48
Susalit and Sidabutar MedJ IndonesHaemodynamic and
Humoral
ProfÏles of Indonesian
Elderly
Hypertensive
Patients
Endang
Susalit, Radja
Pingkir
Sidabutar
Abstrak
Untuk nengerahui profil henodinamik dan hunoral penderita hipertensi usia lanjut, telah diselidiki 60 penderita hipertensi ( 30 berusia lebih dari 60 tahun dan 30 kurang dari 40 tahun ).Tekanan darah arteri rata-rata, jenis kelanin, tinggi dan berat badan kedua kelontpok setaraCurah jantung, indelcs jantung, frekwensi denyut jantung, aliran darah ginjal,laju
filtasi
glonerulus dan aktiftas renin plasma lebih rendah, sedangkan ukuran tebal septu,il dan dinding posterior ventrikelkiri, resistensi
vaskuler perifer total dan ginjal serta kadar peptida natriuretik atriutn plasma lebih tinggi pada penderita hipertensi usia lanjut. Disinpulkan bahwa hipertensi pada usia lanjut merupaknn penyakit dengan profil kardiah henodinanik dan hwnoral yang khas.Abstract
In an
attempt to investigate the haenodynatnic and hutuoral profile of the elderly hypertensive patients , 60 patients ( 30 olderthan
60 years and 3O youngerthan 41years
) were studied. The elderly patiena were natchedfor
nean arterial pressure, sex, height and weight with the younger patiens. Cardiac output, cardiac index, hearî rate, renal bloodflow, glomerularfiltration
rate and plasnn renin activity weresignificantly lower
in the elderly,
whereas total peripheral as well as renal vascular resistance, Ieft ventricular posterior wall, septal thickness and plasma atrial natriuretic peptide were higher. Itis
cottcludedthat
hypertension in the elderlyis a
distinct etltity with specific cardiac, haenrcdynanic and hunroral findings.Keywords : Hypertension, elderly, haenod7,17s111ic and hwnoral profile
INTRODUCTION
In
industrialized
societies, the prevalenceof
hyperten-sion
,in
patients
of
65
years
of age
or older is
over
50%,'
whereas
the present authors found the
pre-valenceof
hypertension
in
Indonesian
peopleover
60 yearsof age
is
around
30
%.
Because the prevalenceof elevated
blood
pressure
increaseswith
age2 and, becausethe
life expectancy of
theIndonesian
peoplewill
be much longer in thecoming years, the magnitude
of
theproblem
of
elderly hypertension in Indonesia
is expectedto
increase.For many years, the age related rise
in
blood
pressure
was considered
a
normal and inevitable
haemodynamic
consequence
of
growing
old.
This
belief
caused someauthorities
toadvocate therapeutic
nihilism for
elderly patients
with
hypertension.3However,
more recent datashow
that these pres-sure increasesare
associatedwith
risks
for
cardiovas-cularcomplications,4
and its treatment has been shownto
be
beneficial.s'o
National
High Blood Pressure
Education Program Working Group also had
maderecommendations
that
raised
blood
pressuresin the
elderly
and the
increasedprevalence
of
hypertension
in this population are
not
benign
occurrences
andshould not
beviewed
as a normalor
inevitable
conse-quenceof
aging.TFurthermore,there
is
increasing
in-terest
in
the
pathophysiology
of
hypertension
in the
elderly,becausethis understanding could
lead to bettermethods
of
control either through dietary
modifica-tions or use
of
drug
therapy.Some authors
have
suggested
that
clinical
andpathophysiological
findings
of
essentialhypertension
in
theelderly
arediffereni
f.o-
that
of
the-younger,sVol 4, No 1, January-March 1995
but
only
afew data is available to
support this concept.eThus,
in
an
attempt
to provide additional data, we
investigated
the
haemodynamic and
humoral
parametersin
the
elderly
hypertensive
patients
andcompared them with
younger adults.
We
matched
mean
arterial
x
d weight
with
c
compared
their
cMATERIALS
AND
METIIODS
We
investigated
60 essentialhypertensive
patients(30
older
than 60 years and 30 younger than40years). The
matching procedure
took into account mean arterial
pressure,weight, height
and age.patients
with essen_
tial diastolic
and isolated
systolic
hypertension were
included
in
this
study.
Somepatients
hadnever been
treatedfor
high blood
pressure,and in all others
an_tihypertensive
therapy
was discontinued
at
least 2
weeksbefore
thestudy.
The
patients were informed
of
the nature and purposeof
thestudy
and were askedto
give their
consent
to
participate.
patients with
malignant
or
accelerated
hypertension,
and/or
anyother
severeconcomitant pathologic condition
were excluded.Haemodynamic and echocardiographic
assess_ed out by
odlo using
resistancelated
by dividing effective
renal plasma
flow
by
theterm (1
- hematocrit).
Renal vascular
resistance wasderived from the
ratio
of
mean
arterial pressure
to renalblood
flow.
Plasma
renin
activity was measured
after
30minutes
of
sitting by radioimmunoassay
methods
usingcommercial
kit (Angiotensin
I-Bioteci
Radioim_ munoassayKit). Circulating
level of insulin
was deter_ernight
fasr by
t
Insulin).The
plasma concentrarion
of atrial
"",.r,Ti"",1"tiï:fi:
(HANP Kit Eiken)
and the amountof
catecholaminein
24-hour urine output
(Amicyl-Test
Katcombi).
A
two-tailed
t test
was used
to
compare
theelderly and
younger hypertensive
patients, and statis_tical significance
was presented as the meanRESULTS
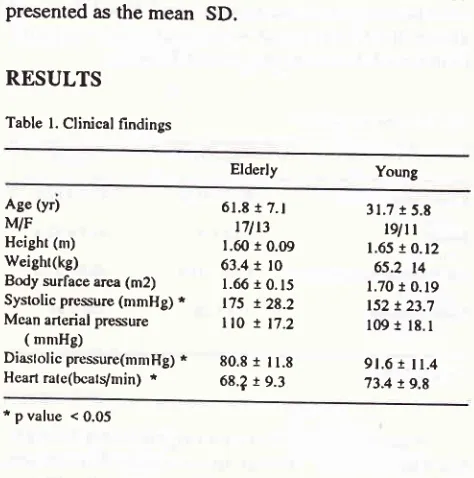
Table l. Clinical findings
Hypertension in the
Elderly
49calculated at
5 % level. Data aresD.
Elderly
youngAge (yr) WF Hcight (nù Weighr(kg)
Body surface area (m2) Systolic prcssure (mmHg) * Mcan arlcrial pressure
( mnrHg)
Diaslolic pressure(mnrHg) * Heart rate(bcats/min) *
6l.t
t 7.t
r7l t3 l.60 10.09 63.4t
l01.66
t
0. 15 175 !28.2ll0 r
17.280.8 1 I1.8 68.?
t
9.331.7
t
5.8tgltt
1.65 r 0.12 65.2 l4
1.70
r
0.19152
t
23.7109
t
18. I 9t.6r
il.4
13.4 !9.8 *pvalue <0.05The data
from
clinical
findings showed
thatelderly patients were
on average
around 30
yearsolder
than theyounger
subjects.younger patients (Table
1).Cardiac
output, cardiac index,
andstroke volume
were
significantly
lower in the elderly patients
thanin
theyounger
group.Echocardiographic
data showed
that
the left
ventricular
wall
and septum were
thicker
in
elderly
patients.Table 2. Haenrodynamic and echocardiographic findings
Eldcrly Young
Cardiac output (l/min) * Cardiac indcx (l/mirVm2) * Stroke volunre (nl) * LV wall thickness (mnr) * IV septal thickness (mnr) * Tolal peripheral resislance *
(unirs)
Rcnal blnod flow (ml/min) * Renal vascular resislance *
(unirs)
Glonrcrular fillralion rate * (ml/miry'l.73m2)
4.51
!
l.17 2.59t
0.5t 67.8!
t7.4ll.8
t
1.3 10.9r
3.324.9
!
7.4650
r
89170
r l8
87 !20
6.03
t
1.293.29
!
0.54 83.8r
t9.7 9.3!
2.O9.5
t
3.1l8.t
t
5.5lo57 !247 lo7
t
15l191 l8
[image:2.595.302.539.104.343.2]50
Susalit and SidabutarTotal
peripheral
and renal
vascular
resistance werehigher
in
theelderly,
and renal
blood
flow
andglomerular
filtration
ratewere lower
when
comparedto
those of the younger
group
(Table
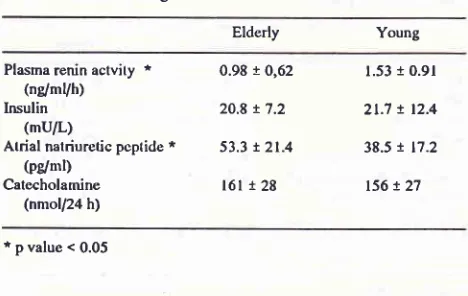
2).Table 3. Humoral findings
Elderly
YoungMed J Indones
which
peripheral
resistahce
is normal and
cardiac
index
is
increased. As
hypertension
progresses
,ffj:tffifi
l.,fsistance
gradually
increases andcardiac
Effects of
age on renal haemodynamics have alsobeen
studied.l3'T4
All
have shown
an
age-related
decline in renal blood
flow
and
glomerular filtration
rate. The decline in renal blood
flow in our elderly
hypertensive patients is not
a secondary phenomenon related to thefall
in cardiac output. In this study,
renalblood
flow
was
39 % lower
in
the elderly
patients,whereas
the
fall in
cardiac
output was
only
25
%,indicating a redistribution
of
cardiac
output
in
theelderly, probably resulting from
nephrosclerosis,
assuggested
by
the increasedrenal vascular
resistance. Schm.ieder etal,
reported
that
patients
with
es-tablished hypertension
have
anaccelerated decline
in
renal
perfusion
with
aging,
reflecting
selective
functional
or
structural
changesor both
in
renal
vas-cular
bed'15The renin-angiotensin-aldosterone
systemplays
a key role
in
salt and water
homeostasis and
in
theregulation
of
vascular tone. 16'17It
is
well
establishedthat renin
is
inversely
correlated
with
age.18 This
study
supports
other
reports
which
demonstrated
alower
plasma reninactivity
in
elderly
than inyounger
patients.g'19Imbalances
in
several neurotransmitters
andneuromodulators
are presentduring
the
development
of
hypertension
and
these
may
contribute
to
in-creased release
of
norepinephrine onto
thepostsynap-tic
targetsof
thesympathetic
nerves.20Esler et al
showed
that
reduced norepinephrine
reuptake increases the
overflow of the
neurotransmit-ter
to
plasma
from
the aging heartduring
stimulation
of
thecardiac sympathetic out
-flow.2l In
elderly
sub-jects,
baselinesympathetic
nerveactivity
per se seems to be increased, as shown by elevated levels ofcirculat-ing
catecholamines and
by a higher level
of
muscle'
sympathetic
nerveactivity
recordedby
microneurog-raphy.22 Thus, theelevation
of
plasmanorepinephrine
and exagerated responses tostimuli
in theelderly could
play
arole
in
hypertension.
In
this study
the
increase
of
24-hour urine
catecholamine
was
not significant. This result
is in
accord
with
the study
of
Goldstein et
al,
which
sug-gested
that the
age-effect
on
plasma norepinephrine
levels
wasobscured
in
hypertensive patients,
becauseof elevated value in
.21
thoseof
younger than in theelderly
suDJects.
The current
interest concerns
linking
hyperten-sion
to
hyperinsulinemia and
insulin
resistance
through increased
vascular
resistance. Both
animal
Plasma renin actvity *
(nglmVh)
Insulin
(mu/L)
Atrial natriuretic pcptide *
@g/nl)
Catecholamine (nmoU24 h)
0.98
t
0,6220.8
!
7.253.3
t
2t.416l 1 28
t.53
r
0.912t.7
!
12.438.5
t
17.2ts6
!
2l
ipvalue<0.05
Plasma
renin activity
was
significantly lower in
the
elderly,
and 24-hour
urine
catecholamine
wasslightly
but not
significantly
higher.
No
difference was
observed
in
plasma insulin
level, but
plasma
atrial natriuretic peptide was
sig-nificantly
higher
in
theelderly
(Table
3).DISCUSSION
With
advancing years, several changes
occur in
the anatomy andphysiology
of
thecardiovascular
system. These changesinvolve
both
the heart and thesystemic
vasculature.
The
major problem
instudying
theeffects
of
age andhypertension
on thecardiovascular
system,has been to
distinguish
age-relatedfrom
hypertension-related
changes
in
structure and function.
Severalreviewers
believe
that
elderly
hypertensives
repre-senta
unique
andgrowing
subset that
deservesspe-cial consideration.''
I IThe
results
of
this
study
suggests
that
the
pathophysiological
featuresof
essential hypertension
in the
elderly
differ distinctly
from
those in theyounger
patients.
In
theelderly,
essentialhypertension
ischar-acterised
by
ahypertrophied
heart, asscociated
with
a
low systemic
and
renalblood
flow, working
against ahigh total
peripheral
resistance.Indeed, the thicker
left ventricular
wall
and septum were found
in
theelderly
group.The
low
cardiac
output
results
from
both
asmaller stroke volume
and a reduced heartrate.
When
cardiac output declines
and
mean
arterial
pressureremains
unchanged
or
rises, total peripheral
resis-tance can be expected to rise. Several small
prospective
studies have
shown
thatearly
in
the courseof
[image:3.595.49.283.165.313.2]Vol 4, No l, January-March 1995
and
human
data support the idea
that insulin
resis-tanceis
associatedwith
enhanced pressorresponsive-,r"r".24
Further supports
come
from
Grunfeld
et al
who
found
the
time precedence
of
hyperinsulinemia
and
possibly
insulin
resistance over
the appearance
of
clinical
hypertension
in
a high-risk
population.2sAlthough we
observed
higher
total
peripheral
resis-tancein
theelderly
thanin
theyounger
subjects, therewas however
no difference in fasting
plasma
insulin
level
in
both
groups.Fasting plasma
insulin
and glucose
disposal
during
ahyperinsulinemic euglycemic
clamp maypro-vide different
estimates
of
insulin
resistance. Fastinghyperinsulinemia may reflect mainly hepatic insulin
resistance, whereas
impairment
of
glucose
disposalindicates
resistance to themetabolic
effects of insulin
in skeletal
muscle.26Dengel
et al usingthe
three-dosehyperinsulinemic euglycemic clamp
concluded
thathypertensive
obese,
sedentary older men have
areduction
in
both
sensitivity
andmaximal
responsive-ness toinsulin
which is
directly
relatedto
theseverity
of
hypertension, independent
of
obesity and physical
fitness.z /
Atrial
natriuretic peptide
was sequencedl0
years ago.28Berglund
et
alzÇ andJoshimurâ
et a1.30 shâwedgood
evidences that
atrial
pressuredetermines atrial
natriuretic
peptide concentrations,
whereasparkes
et alteported
that the increasein
atrial natriuretic peptide
is
gradual and
may be
dependenton the
gradual
in-creasein right atrial
pressure.r'
The accumulated
evidence indicates that atrial
natriuretic
peptideis
implicated in
thecontrol of blood
pressure,
body
fluid
homeostasis,and vascular
remodelling
as
both
cardiac
hormone
and local
regulator.32Thus, atrial natriuretic
peptide due
to its
renal,
endocrine
and
cardiovascular actions,
mayhave
a
physiological
role
in
theelderly
hyperten-sive
patients.In
this study,we
found
that plasmaatrial
natriuretic
peptide
was
significantly higher
in
theelderly as reported
by others.rr
Taken together,all
of
the
studies suggest
that an
age-related increase
in
plasma atrial natriuretic peptide
may
be present.CONCLUSIONS
Hypertension
in
the elderly
is
a distinct entity with
specific cardiac,
haemodynamic,
and humoral
find-ings.
Acknowledgements
The authors
wish
to
thank the
p.T.
Tanabe
Abadi
Jakarta,
Indonesia
for
the sponsorship.Hl,pertension in the
Elderly 5l
REFERENCES
1. Busse JC, Matterson BJ. Geriatric hypertension : the grow-ing use of calcium-channel blockers. Geriatrics 1988;43:
5
l-8.
2. Tell GS, Rutan GH, Kronmal RA et al.Correlates of blood pressure
in community-dwelling
older adults.The
car-diovascular health study. Hypertens ion L99 4;23 : 59 -67 .3. Flack JM, McVeigh G, Grimmy RH. Hypertension therapy
in the elderly. Cun Opin Nephrol Hypertens 1993;2:3g6-94. 4.
Ostfeld
AM,
Shekelle
RB,
Klawans
H, Tufo
HM.
Epidemiology
of
stroke in an elderly welfare population .Am
I
Public Health 1974;64:450-8.5, Pearce KA, Furberg CD. Hypertensive cardiovascular dis-ease and the treatment of hypertersion in the elderly . Curr
Opin Nephrol Hypertens 1994;3:2L3-7.
6. Freis ED. Prognosis in elderly hypertensive
patients.Medi-cal
Progress L995;22:14-8.7. National High Blood Pressure Education program Work-ing Group.National high blood pressure education program working group report on hypertension in the elderly. Hy-pertension 199 4;23:27 5 -85.
8. O'Malley K, O'Brien
E. Management of hypertension in theelderly. N Engl
I
Med 1980;302:1397-4O1.9. Messerli FH, Sundgaard-Ruse K, Ventura HO et al.Essential hypertension in the elderly: haemodynamics, intravascular volume, plasma renin activity,and circulating catecholamine levels. Lancet 1983;2:983-5.
10. O'Rourke RA, Hanrath P,Henry WN et al.Reporr of the Joint International Society and Federation of Cardiology / World Health Organization Task Force on recommendation
fot
standardization
of measurements
from
M-mode echocar-diograms. Circulation 1984;69:8544-7A.I
l.
Kirkendall WM, Hammond JI. Hypertension in the elderly.Arch
Intern Med 1980;140:1155-61.12. Post WS, L:rson MG, Levy D. Hemodynamic predictors
of
incident hypertension. Hypertension 1994;24:585-9O. 13. Papper S. The effects of age
in reducing renal function.
Geriatrics 197 3;28:83-7 .
14. Hollenberg NK,Adams DF, Solomon HS, et al.Senescence
and the renal vasculature
in normal man.
Circ Res 1974;34:309-16.
15. Schmieder RE, Schachinger H, Messerli FH. Accelerated decline in renal perfusion
with
aging in essential hyperten-sion. Hypertension 1994;23,,3 5 I -7 .16. Laragh JH.
fie
renin system and four linesof
hypertensionresearch. Hypertension 1992;20:267 -7 9.
17. Kruse HJ, Kreutz
R,
Staib S et al. Dissociationof renin
and aldosterone during low-dose epinephrine infusion. Am
J Hypertens 1994;7 :9
l3-8.
18.
Ho
GYF, BlaufoxMD, Smoller
SW etal.
plasma renin predicts success of antihypertensive drug withdrawal . Am JHypertens 19941,7 :679-84.
19. Swales JD. Low renin hypertension: nephrosclerosis?. Lan-cet 1975;i:75-7.
-52
Susalit and Sidabutar22. Veerman DP, Imholz BPM, Wieling W et al. Effects of aging
on
blood pressure variability in resting conditions.Hyper-tension t99 4 ;24 : l2O -30.
23. Goldstein DS, Lake CR, Chernow B. Age-dependence
of
hypertensives-normotensives
differences
in
plasmanorepinephrine. Hypertension 1983;5: 100-4.
24. Baron AD. Pathogenesis and measurement of insulin
resis-tance in hypertension. Cun Opin Nephrol Hypertens 1994;
3:631-5.
25. Grunfeld B, Balzareti M, Romo M et al . Hyperinsulinemia
in
normotensive offspring of hypertensive parents.Hyper-tension 1994;23(Suppl D:I 12-5.
26.
Hall
fE,
SummersRL, Brands
MW
etal. Resistance to
metabolic action
of
insulin andits
rolein
hypertension.Am
I
Hypertens 1994;1:772-88.27. Dengel DR, Pratley RE, Hagberg
IM
et al.Impaired insulinsensitivity and maximal responsiveness
in
olderhyperten-sive men. Hypertension I99 4;23 :32O-4,
28. Struthers
AD.
Effect
of
ACE inhibitors
on
the
atrialnatriuretic peptides in heart failure. Br Heart
I
1994;72:504.Med J Indones
29. Berglund
H,
Nyquist O, BeermannB
et al. Influence ofangiotensin converting enzyme
inhibition
on
the atrialnatriuretic peptide
atrial
pressure relationshipin
heartfailure.Br Heart
I
1994;72:521-1.30. Yoshimura
M,
YasueH,
TanakaH
et al. Responses of
plasma levels
of
A{ype natriuretic peptide
and
B-typenatriuretic peptide
to
alaceprilan angiotensin-convertingenzyme inhibitor
in patients
with congestive heart failure.Br Heart
I
1994;72:528-33.31. Parkes DG, Coghlan JP, Cooper EA et al. Cardiovascular
action ofatrial natriuretic factor in sheep with cardiac failure.
Am J Hypertens 1994;7:905-12.
32. Nakao K, Itoh H, Suga S et al. The natriuretic peptide family. Curr Opin Nephrol Hypertens 1993;2:45-5O.
33. McKnight
IA,
Roberts G, SheridanB,
et al.Relationshipbetween basal and sodium
-
stimulated plasma atrial