Savitri
Sayogo*,Sri
SukmaniahSudardjat., Sumedi
Sudarsono#,Riadi
Wirawant, S.i
Margono+,Lynne
CobiacNAbstrak
Penelitian
ini bertujuan untuk menilai suatu
cara intervensi dalam menurunkan prevalensi anemia pada kelompok rennja putri. Penelitian dilakuknn pada7I
siswi kelasI
danII
sekolah lanjutan tingknt pertann. Pengambilan sampel dilakukan dengan cara cluster, dengan kelas sebagai " cluster" , Intervensi yang diberikan berupa tablet yang mengandung 200 mg sulfas ferosus dan 0,25 mgasamfolat selama l0 hari berturut-turuî per bulan dalamjangka 3 buLan berurutan. Ukuran keluaran uîama status gizi berupa kadar
Hb,
feritin
serum dan indeks massa tubuh. Berdasarkan kadarfetitin
serunt dan Hb didapatkan bahwa defisiensi besi terdapat pada20Vo dan aemia defisiensi besi terdapat pada 5.7%
dari
subyek penelitian. Setelah penrberian suplementasi, didapatkan kenaikan bermakna baik pada kndarferitin
serum maupunHb.
Diperkirakart intervensiini
dapat merupakan strategi alternatif dalanr penanggulangan anemia pada remaja putri.Abstract
This study was undertaken to evaLuate the result of an intervention schente in reducûtg anenia in female adolescences. The study was
carried out in 7l female adolescences (students of the
first
and second year class, junior high schooll), which were taken using cluster sampling technique, with classes as clusters. The intervention was suppLementation of daily pills containing 200 mg sulphate ferrosus ahd 0.25 mgfolic
acidfor
a peiod of
I0
consecutive days monthlyfor
three consecutive ntonths. Tlæ supplementation wereadministered by the teacher at school during school days. Main outcome ,neasLtre was nutritional status i.e. the level of Hb, serurn ferritin as well as Body Mass Inder/BMI. Based on serum
ferritin
and hemogLobin level, around 20Vo of the subjects were classified as early state of iron deficiency/lb, while 5.77o of the subjects suffered from iron deficiency anaemio./lDA. After supplententatiotl, theserumlevel of
ferritin,
Hb, as well as the BMI sho+ved a signifcant increase. This intervention seenÆ to be effective as an altenrative strategy in reducing anemia infemale adolescences.Keywords: Nutritional status, iron pills, ID, IDA Vol 9, No 3, July
-
September 2000A study
on the
intervention
in
Curug,
Tangerang
Indonesia
still has
nationalnutritional
problems. Oneof
the problems
is nutritional
anemiai.e.
iron
deficiency
anemia
(DA).1
Anemia
is
a condition,
characterizedby
hemoglobin
(Hb) level below norïnal
range.2 Theprevalence
of
anemia
in
several
age groups
in
thecommunity is
still
high
i.e. between 40-
60Vo.3 Adolescences,consisting
of
active
individuals
with a
high growth
rate,will
determine thequality of
manin
'
DepartmentS
Nutrition Medicine,'Faculty of MedicineUniversity of Indonesia, Jakarta, Indonesia
t
Departmentof Community Medicine, Faculty
of MedicineUniversity of Indonesia, Jakarta, Indonesia
I Departmenr of Clinical Pathology, Faculty of Medicine
_ Universiry of Indonesia, Jakarta, Indonesia
I Departmen! of Parasitology Medicine, Facuby of Medicine University of Indonesia, Jakarta, Indonesia
s Division of Human Nutritio-n, CSIRO
Intervention scheme to reduce
anemia
175scheme
to
reduce anemia
tn
female
adolescences,
the
future. Therefore
it
is
necessary
to
assure
anoptimal growth
rate
in
this
group,
and
specialattention should
be paid
to
the
health
of
femaleadolescences,
who
aregoing to become mothers
in
thefuture.
There
is
little information available,
however,concerning
the iron
status
in
adolescence
and
the prevalenceof IDA.
The
main
cause
of
iron
deficiency
is
possibly
insufficient intake
of
iron
and
low
absorption
rate.Meanwhile, parasitic
diseasescaused
by
worms
or
malaria
parasites,
may worsen the
situation.o
Thereare
also
several determinant
factors which
influence
the prevalenceof
anemiaamong female
adolescencesi.e.
the economic
level
and
level
of
education
of
theparents.
176
Sayogo et alefforts
to
control
worrns were
already
done
in
elementary schools
in
the
cooperation
with
theDepartment
of
Parasitology,
Faculty
of
Medicine,
University of
Indonesia.One group
pre
andpost test design was
usedfor
this study.The study
was donefrom
Januaryto
September1998.
The
population was female
students
of
thegovemment
junior
high school (the
1"
and
2nd yearclass), age 12-15 years.
Subjects
were taken
usingcluster sampling
technique,
with classes
as
clusters.Sample
size
was calculated using
the
formula of
sample sizefor
related-test.s Theexclution criteria
for
the subjectsof this
study wereHb
level below
8 g/dl.Each subject was subjected
to
anintervention
scheme.The intervention was
supplementation
of
daily pills
containing
200
mg
sulphate
ferrosus and 0.25
mgfolic
acid
for
aperiod
of
10 consecutive daysmonthly
for
three consecutive
by
the
teacherat
school during
school
days.The
supplementation was
doneafter
theelimination of
intestinal helminths.
Home
visits
were done
to
obtain the
dataabout
socioeconomic status
and data
on the
dietary
intake.Furthermore,
body weight, height,
haemoglobinÆIb,and
serum
ferritin
before and after the
intervention
were also
measured.The
Hb
and
serumferritin
levelwere determined using the
cyanmeth6 andIRMAT
by
the
Department
of
Clinical
Pathology,
Medical
Faculty,
University
of
Indonesia.Data analysis was done using the related t-test,
usingSPSS
statistical
package
for
PC. Ethical
clearanceapplied
in
the
study was
approved
by
the
Ethical
Committee Medical Faculty,
University of
lndonesia.RESULTS
Out
of
75
subjects
who
were
selected,
2
were
excluded
from
this
study becausethey did not want
toparticipate,
while
2 subjects movedto
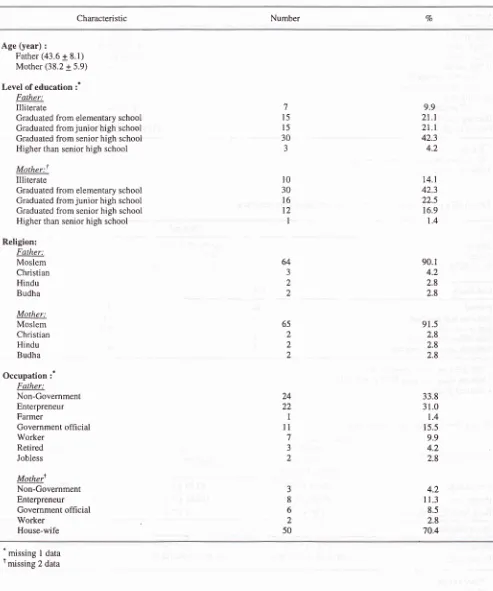
another class.Characteristics
ofthe
subjects
'The socio-economic
characteristic
of
'71 subjects were asfollow:
the
majority
of
the educational level
of
thefathers was
intermediate
(63.4Vo),while that
of
themothers was
low
(56.4Vo).The religion
of
90.l%oof
the
subjects
were
moslem; 64.87o
of
the
fathersworked
atnon government
sector,while
70.4Voof
the
mothers were housewives
(Table
1).Med J Indones
The number
of
the
family
members wasbetween
6-7persons.
Since there were difficulties
to
getinformation
about
the
income,
we
analyzed
theeconomic
level
using
their
monthly
expenditure.Using
theBiro
PusatStatistik criteria
for
expenditure,all of
the subjects hadlow economic
level.eTable 2 is
an
overview
of
the
general
characteristicsof
subjects.
Stunting
was found
in
28Vo
of
cases. Basedon BMIr0
13Voof
the
subjects
were
classified
underweight;86Vo
hadnormal
nutritional
status,while
obese wasfound
in
17oof
subjects.Table
3
is
an overview
of
dietary consumption
andiron
statusof
the
subjects.Further analysis using
2
x
24
hour recall method
revealed
that
nutrient
intake
was below
80Vo
of
the
recommended
dietary
allowances/RDA.rr Compared
to
theRDA,
the intake was 63Vofor
carbohydrate,
S4Vofor protein
and gl%ofor
iron
respectively.
Moreover,
the food pattem of
most
of
the
subjects showed
very
little
variation;
consumption
of vegetables
and
fruits
were
very
rare,as
well
as
the
consumption
of
protein and
iron
sources.
Using
food frequency
amountmethod,
it
was revealed also that theiron intake
wasvery
low
i.e.
4.7 mgdaily
(28Voof
theRDA).
Considering
the
consumption
of
food
it
can
beconcluded
that both
in
quality
and quantity
thenutrient intake was
not
adequate.
Furthermore,
theproportion
of
carbohydrate,protein
andfat
to
thetotal
calorie intake
were
56.8
+
9.0, 9.6
+
2.3,
and
30.25(median), respectively.
This
findings indicated
that the subjectsdid
not consume awell
balance diet.l2Hematologic data
Based
on Hb
and
serum
ferritin
parameters,
thesubjects
were
then
categoryzed
in
different
iron
status.r3
The distribution
is
shown
in
table
3, where
69.6Vo of
the
subjects
were
classified
as
having
normal
iron
status,while
iron deficiency
wasfound in
+
2OVoof
the subjects.Reassessment
of other variables
Before
the
reassessmentof
blood
and
anthropornetry parameters,stool examination
was done.The
result'of
stool examination
will
bepublished
in
another paper.The
results
of
blood
examination and anthropometry
Vol 9, No 3, July
-
September 2000Table 1. Distribution of study subjects according to socio-economic characteristics (n=7 I )
Intervention scheme to reduce anemia 177
Characteristic Number Vo
Age (year) :
Father (43.6 + 8.1) Mother (38.2 + 5.9)
Level of education :* Father:
Illiterate
Graduated from elementary school Graduated from junior high school Graduated from senior high school Higher than senior high school
Mother:t Illiterate
Graduated from elementary school Graduated from junior high school Graduated from senior high school Higher than senior high school
Religion: Falher: Moslem Christian Hindu Budha
Mother: Moslem Christian Hindu Budha
Occupation
:'
Father:Non-Government Enterpreneur Farmer
Government ofhcial Worker
Retired Jobless
Mothert Non-Government Enterpreneur Government official
Worker House-wife
7
l5
l5
30J
9.9
2t.t
2t.t
42.3 4.2t4.t
42.3 22.5 16.9 1.490.1 4.2 2.8 2.8
91.5 2.8 2.8 2.8
33.8 31.0 1.4 15.5 9.9 4.2 2.8
l0
30
l6
l2
I64
J 2 2
65 2
2 2
24 22 1
ll
7 J2
3 8 6 2 50
4.2 I 1.3
8.5 2.8 70.4
-
missing
I data
[image:3.595.81.574.99.690.2]I78
Sayogo etal
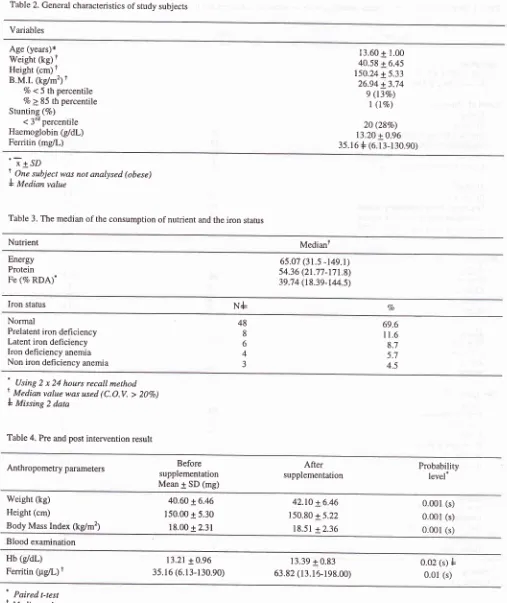
Table 2. General characteristics of study subjects
Med J Indones
Variables
Age (years)* Weight (kg)
f
Height (cm)t
B.M.I. (kg/m2)t %
<5 th percentile
Vo > 85 th percentile Stunting (%)
< 3'd percentile Haemoglobin
(g/dl)
Ferritin (mg/L)13.60 + 1.00 40.58 + 6.45 150.24 + 5.33 26.94 + 3.14 9 (t3Vo)
I
(l%o)20 (28Vo)
13.20 + 0.96 35.16 + (6.13-130.90)
-Ï+SD
t, One subject was not analysed (obese)
L Median value
Table 3. The median of the consumption of nutrient and the iron stahrs
Nutrient Medianl
Energy Protein Fe (% RDA)"
65.07 (31.s -t4e.t) 54.36 (21.77-171.8) 39.74 (t8.39-144.5)
Iron status
N+
VoNormal
Prelatent iron defi ciency Latent iron deficiency Iron deficiency anemia Non iron deficiency anemia
48
8
6
4 J
69.6 I 1.6
8.7 5.7 4.5
'
Using 2 x 24 hours recall methodt. M"dion value was used (C.O.V. >
207o)
I
Missing 2 dataTable 4. Pre and post intervention result
Anthropometry parameters Before
supplementation Mean
1SD
(mg)After
supplementation Probabilitylevel*
Weight (kg) Height (cm)
Body Mass Index (kg/m2)
40.60 + 6.46 150.00 + 5.30 18.00 + 2.31
42.10 + 6.46 150.80 + 5.22 18.51 + 2.36
0.001 0.001 0.001
(s) (s) (s) Blood examination
Hb (g/dl)
Fenitin (pg/L)
t
13.21+0.96 3s.16 (6.r3-130.90)
13.39 + 0.83 63.82 (13.15-198.00)
0.02 (s)
f
0.01 (s)^
Paired t-testt
Medianyalue [image:4.595.69.576.84.687.2]VoI 9, No 3, July
-
September 2000DISCUSSION
Characteristics
of the subjects
In
term
of
ecorbmic level,
all of
the
subjects
wereclassified as having
low
economic level (Table
1).This
condition
affects
the
nutrient intake
of
the subjects,since they
still
dependon
their family.
This
situation was
worsened
by
the fact that
56Voof
the
mothers had
low
educationlevel.
Uneducated motherslead
to
inability
to
absorb informations
regardinghealth, particularly
on
IDA. On the
other
hand,mothers have important
role on
the preparation of
meals
in
the family.
Considering
this
data,
we
may
conclude that most
of
the
subjectscould be classified
as
having
low
socioeconomic level.
This
conclusion
is
supportedby the overview
of
thegeneral characteristic
of
the
subjectswhich could
beseen
in
table2. The
high
rateof
stunting
(28.2Vo)is
amanifestæion
of
previous
chronic poor health
andnutrition condition, which has
been regarded
as
anintemlav between nutrient intake
and
infection
in
"urty
of
stunting
tii".to Nutritional
process
than
factors
the ethnic
are a moreor
genetic
likely
causeback,
ts" '
grouno.
Hematologic data
Iron
deficiency
refersto
a statein
which
thebody iron
stores
have been depleted,
while
IDA
refers
to
ahematologic
statusresulting
from
iron deficiency.
Theoccurance
of
IDA
implies that body
iron
stores
areseverely depleted.r6
Table
3
shows
that from the total
sample,
69.6Voof
the
subjectswere normal, non anemic
iron
deficiency
were
20.3Vo,while
the prevalence
of
IDA
was 5.1Vo.These
findings indicate
that
in this
study
iron
deficiency was
still
anutritional
problem
(267o).It
isobvious
that not
all
anemia
is
causedby the lack of
iron.
There were
3
subjects (4.5Vo)who did not
meetthe criteria
of IDA.
These subjects showed
that
the cauesof
the
low Hb level
was dueto
something else.For
example
vitamin
Bo
deficiency,
vitamin
B12deficiency
or
due
to a
chronic
disease. However,
further
analysisshould
be doneto
determinethis
kind
of
anemia.With
regardto
iron
deficient
status,dietary supply
hasto
be
taken
into
consideration.
It
is
known that
thedietary supply of iron is
determinedby
3main
factors:total
iron
intake, content
of
hemeiron
taken
and theIntervention scheme to reduce
anemia
179bioavailability
of
the
non-heme iron.rT
Before
inter-vention,
the percentageof low
plasmaferritin is
quite
high
(26Vo).This condition could be
caused
by
theincreasedphysiologic
d
,expanding
redcell
mass, basalloss
8At
the end of the supplementation, several points could be noted:1.
There were anevident significant
increaseof
both
serum
ferritin
andHb
level.
2.
The
increasein
weight
as
well
as
BMI
indicate
increased
dietary
energy
intake
due
to
increased appetiteattributed
to theintake
of
supplement.3.
The
increase
in
height can
be
attributed
to
thenormal
increasein
height
of
adolescence. Increasein
height due
to
iron
supplementation
was
alsoobserved
in
oreschool
children''
and
schoolchildren.20
In
public
health programs,
impact
evaluation
is
very
important.
In
this study,
after theiron
supplementationthere
was
a
decrease
in
the
prevalence
of
iron
deficiency.
Regarding
the
food
consumption
of
the subjectsit
can
be
concluded that
the quality
and
thequantity
were
not
adequate.
On the
other
hand,prolonged poor Fe intake combined
with
increasediron
losses
due
to
menstruation may pose as risk
factors
of
anemia.Therefore,
iron
supplementation
asan immediate solution,
remains
the
mainstay
in
thestrategy
of
controlling
iron
deficiency/ID and IDA.
Supplementation aspreventive
strategyshould
also beimplemented
in this high risk
adolescencegroup
(thelow
socio-economic
level). The result
of
our
studyshowed
that
the
intervention
is
effective
as
analternative
strategyof
controlling ID
andIDA.
CONCLUSION
The
method
of
the
intervention
was
effective
in
reducing
anemia aswell
asthe
causeof
improvement
of
thenutritional
status.Acknowledgement
Our gratitude is
extendedto
all who
were
involved
inthis
study and
who
made the course
of
this
researchpleasant and smooth.
Our
thanksto
theformer
Rector
(Prof.
Dr.
M.K.
Tadjudin)
and
Rector
of
theUniversity of
Indonesia (Prof.
Dr. A.R. Budi
Santoso,MD),
CSIRO,
the
Health
Officials
of
Kabupaten Tangerang and Puskesmas KecamatanCurug,
and theteachers and students
of
the Govemment Junior
High
School Curug,
for
the good cooperation and financial
180
Sayogo et alREFERENCES
l.
Depatemen KesehatanRI. Profil
kesehatan Indonesia.Jakarta: Departemen Kesehatan, 1993; 66-9.
2.
World Health Organization. Nutritional anernias. Report of WHO Scientific Group. Geneva: WHO, 1972; 5-10.3.
Kodyat BA, Thaha RA, Minarto. Penuntasan masalah gizikurang.
In:
Risalah Widyakarya Pangan danGizi
VI.Jakarta: LIPI, 1998; 7 55-66.
4.
Mahdin
AH,
SuhamoD,
HusainiYK,
Siagian LU,Harahap H, Wijayanti TF, et al. Study nutritional anemia an assessment of information complication for supporting
and formulating national
policy
and program. Jakarta: Departemen Kesehatan, 1989; I l-12.5.
MadiyonoI,
Purwanto HS. Perkiraan besar sampel. In: Sastroasmoro S, Ismail S, eds. Dasar-dasar metodologi peneliti an klinis. Jakarta: Binarupa Aksara, 1 99 5 : 19 4 -5.6.
Boehringer Manheim
GmBH.
Diagnostica
TextCombination
Haemoglobin.
Manheim:
BoehringerManheim GmBH, 1984.
7.
Anonymous. Operator's manualK-1000. Kobe:
Toa Medical Electronics, 1991.8.
Abidin SA, Rasad R. Pengobatan infeksi nematoda usus dengan mebendazol 500 mg dosis tunggal. Medika 1990; 3 :192.9.
Biro
Pusat StatistikRI.
Pengeluaranuntuk konsumsi
penduduk Indonesia
per
propinsi. Jakarta:Biro
pusat Statistik, 1996; Buku 3 tabel 2.10.
WHO. Adolescent.In:
WHO. Physical status: The useand interpretation
of anthropometry.
WHO
TechnicalReport Series. Geneva: WHO, 1995; 263-306.
ll.
Med J Indones
Muhilal, Jus'at
I,
Husaini, Djalal F, Tarwodo Ig. Angka kecukupangizi
yang dianjurkan.In:
Rivai
MA,
ed.Risalah
Widyakarya Pangandan Gizi
V.
Jakarta:Lembaga Ilmu Pengetahuan Indonesia 1994;432.
Departemen Kesehatan RI. Panduan 13 pesan dasar gizi seimbang. Jakarta: Depkes RI, I 995; I I -4.
13. Wick
M,
PinggeraW,
Lechmannp.
Ferritin
in iron
metabolism, diagnostic strategies. New
york:
Springer-Verlag,l99l;l-48.
Martorell
R,
Khan
K, Schroeder
D.
Reversibility ofstunting
epidemiologicalfrndings
in
children
from developing countries. Eur J Clin Nutrition 1994; 48 suppl.l:
S 45-57.Karlberg
J,
JaklF,
LamB, Low
L,
JeungC.
Linear growth retardation to three phases of growth. Eur J Clin Nutrition 1994: 48 suppl. I : S 25-44.Cook JD, Finch CA. Assessing iron status of a population. Am J CIin Nutrition 1979:32:2115-9.
De
MaeyerEM,
DallmanP,
GurneyJM,
Hallberg L,Sood SK, Srikantia SG. Preventing and controling iron deficiency anemia through primary health care. Geneva: WHO, 1989; 14-5.
Dallman
P.
Changingiron
needsfrom birth
through adolescence.In:
Folmon SJ,Zlotkin
S eds. Nutritional anemias. New York: Raven Press, 1992;29-35.Angeles
lT,
Schulrink
W,
Marulessyp,
Gross R,
Sastroamidjojo S. Decreased rate of stunting through iron supplemenration. Am J Clin Nutrition 1993; 5g: 339-42. ChwangL,
SoemantriA, Pollit
E. Iron supplementation and physical growthof
rural Inclonesian children. Am JClin Nutrition 1988; 47: 496-501. t2
t4
15
l6
17
l8
l9