Informasi Dokumen
- Penulis:
- Reynanta
- Pengajar:
- Dr. Binarwan Halim, Sp.OG(K)
- Dr. M. Fidel Ganis Siregar, Sp.OG
- Sekolah: Universitas Sumatera Utara
- Mata Pelajaran: Obstetri dan Ginekologi
- Topik: Hubungan antara Infeksi Chlamydia trachomatis dengan oklusi tuba yang dideteksi dengan HSG pada wanita infertil
- Tipe: tesis
- Tahun: 2011
- Kota: Medan
Ringkasan Dokumen
I. PENDAHULUAN
Bagian ini membahas latar belakang penelitian yang menyoroti pentingnya memahami hubungan antara infeksi Chlamydia trachomatis dan oklusi tuba pada wanita infertil. Infertilitas adalah masalah umum yang mempengaruhi banyak pasangan, dan infeksi Chlamydia trachomatis sering kali menjadi penyebab yang tidak terdiagnosis. Dengan adanya data epidemiologi yang menunjukkan prevalensi infeksi ini, penelitian ini bertujuan untuk memberikan wawasan yang lebih baik mengenai faktor risiko yang berkontribusi terhadap infertilitas, serta untuk mengembangkan pendekatan diagnostik yang lebih efektif.
1.1. Latar Belakang
Latar belakang penelitian menjelaskan bahwa infertilitas mempengaruhi 10-15% pasangan usia reproduktif. Penelitian ini penting untuk mengidentifikasi peran infeksi Chlamydia trachomatis dalam menyebabkan oklusi tuba, yang dapat mengarah pada infertilitas. Dengan pemahaman ini, diharapkan dapat meningkatkan kesadaran akan pentingnya skrining dan diagnosis dini untuk mengurangi angka infertilitas.
1.2. Rumusan Masalah
Rumusan masalah dalam penelitian ini berfokus pada pertanyaan apakah ada hubungan signifikan antara infeksi Chlamydia trachomatis dengan oklusi tuba pada wanita infertil. Ini mencakup pertanyaan tentang proporsi infeksi dalam kelompok wanita dengan oklusi tuba dibandingkan dengan wanita yang memiliki tuba normal, yang akan membantu dalam memahami dampak infeksi ini pada fertilitas.
1.3. Hipotesis Penelitian
Hipotesis penelitian menyatakan bahwa terdapat hubungan positif antara infeksi Chlamydia trachomatis dan oklusi tuba pada wanita infertil. Penelitian ini berusaha untuk menguji hipotesis tersebut melalui analisis data yang diperoleh dari pemeriksaan HSG dan tes serologi.
1.4. Tujuan Penelitian
Tujuan utama penelitian ini adalah untuk menilai hubungan antara infeksi Chlamydia trachomatis dengan oklusi tuba pada wanita infertil. Selain itu, penelitian ini bertujuan untuk mengevaluasi proporsi infeksi dalam kelompok wanita dengan oklusi tuba dibandingkan dengan yang memiliki tuba normal, yang dapat memberikan informasi penting bagi praktik klinis.
1.5. Manfaat Penelitian
Manfaat dari penelitian ini termasuk memberikan data yang dapat digunakan untuk meningkatkan skrining dan diagnosis infeksi Chlamydia pada wanita infertil. Hasil penelitian diharapkan dapat memberikan kontribusi terhadap pengembangan pedoman klinis untuk penanganan infertilitas yang lebih baik.
II. TINJAUAN PUSTAKA
Bagian ini menyajikan tinjauan literatur terkait infertilitas, infeksi Chlamydia trachomatis, dan metode diagnostik yang digunakan untuk mendeteksi oklusi tuba. Tinjauan ini mencakup definisi infertilitas, etiologi, sejarah dan epidemiologi Chlamydia trachomatis, serta patogenesis dan manifestasi klinisnya. Selain itu, bagian ini juga membahas hubungan antara infeksi ini dengan infertilitas tuba, serta pemeriksaan patensi tuba seperti HSG.
2.1. Infertilitas
Infertilitas didefinisikan sebagai ketidakmampuan untuk hamil setelah satu tahun berhubungan seksual tanpa kontrasepsi. Terdapat dua jenis infertilitas: primer dan sekunder, dengan berbagai faktor penyebab yang dapat mempengaruhi kesuburan. Memahami etiologi infertilitas sangat penting untuk diagnosis dan penanganan yang tepat.
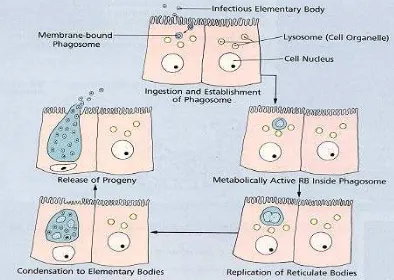
2.2. Chlamydia Trachomatis
Chlamydia trachomatis adalah infeksi menular seksual yang paling umum, sering kali tidak terdiagnosis karena asimptomatik. Infeksi ini dapat menyebabkan penyakit radang panggul dan oklusi tuba, sehingga mempengaruhi kesuburan. Tinjauan ini mencakup sejarah, morfologi, dan faktor risiko terkait infeksi ini.
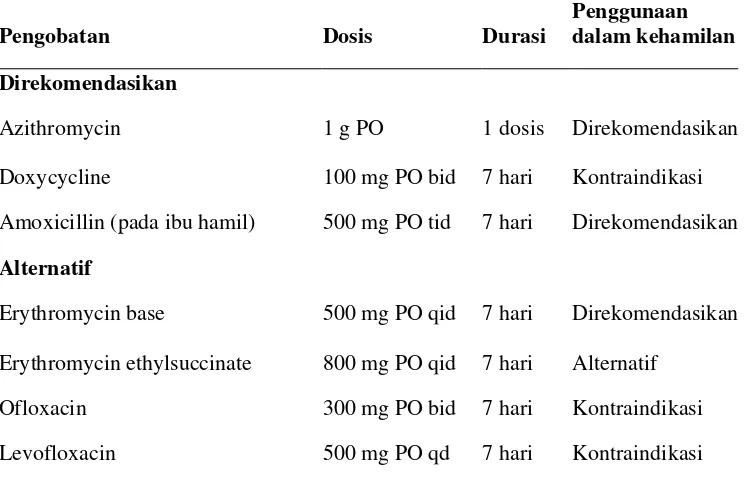
2.3. Tes Diagnostik
Berbagai metode diagnostik digunakan untuk mendeteksi infeksi Chlamydia trachomatis, termasuk kultur, pengujian sitologi, dan serologi. Tes serologi, terutama untuk antibodi IgG, dapat menjadi indikator penting untuk menentukan paparan sebelumnya terhadap infeksi ini, yang relevan dalam konteks infertilitas.
2.4. Hubungan Chlamydia dengan Infertilitas Tuba
Terdapat bukti yang menunjukkan bahwa infeksi Chlamydia trachomatis berkontribusi terhadap oklusi tuba, yang merupakan salah satu penyebab utama infertilitas pada wanita. Penelitian ini mengkaji hubungan ini lebih dalam, dengan fokus pada prevalensi infeksi dalam kelompok wanita infertil.
2.5. Pemeriksaan Patensi Tuba
Histerosalpingografi (HSG) adalah metode yang umum digunakan untuk menilai patensi tuba. Metode ini membantu dalam mendiagnosis oklusi tuba dan memberikan informasi penting dalam konteks penanganan infertilitas. Bagian ini juga membahas kelebihan dan kekurangan dari berbagai metode pemeriksaan.
III. METODE PENELITIAN
Bagian ini menjelaskan desain penelitian yang digunakan, termasuk lokasi, waktu, dan metode pengambilan sampel. Penelitian ini merupakan studi analitik komparatif dengan pendekatan potong lintang, yang dilakukan pada wanita infertil yang menjalani pemeriksaan HSG. Kriteria inklusi dan eksklusi juga dijelaskan untuk memastikan validitas hasil penelitian.
3.1. Desain Penelitian
Desain penelitian ini adalah studi analitik komparatif dengan pendekatan potong lintang. Penelitian dilakukan untuk membandingkan wanita infertil dengan oklusi tuba dan tuba normal, dengan tujuan untuk menilai hubungan antara infeksi Chlamydia trachomatis dan oklusi tuba.
3.2. Tempat dan Waktu Penelitian
Penelitian dilakukan di beberapa rumah sakit dan klinik di Medan, termasuk RSUP H. Adam Malik dan Halim Fertility Centre, selama periode Maret 2010 hingga Januari 2011. Pemilihan lokasi ini bertujuan untuk mendapatkan sampel yang representatif dari populasi wanita infertil.
3.3. Sampel dan Besar Sampel Penelitian
Sampel penelitian terdiri dari wanita usia reproduktif yang mengalami infertilitas. Kriteria inklusi mencakup wanita yang tidak memiliki riwayat operasi yang dapat mempengaruhi hasil, sementara kriteria eksklusi mencakup kondisi seperti mioma uteri dan endometriosis. Sampel diambil secara konsekutif untuk memastikan keakuratan data.
3.4. Cara Kerja
Prosedur penelitian melibatkan pengambilan sampel darah untuk pengujian serologi dan pemeriksaan HSG untuk menilai patensi tuba. Data yang diperoleh akan dianalisis secara statistik untuk menentukan hubungan antara infeksi Chlamydia trachomatis dan oklusi tuba.
3.5. Alur Penelitian
Alur penelitian dimulai dengan seleksi peserta berdasarkan kriteria yang telah ditentukan, diikuti dengan pengambilan sampel darah dan pemeriksaan HSG. Data yang diperoleh akan dicatat dan dianalisis untuk menentukan prevalensi infeksi dan hubungannya dengan oklusi tuba.
IV. HASIL DAN PEMBAHASAN
Bagian ini menyajikan hasil penelitian yang diperoleh dari analisis data, termasuk karakteristik peserta, hubungan antara infeksi Chlamydia trachomatis dan oklusi tuba, serta keterbatasan penelitian. Hasil menunjukkan adanya hubungan signifikan antara infeksi dan oklusi tuba, yang memberikan wawasan penting untuk penanganan infertilitas.
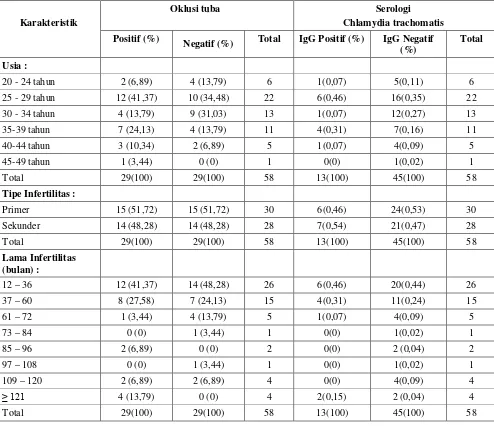
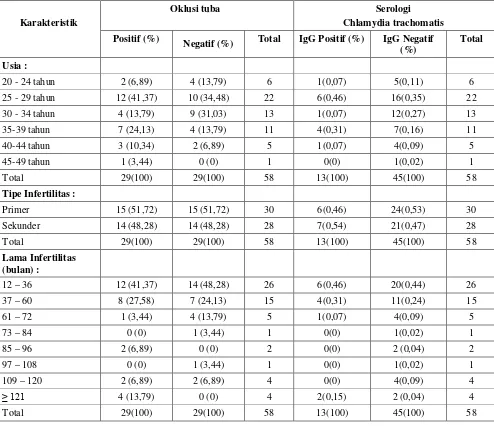
4.1. Karakteristik Peserta Penelitian
Karakteristik peserta penelitian mencakup usia, tipe infertilitas, dan lama infertilitas. Data menunjukkan bahwa sebagian besar peserta berusia antara 25-29 tahun dan mengalami infertilitas primer. Informasi ini penting untuk memahami demografi wanita yang terlibat dalam penelitian ini.
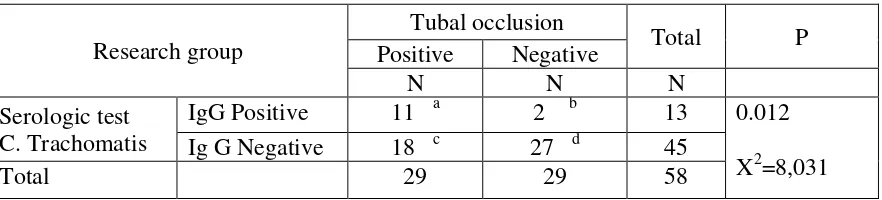
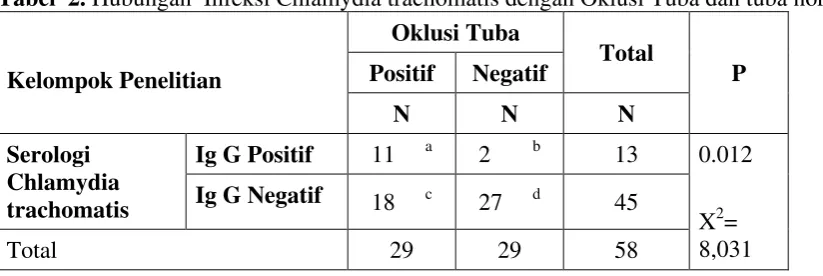
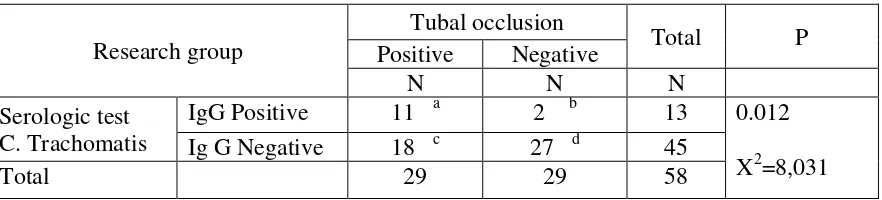
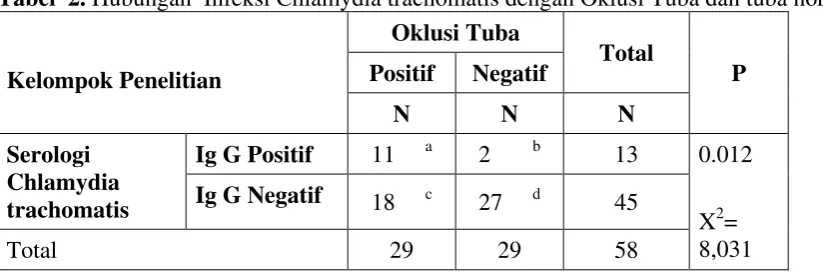
4.2. Hubungan Chlamydia trachomatis dengan Kelainan (Oklusi) Tuba
Hasil analisis menunjukkan bahwa proporsi infeksi Chlamydia trachomatis lebih tinggi pada wanita dengan oklusi tuba dibandingkan dengan yang memiliki tuba normal. Ini menunjukkan adanya hubungan signifikan antara infeksi dan oklusi, dengan nilai p < 0.05, yang mendukung hipotesis penelitian.
4.3. Keterbatasan Penelitian
Keterbatasan penelitian mencakup ketidakmampuan untuk membedakan antara berbagai mikroorganisme lain yang dapat menyebabkan oklusi tuba. Selain itu, ukuran sampel yang terbatas juga dapat mempengaruhi generalisasi hasil. Penelitian lebih lanjut diperlukan untuk mengatasi keterbatasan ini.
V. KESIMPULAN DAN SARAN
Kesimpulan dari penelitian ini menegaskan adanya hubungan signifikan antara infeksi Chlamydia trachomatis dan oklusi tuba pada wanita infertil. Penelitian ini memberikan bukti bahwa infeksi ini dapat menjadi faktor risiko penting untuk infertilitas, serta menyarankan perlunya skrining yang lebih luas untuk deteksi dini.
5.1. Kesimpulan
Kesimpulan penelitian menunjukkan bahwa wanita dengan infeksi Chlamydia trachomatis memiliki risiko 8.25 kali lebih tinggi untuk mengalami oklusi tuba dibandingkan dengan yang tidak terinfeksi. Ini menggarisbawahi pentingnya deteksi dan pengobatan infeksi ini dalam konteks infertilitas.
5.2. Saran
Saran dari penelitian ini adalah agar dilakukan skrining rutin untuk infeksi Chlamydia trachomatis pada wanita usia reproduktif, terutama yang mengalami infertilitas. Selain itu, penelitian lebih lanjut diperlukan untuk mengeksplorasi intervensi yang dapat mengurangi dampak infeksi ini pada kesuburan.
Referensi Dokumen
- Netter’s obstetrics, gynecology and women’s health ( Smith RP, Netter FH )
- Key topics in sexual health ( Cahill D )
- Current diagnosis & treatment obstetrics & gynecology ( DeCherney AH, Nathan L )
- Medical microbiology ( Brooks GF, Butel JS, Morse SA )
- Laboratory diagnosis of human Chlamydial infection ( Barnes RC )