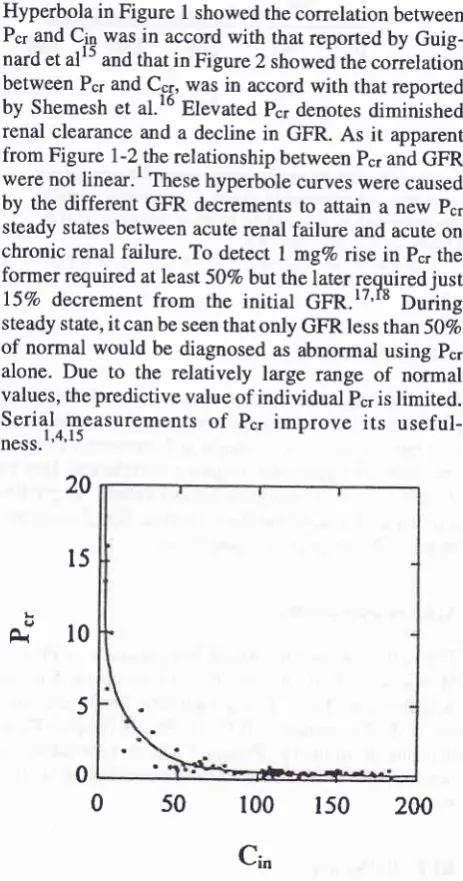
Hyperbola in
Figure
I
showed the correlation between Pcr and C-in wasin
accordwith
that reported
by
Guig-nard et
alls
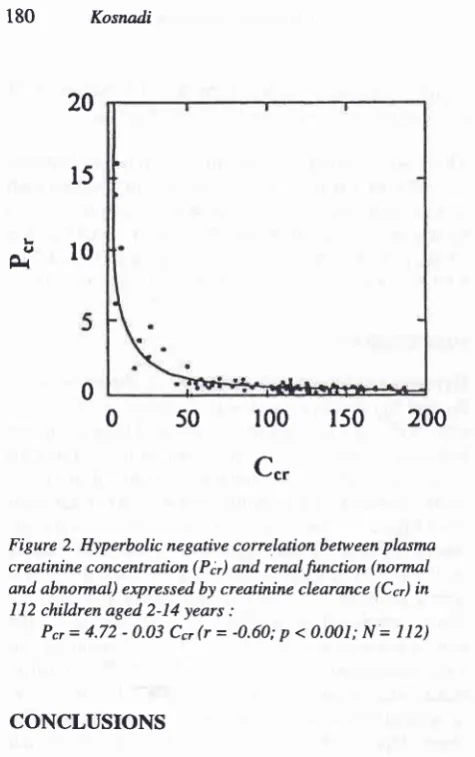
and thatin Figure 2 showeà the
correlation
between Pcr and C-s1, wâsin
accord
with
that reported
by
Shemeshet al.l6
Elevated
Pcr denotesdiminished
renal clearance and
a decline
in
GFR.
As
it
apparentfrom Figure l-2,the
relationship
between pcr andGFR
werenot
linear.'
These hyperbole curveswere caused
by the different GFR
decrements
to attain
anew
ps1steady states
between acute renal
failure
and acute onchronic renal
failure. To
detect
I
mg%orise
in p".
theformer required at least
507o but the later requirediust
l5Vo
decremenr
from
the
initial
GIR.l7'r8
ouiing
steady state,
it
can be seen that only GFR less than 50Voof normal would
be diagnosed as abnormal using
ps1alone. Due
to
the relatively large range
of
normal
values, thepredictive
value ofindividual
pcris
limited.
Serial
m,easurements
of
Psl
improve
its
useful-n"ra.1'4'15
È"
l0
20
t5
0 s0
100
lso
200
[image:2.595.293.525.234.675.2]Cin
Figure
l.
Hyperbolic negative correlation between plasma creatinine concentration(Pà
and renalfunction (Normal and Abnormal) expressed by inulin clearance(Ciil
in I 12 childrenaged2-l4years:
Pcr= 4.34 - 0.03
Cinft
= -0.58; p < 0.0A1; N =l12)
5
180 Kosnadi Med J Indones
2. van Collenburg J. Aspecten van (Gescheiden) Nier Functie Onderzoekbij Kinderen (Proefschrift). Rotterdam : Erasmus
Univemiteit, 1980.
3 . Liftchift MD . The Evaluation of Renal Function. In : Forland
M, editor. Nephrology. Bern : Huber Publishers,
1977:34-42.
4. Taylor CM. Assessment of Glomerular Filtration Rate. In :
Postlethwaite
RI,
editor. Clinical Paediatric Nephrology. 2nd ed. Oxford : Butterworth Heinemann, 1994:89-100. 5. KoeppenBM,
StantonBA. Renal Physiology.
lst
ed. StLouis : Mosby Year Book, 1992.
6. Lydia-Kosnadi, Tambunan T, V/ila ttr/irya IGN, Alatas H, Rauf S, Singadipura B, Sekarwana N, Bahrun D, Damanik M, Suryantoro P, Komang Kari I. PolaPenyakit Ginjal Anak
di Indonesia
-
Studi Kolaboratif. Dalam : Lydia Kosnadi,Santoso Soeroso, Hariyono Suyitno, editor. Disajikan pada
Simposium Nasional
IV
Nefrologi Anak. Fakultas Kedok-teran Universitas Diponegoro- Ikatan Dokter Anak
In-donesia Jateng, Semarang, Jtni23-211.,
1989-7. Sri Oemijati, Setiabudy S, Budiyanto
A.
Pedoman EtikPenelitian Kedokteran Indonesia. Jakarta : Fakultas
Kedok-teran Universitas lndonesia, 1987.
8. Moore ES, Aronson AJ, Northrup TE. The Assessment of
Renal Function. In
:
PostlethwaiteRI,
editor. ClinicalPaediatric Nephrology.
lst ed.
Bristol : Wright,1986:404-ll.
9. Schwartz GJ,
Brion LP, Spitzer
A.
The Useof
PlasmaCreatinine for Estimating Glomerular Filtration Rate in
In-fants, Children and Adolescents. Pediatr Clin North Amer 1987;34 (3):571- 90.
10. Madiyono
B, Moeslichan S, Sastroasmoro S, Budiman
I,Purwanto SH. Perkiraan Besar Sampel. Dalam
:
Sastroas-moro S, Ismael S, editor. Dasar-Dasar Metodologi Penelitian Klinis. Jakarta : Binarupa Aksara 1985:187-212.
11. Bohlin AB. Clinical Course and Renal Function in Minimal
Change Nephrotic Syndrome. Acta Paediatr Scan 1984;
73:631-6.
12. Reynold EF, Prasad AB. Inulin. In : Martindale - The Extra Pharmacopoeia. 28th ed. London
:
The PharmaceuticalPress, 1982: 520.
13.
Boehringer Mannheim Biochemical Analysis,
Food Analysis. D- Glucose/D-Fructose, 1990.14. Munro BH, Visintainer MA, Page EB. Statistical Methods
for
Health
Care Research. Philadelphia:
Lippincott,
1986:86-126.15. Guignard JP, Torrado A, Feldman H, Gautier F. Assessment
of Glomerular Filtration Rate in Children. Helv Paediat Acta 1980;35:437-47.
16. Shemesh O, Golbets H, Kriss JP. Limitations of Creatinine
as a Filtration Marker in Glomerulopathic Patients. Kidney
Int 1985;28:830-8.
17. Kassiger JP, Harrington JT. Laboratory Evaluation of Renal Function. In : SchrierRW, Gottschalk CW, editors. Diseases of the Kidney. 4th ed. Vol I. Boston : Little Brown, 1988 :
393-441.
18. Brezis
M,
Rosen, Epstein FH. Acuûe Renal Failure.In
:Brenner BM, Rector FCJr, editors. The Kidneys. 4th ed. Vol
I. Philadelphia : Sauders, 1991 :993-tr061.
20
l5
Ê.b
l0
0
0 50
100
150
200
[image:3.595.49.287.50.429.2]C..
Figure 2. Hyperbolic negative correlation between plasma creatinine concentration
(Pâ
and renalfunction (normal and abnormal) expressed by creatinine clearance(Cà
in1 12 chil^dren aged 2-14 years :
Pcr = 4.72 - 0.03
Ccrî
= -0.60; p <0.0il;
N=
112)CONCLUSIONS
In children
with
normal and decreased
renalfunctions,
plasma
creatinine
concentrations and glomerularfiltra-tion
rates, expressedby inulin
andcreatinine
clearan-ces, showed
hyperbolic
negative
correlation. Due
to
the
relatively
large rangeof normal
values, thepredic-tive
value
of individual
Pcr islimited.
Serial
measure-mentsof
P".improve its
usefulness.Acknowledgements
The
author wishes
to
extend
her
gratitude
to Prof
dr
Moeljono S Trastotenojo, Prof
Dr
dr Imam
ParsudiAbdulrochim, Dr
dr
Tonny Sadjimin,
Staffs
andNur-ses of the
Departments
of Child
Health,
PhaprosPhar-maceutical
Industry, Prodia
Clinical
Laboratory in
Semarang,
for
their
substantive
contribution
to
this
study.
REFERENCES
l. Kher
KK.
Evaluationof Renal Functions.
In :
Kher KK,Makker SP, editors. Clinical Pediahic Nephrology,
lst
ed.