Child psyChiatry and developmental disorders
mediCine 36:9 489 © 2008 published by elsevier ltd.
Autism spectrum disorder
in childhood
armin raznahan
patrick Bolton
Abstract
the term autism spectrum disorder (asd) refers to a group of child-hood onset neurodevelopmental disorders characterised by problems with social communication and repetitive behaviours. these conditions are increasingly recognised and often associated with marked disability across the lifespan. Whilst the causes of asd remain uncertain, it is clear that genetic factors play a major role. diagnosis should take place following a multidisciplinary assessment which also identiies individual strengths and weaknesses. as yet, there is no cure for asd, and few evidence-based options for the treatment of core-features – educational, behavioural and occasionally pharmacological interventions can be used to good effect.
Keywords autism spectrum disorder; child; development; pervasive developmental disorder
Clinical features
Autism spectrum disorder (ASD) includes the diagnoses of autism, Asperger’s syndrome and atypical autism which fall within the pervasive developmental disorder (PDD) category of ICD-10.1 All three diagnoses are characterized by the presence of:
• impairments in verbal and non-verbal communication • impairments in reciprocal social interaction
• the presence of restricted interests and repetitive behaviours. ASD diagnoses differ from each other in early developmental proile and symptom severity. Diagnostic criteria, important dif-ferential diagnoses, comorbid disorders and associated features are shown in Table 1. A key feature of ASD is its marked variabil-ity in presentation. This greatly impacts on academic and clinical approaches to ASD.
Epidemiology
Prevalence estimates of autism and ASD have shown a dramatic increase over the past 30 years: a recent UK study suggested that up to 1% of children may fulil criteria for an ASD (approximately
Armin RaznahanMRCPCH MRCPsych is a MRC Clinical Research Training Fellow at the Institute of Psychiatry, King’s College London, UK Competing interests: none declared.
Patrick BoltonPhD FRCPsych is a Professor of Child Psychiatry at the Institute of Psychiatry, King’s College London, UK. Competing interests: none declared.
0.3% autism, 0.2% Asperger’s syndrome, 0.5% PDD-other).2 This change is thought to be largely driven by increased public and professional awareness, and improved and altered diagnos-tic pracdiagnos-tice.3
ASD is more prevalent in males, although the sex ratio varies (M:F − autism 4:1, Asperger’s 10:1). There is no clear evidence that the prevalence of ASD differs as a function of socioeconomic status or ethnicity.
Aetiology
Autism shows the highest heritability estimates of any psychi-atric disorder (approximately 90%). The genetic inluences are complex, and so far no common genetic variants of major effect have been identiied. Non-genetic factors must also play a role as behavioural differences can be seen within affected monozygotic twins pairs. Despite many suggestions and much speculation, however, no clear environmental risk factors for ASD have so far been identiied.4
In approximately 10–15% of ASD cases, a primary medical disorder can be identiied (e.g. tuberous sclerosis, Fragile X syndrome). The remainder of cases are considered ‘idiopathic’ and thought to relect the combined action of multiple risk alleles for ASD. New approaches in genetic research, however, are changing our models for how genes might relate to behav-iour in ASD.5,6 Neuroimaging studies in people with ASD have found there to be early brain overgrowth, as well as structural and functional abnormalities within and between speciic brain regions (fronto-temporal cortices, limbic system, basal ganglia and cerebellum).7,8
Assessment
National guidelines available for ASD assessment adopt staged models.9,10 They emphasize the need for effective surveillance in primary care, the use of appropriate screening tools,11 and the beneits of diagnostic assessment being carried out in a mul-tidisciplinary team setting by experienced clinicians. The best validated and most widely used research-diagnostic instruments are the Autism Diagnostic Interview-Revised (ADI-R)12 and the Autism Diagnostic Observation Schedule (ADOS)13, and they can be useful in the diagnosis of complex cases. Readers are strongly advised to refer to the National Autism Plan for detailed guidance (Table 2).
Currently, the main purpose of physical investigations, such as genetic testing or brain scanning, in ASD is to aid
• there is postnatal brain overgrowth in the irst three years
• submicroscopic, structural chromosomal copy number variants are associated with autism
• there is no good evidence that mmr vaccine plays a role in aetiology
Child psyChiatry and developmental disorders
mediCine 36:9 490 © 2008 published by elsevier ltd.
identiication of an underlying medical disorder. Whilst there is some disagreement about exactly how and why to use such tests,14 most would agree that all children should have a karyo-type analysis carried out, and be tested for Fragile X syndrome. Further genetic tests and structural magnetic resonance imag-ing (sMRI) should be requested if there is evidence from history or examination of a neurogenetic syndrome (e.g. severe learn-ing disability, epilepsy, facial dysmorphology, neurocutaneous stigmata).
Management
General principles
Generic aspects of any management plan should include psycho-education, offering details of voluntary agencies and support groups, ensuring educational provision is appropriate and making sure carers and teachers are able to tailor their approach to the child in an ‘ASD-appropriate’ way pitching com-munications at the right level and using non-verbal means of
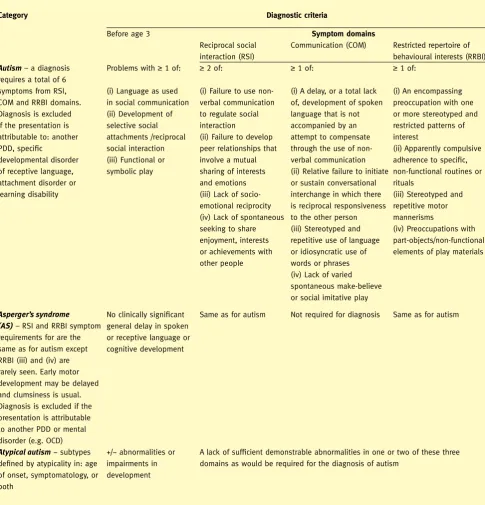
ICD-10 criteria for research diagnoses within the autism spectrum (abbreviated)
Category Diagnostic criteria
Before age 3 Symptom domains
reciprocal social interaction (rsi)
Communication (Com) restricted repertoire of behavioural interests (rrBi)
Autism – a diagnosis requires a total of 6 symptoms from rsi, Com and rrBi domains. diagnosis is excluded if the presentation is attributable to: another pdd, speciic
developmental disorder of receptive language, attachment disorder or learning disability
problems with ≥ 1 of:
(i) language as used in social communication (ii) development of selective social attachments /reciprocal social interaction (iii) Functional or symbolic play
≥ 2 of:
(i) Failure to use non- verbal communication to regulate social interaction
(ii) Failure to develop peer relationships that involve a mutual sharing of interests and emotions (iii) lack of socio- emotional reciprocity (iv) lack of spontaneous seeking to share enjoyment, interests or achievements with other people
≥ 1 of:
(i) a delay, or a total lack of, development of spoken language that is not accompanied by an attempt to compensate through the use of non- verbal communication (ii) relative failure to initiate or sustain conversational interchange in which there is reciprocal responsiveness to the other person (iii) stereotyped and repetitive use of language or idiosyncratic use of words or phrases or more stereotyped and restricted patterns of requirements for are the same as for autism except rrBi (iii) and (iv) are rarely seen. early motor development may be delayed and clumsiness is usual. diagnosis is excluded if the presentation is attributable to another pdd or mental disorder (e.g. oCd)
no clinically signiicant general delay in spoken or receptive language or cognitive development
same as for autism not required for diagnosis same as for autism
Atypical autism − subtypes deined by atypicality in: age of onset, symptomatology, or both
+/− abnormalities or impairments in development
a lack of suficient demonstrable abnormalities in one or two of these three domains as would be required for the diagnosis of autism
asd, autism spectrum disorder; ld, learning disability; pdd, pervasive developmental disorder; oCd, obsessive compulsive disorder.
Child psyChiatry and developmental disorders
mediCine 36:9 491 © 2008 published by elsevier ltd.
communicating if appropriate, fostering social skills, establishing structure in daily routines, being aware of sensory sensitivities. On a wider level there is a need to promote people’s understand-ing of ASD in order to reduce stigma in school, work and the community.
Psychosocial
There is insuficient data to draw any deinitive conclusions about the effectiveness and cost:beneit proile of psychosocial treat-ments aimed at targeting the core features of ASD, although it is generally felt that early behavioural interventions (EBI) have some beneits.15 However, there is a need to establish exactly which components of EBI lead to improvements in symptomatology and functioning, as well as the ideal intensity and setting within which EBI should be delivered. Work on psychosocial interven-tions based on basic neuropsychological research in ASD has only just begun.16 Learning theory based behavioural therapy can be effective in the treatment of maladaptive behaviours in ASD.
Pharmacological
There is some evidence that antipsychotic medications such as risperidone17 and selective serotonin reuptake inhibitor (SSRI) drugs (e.g. luoxetine) can be useful adjunctive treatments of maladaptive or restricted and repetitive behaviours in ASD. These treatments are not however without side effects (to which people with ASD may be especially prone) and should only be used in specialist care (see also pages 501–504).18
Prognosis
There is marked variability in long-term outcome in ASD, although impairments of one form or another tend to persist into adult-hood. As a result, a signiicant proportion of children with ASD remain dependent on others for support in adulthood. Those with normal intelligence and/or functional speech by the age of 5 years have the best outcomes,19 but the severity of social impairments and repetitive behaviours are also relevant in prognosis. ◆
REFERENCES
1 World health organization. mental disorders; a glossary and guide to their classiication in accordance with the 10th revision of the international classiication of diseases-research diagnostic criteria (iCd-10). Geneva: Who, 1993.
2 Baird G, simonoff e, pickles a, et al. prevalence of disorders of the autism spectrum in a population cohort of children in south thames: the special needs and autism project (snap). Lancet 2006; 368: 210–15.
3 Wazana a, Bresnahan m, Kline J. the autism epidemic: fact or artifact? J Am Acad Child Adolesc Psychiatry 2007; 46: 721–30. 4 rutter m. aetiology of autism: indings and questions. J Intellect
Disabil Res 2005; 49: 231–38.
5 ronald a, happe F, Bolton p, et al. Genetic heterogeneity between the three components of the autism spectrum: a twin study. J Am Acad Child Adolesc Psychiatry 2006; 45: 691–99.
6 sebat J, lakshmi B, malhotra d, et al. strong association of de novo copy number mutations with autism. Science 2007; 316: 445–49. 7 Geschwind dh, levitt p. autism spectrum disorders: developmental
disconnection syndromes. Curr Opin Neurobiol 2007; 17: 103–11. 8 palmen sJ, van engeland h. review on structural neuroimaging
indings in autism. J Neural Transm 2004; 111: 903–29. 9 Johnson Cp, myers sm, the Council on Children With disabilities.
identiication and evaluation of children with autism spectrum disorders. Pediatrics 2007; 120: 1183–215.
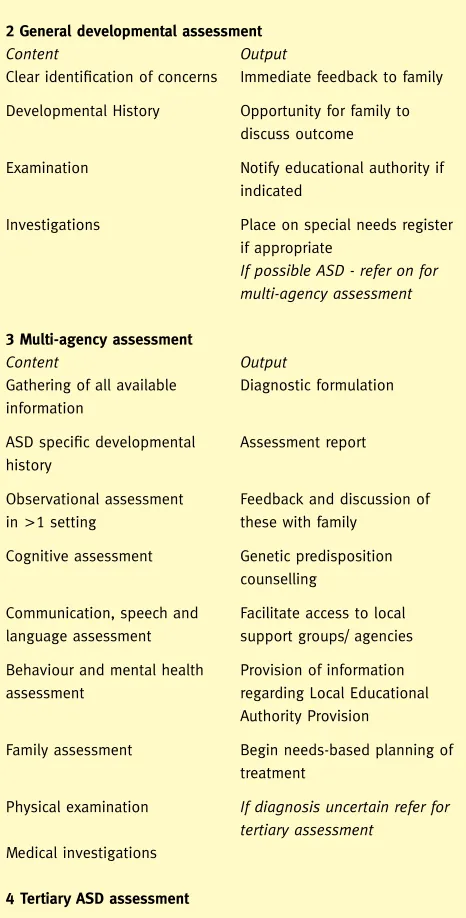
Simplified summary of recommended stages of
autism spectrum disorder assessment process as
outlined in the National Autism Plan
1 Identification of concerns
refer on for general developmental assessment
2 General developmental assessment
Content Output
Clear identiication of concerns immediate feedback to family
developmental history opportunity for family to discuss outcome
examination notify educational authority if indicated
investigations place on special needs register if appropriate
If possible ASD - refer on for multi-agency assessment
3 Multi-agency assessment
Content Output
Gathering of all available information
diagnostic formulation
asd speciic developmental history
assessment report
observational assessment in >1 setting
Feedback and discussion of these with family
Cognitive assessment Genetic predisposition counselling
Communication, speech and language assessment
Facilitate access to local support groups/ agencies
Behaviour and mental health assessment
provision of information regarding local educational authority provision
Family assessment Begin needs-based planning of treatment
physical examination If diagnosis uncertain refer for tertiary assessment
medical investigations
4 Tertiary ASD assessment
asd, autism spectrum disorder. see www.nas.org.uk for full details.
Child psyChiatry and developmental disorders
mediCine 36:9 492 © 2008 published by elsevier ltd.
10 le Couteur a. national autism plan for Children (napC), plan for the identiication, assessment, diagnosis and access to early interventions for pre-school and primary school aged children with autism spectrum disorders (asd). london: the national autistic society for niasa in collaboration with the royal College of psychiatrists, the royal College of paediatrics and Child health and the all party parliamentary Group on autism, 2003.
11 Charman t, Baird G, simonoff e, et al. eficacy of three screening instruments in the identiication of autism spectrum disorder. Br J Psychiatry 2007; 191: 554–59.
12 lord C, rutter m, leCouteur a. autism diagnostic interview-revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders.
J Autism Dev Disord 1994; 24: 659–85.
13 lord C, risi s, lambrecht l, et al. the autism diagnostic observation schedule-generic: a standard measure of social and communication deicits associated with the spectrum of autism. J Autism Dev Disord
2000; 30: 205–23.
14 schaefer GB, mendelsohn nJ. Genetics evaluation for the etiologic diagnosis of autism spectrum disorders. Genet Med 2008; 10: 4–12. 15 magiati i, Charman t, howlin p. a two-year prospective follow-up
study of community-based early intensive behavioural intervention and specialist nursery provision for children with autism spectrum disorders. J Child Psychol Psychiatry 2007; 48: 803–12.
16 aldred C, Green J, adams C. a new social communication intervention for children with autism: pilot randomised controlled treatment study suggesting effectiveness. J Child Psychol Psychiatry
2004; 45: 1420–30.
17 mcCracken Jt, mcGough J, shah B, et al. risperidone in children with autism and serious behavioral problems. N Engl J Med 2002; 347: 314–21.
18 malone rp, Gratz ss, delaney ma, hyman sB. advances in drug treatments for children and adolescents with autism and other pervasive developmental disorders. CNS Drugs 2005; 19: 923–34. 19 howlin p, Goode s, hutton J, rutter m. adult outcome for children
with autism. J Child Psychol Psychiatry Allied Disciplines 2004; 45: 212–29.
Practice points
• autism is the prototypical form of a spectrum of disorders that includes variants such as asperger’s syndrome
• autism spectrum disorder (asd) is found in around 1% of children
• asd is associated with various indices of neurodevelopmental abnormality such as macrocephaly, facial dysmorophology and epilepsy
• speciic probably causal medical disorders are identiied in a signiicant minority of cases (currently investigation identiies these conditions in approx 10% of cases)
• early behavioural intervention programmes may improve outcome, although autism spectrum disorder usually gives rise to persisting dificulties