Vol 9, No 3, July
-
September 2000 CT staging of laryngealcarcinoma
217Computed tomography
based
staging
in
the carcinoma of the larynx
Sarita Magu*,
Mona Bhatia*, Daya
Shankar Mishra*, VivekKumar
Kaushal**,
Manav Rakshak**,
Vikas Kakkar$
Abstrak
Karsinoma laring mewakili kira-kira sepertiga dari keganasan leher dan kepeLa dan merupalcan satu diantara keganasan yang paling sering di India. IJntuk mengevaluasi peranan CT scan dalarn proses " staging" karsinoma
laing,
dua puluh penderita telah dipelajari. Semua penderita adolah laki-laki dengan rata-rata usia 54 tahun. Laringoskopi Langsung dan tidak langsung memberi hasill)
tumorglotis (55%) dan 9 tumor supraglotis (45Vo). Secara histologis, semua tumor berjenis karsinoma skuamosa. Staging klinis dan CT dilakukan berdasarknn kriteria AJCC 1988. CT upstaging terjadi pada 13 kasus (65Vo). Beberapa invasi tumor hanya terdetel<si
dengan CT: daerah tiroaritenoid (55Vo) pasca laring (50Vo|
di
bawah pila suara (45Vo), sinus piriformis (35Vo| komisura anrcrtor (25Vo), invasi kartilago (25Vo), daerah preepiglotis (20Vo), pasca krikoid (lïVo), komisuraposteior
(l5Vo) dan subgloti,s (l0Vo). Keterlibatan kelenjar getah bening terdeteksi pada tiga penderita ( I5Eo).Abstract
Carcinoma of the larynx represents approximately one third of
all
head and neck cancers and is amongst the commonest head and neck malignancy in India. In order to evaluate the role of computed tomography in staging laryngeal carcinoma, tvventy consecutive patients of subsequently proved carcinoma of the larynx were recruitedin
this study.All
the patients were males with avarage ageof
54 years, Indirect and direct laryngoscopy revealed I
I
îumoursto
be glottic (55Vo) and 9 tumoursto
be supraglottic (45Vo).Histologically,
all
tumours were squamous cell carcinomas. The clinical and CT staging was done according to AJCC 1988 staging system. CT upstaging of the carcinoma occurred in 13 cases (65Vo). Certain invasions were detected only on CT: thyroarytenoid space (55Vo) paralaryngeal space (50Vo), undersurfaceof
true vocal cords (45Vo), pyriform sinus (357o), anterior commissure (25Vo),cartilage invasion (25Vo), pre-epiglottic space (20Vo), post cricoid (1 57o), posterior commissure ( I 5Vo) and subglottic extension ( l07o). Lymph node invotvement was detected in three patients (ISVo).
Keywords: Laryngeal carcinoma, computed tomography, larynx, CT staging.
Carcinoma
of the
larynx
representsapproximately
onethird of
all
head
and neck cancers.r Almost
all
malignancies
of
the larynx arise from the
mucosal surfaceand thus
are accessibleto direct
visualization
and
biopsy. The radiologist
evaluates
areas that theclinician
cannot
see, such as areas deepto
the mucosaor blocked
from
direct visualization by
the bulk of thetumour.2
The goal
of the radiologic
study
is to help
determining
the most appropriate therapy.
Modern
laryngeal
imaging
useseither
computed tomography
(CT)
or
magnetic
resonance(MR) imaging
to show
*
Department of Radiodiagnosis, Pt. B.D. Sharma PGIMS, Rohtak - 124001, Haryana, India
'* Department of Radiotherapy, Pt. B.D. Sharma PGIMS, Rohtak - 124001, Haryana, India
# Deparnnent of E.N.T., Pt. B.D. Sharma PGIMS,
Rohtak - 124001, Haryana, India
the
relationship
of
diseaseto
the
very
small laryngeal
structures.
Even
in
patients
who cannot
co-operate completely,CT
offers
a consistently good examination,with
short imaging
times and
thin
section.'
Better
geometric delineation
of
the anatomy
of
the
larynx
islikely to improve
staging and
radiation
treatment
of
the carcinoma
of
the larynx
as compared
to clinical
staging, especially for supraglottic and glottic cancers.3'45This
study
\ryas undertakento
assessthe role
of
computed tomography based stagingfor the staging
of
carcinomaof
thelarynx.
METHODS
218
Magu et alexamined
clinically, including indirect
laryngoscopyand had
Me
disease.
Direct
laryngoscopy
wasundertaken
in all
patients and
clinical
staging
wasdone.
Radiological
examination included
radiographyof
the
neck and
chest soft
tissue
and
contrastenhanced computerised
tomography
(CT).
CT
wasdone on Shimadzu
SCT 3000
TF
scanner. Sections
were obtained parallel
to
the laryngeal ventricle
asseen
on
lateral scout
view
with
the patient
in
thetreatment position.
If the
ventricle
wasnot
identified,
CT
gantry angle was adjusted so
that the
scan beamwas
parallel to
C5-C6intervertebral disc
space. Scanswere
obtained
in
quiet
breathing
from lobule
of
theear
to the
manubriosternal
junction. Five
millimeters
thick
sections
were taken with
additional
2
mm sections at thelevel
of
vocal cords.
2-D
reconstructionin
sagittal
and
coronal planes
were done using
computer
assistedfunctions
to
seethe
extent
of
thetumour.
The staging-
was done according
to
AJCC
1988 staging system.ÔRESULTS
The
present study comprises
20
patients, previously
untreated
and
histopathologicaaly
proved
squamouscell carcinoma
of
the larynx.
All
the
patients
were maleswith
the mean
ageat presentation of
54
years.Thirteen patients
(65Vo)
were aged
between
41-60years.
Fifteen patients
(75Vo)
were admitted within
four
months
of
the
onset
of
the
first symptom.
Hoarseness
16120(80Vo)
was
the
main
presentingsymptom,
the
other
were
stridor
7/20
(357o)
anddysphagia
5120 (25Vo).Indirect
anddirect
laryngoscopy revealed I
I
tumoursto
be
glottic
(55Vo)
and nine
tumours,
to
besupraglottic
(45Vo)(Table
I and 2). Table 3 shows the
comparative
clinical/CT
stagingof
the tumour.A
total
of
nine
(45Vo) casesof
carcinoma
of
the
glottis
were upstaged. One caseof
T1,carcinoma of the glottis
wasupstaged to T2 status;
two
casesof
T2 andsix
casesof
Tr
carcinoma
of
theglottis
were upstaged to Ta status.At
the
supraglottic site,
CT
upstaging of the primary
lesion was
seen infour
(20Vo) cases. One caseof
T2and T3 each and both cases
of
T2 status were upstagedto T4 status. On
clinical
evaluation,
only
seven (35Vo)cases
found
to
be staged
correctly when
comparedwith
CT staging.
All
were
squamouscell
carcinomaof
owhich
3}Ve-.werewell
differentiated,
55Vowere
moderately differentiated,
while
l}Vo
were
poorly
differentiated.
Med J Indones
Clinical
examjnation
of
the
cervical
lymph
nodesrevealed two patients
with
Nz status and one casewith
N3 status. On CT staging, three cases were detected as
having occult lymph
nodes. Theoverall upstaging
wasobserved
in
13
cases
(657o). Table
4
shows
thevarious tumour
invasions detected
only on CT
andwere
primarily
responsiblefor
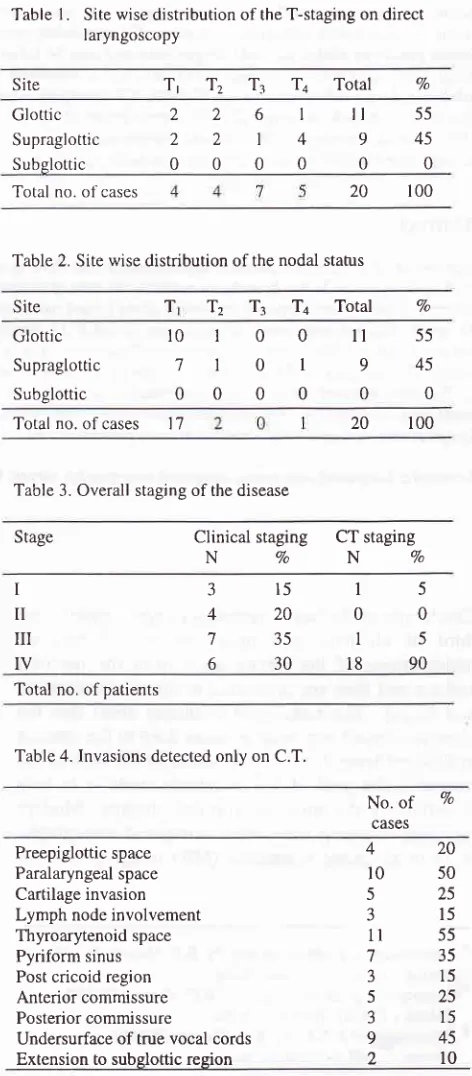
the upstaging.Table
l.
Site wise distribution of the T-staging on direct laryngoscopyTl T2 Tr '14
Total VoSite
Glottic Supraglottic Subslottic
2 2 0
2 2 0
6 I 0
I
4
0
il
9 055 45
0
Total no. of cases 20 t00
Table 2. Site wise distribution ofthe nodal stahrs
T
Site
T2 T3 T4
Total VoGlottic Supraglottic Subglottic
l0
7 0
ll
9 055
45 0
100
101
000
Total no. of cases t7 20 100
Table 3. Overall staging of the disease
Stage Clinical
staging
CT stagingNVoNVo
I
II
III
IV
3
4
7 6
15 20 35 30
I
0I
18 5
0
5 90
Tota! no. ofpatients
Table 4. Invasions detected only on C.T.
No.
of
Vocases
Preepiglottic space
Paralaryngeal space
Cartilage invasion Lymph node involvement Thyroarytenoid space
Pyriform sinus Post cricoid region Anterior commissure Posterior commissure
Undersurface of true vocal cords
Extension to subglottic region
420
l0
50525
315
1l
55735
315
525
3
15 [image:2.595.337.573.187.725.2]Vol 9, No
j,
July-
September 2000DISCUSSION
Almost
all
malignancies
of
the larynx
are
squamouscell
carcinoma.'
In
our
study
all
the patients
weremale.
A
male
preponderance
has been reported
in
other
studies.t-tuOur
study revealed that
55Voof
the
tumours
were glottic,
which
is well
documented in
literature.eThe
mean ageof
the patients was54
yearswith
657oin
the agegroup of
4l-60
years. Hoarsenesswas the
predominant symptom
(80Vo).
For
manyyears, examination
of
the
larynx was restricted
todirect
and
indirect
laryngoscopy, conventional
tomo-graphy
andlaryngography.r'
with the development
of
better radiation therapy planning and
conservativesurgery techniques; precise delineation
of
tumour
extent preoperatively
by
imaging
studies
and
exactstaging
have
become
imperative
for
the
apyropriate therapeuticplanning of laryngeal
carcinoma.r'CT
displays thelarynx
in
a3-D format
allowing
direct
demonstration
of
tumour
in
both
the
larynx
andparalaryngeal soft
tissues aswell
ascartilages.'t
CT
ismore
accurate
than
laryngography
in
determining
superior and
inferior limits
of
the tumour.ll
In
our study,
CT
upstagingof
thecarcinoma
occurredin
13
(65Vo) cases.
Twelve
cases (60Vo),
wereupstaged
to
stage
IY1,57o
from
stage
I,
20Vafrom
stage
II
and 35Vofrom
stageIII,
while
one
(57o) casewas
upstaged
from
stage
I
to
stage
III. In
35Voof
cases, staging changed
from Tr
to
T+;in
20VofromT2
to
T4 statusand
in
SVofrom
Tz
to T4. Charlin et
ala
have also observed thatCT
was mostuseful
in
lesionsinitially
classified
as
T2
and T3.
Sulfaro et al
found
that CT
has ahigh
overall specificity i.e.
88.2Vobut
alow
sensitivity
(47.l
Vo).5Clinical
and endosc-opicevaluation may
fail to
revealcartilage invasion.''
In
our
study, cartilage
involve-ment was
seenin
25Vo cases,not
detectedclinically.
Evidence
of
cartilage invasion
is
related
to
tumour
size: lesions greaterthan
16mm
lying
below
the apexof
the
arytenoid have
a high probability
of
cartilageinvasion.ro
CT
may
detect
erosion
of
laryngeal cartilageswhen
sufficiently
extensivebut microscopic
extension cannot bedetected.a't'"'tt
Tu-our
extensionlateral
to the
arytenoid cartilage
is
difficult
to
âssessby
laryngoscopy
but
may
be
assessed
by CT.
Widening
of
the
thyroarytenoid
spaceindicates
such asan invasiontO't'
andwas
seenin
55Voof
our
cases(Fig.1).
CurtinrT considered
obliteration
of
fat within
or
widening
of
the
thyroarytenoid gap
on
CT
asinvolvement
of
thepyriform
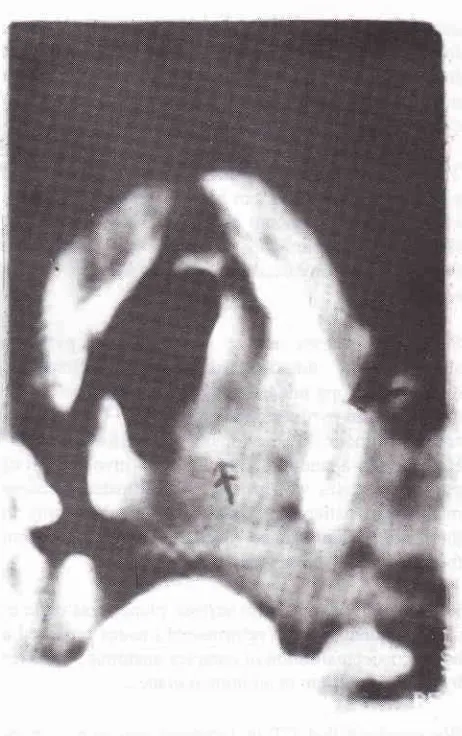
sinus apex. [image:3.595.333.564.74.442.2]CT staging of laryngeal
carcinoma
219Figure 1. Axial CT (glottic level); growth involving the vocal
cord,
exlensionlateral
to
the
arytenoid cartilage, medial tlispLacementof
the arytenoid and widened thyro-arytenoid distance. Notice there is also invasion ofthe.thyroid cartilage.In
the presentstudy,
two
cases(l}Vo)
with
subglottic
extension
were missed
clinically.
Tumours
arising
between the true cords andlower border
of cricoid
arerare.
Any
soft
tissue between
cricoid cartilage
andairway
is
abnormal
and may
represent
subglottic
tumour
extension.ls
Inferior
extension
can easily
be assessedwith
either
CT or MR
imaging.
However,
MRI
doesafford the additional perspective
of
coronal
sections.2
Involvement
of
preepiglottic
space
occurs
with
supraglottic
tumours.The
depthof
tumour invasion
isthe most
difficult
to
measureclinically.r3
In
our
study,45Vo
were
supraglottic tumours.
[n
20Vo
cases,preepiglottic space involvement
was
not
detectedclinically,
but
was seen onCT. CT
is morereliable
for
22O
Magu etal
into
_-the
preepiglottic
space
and
aryepiglottic
fold.r-J'rr'reDetection
of
this type
of
invasion
is
vital
for
future
therapy
planning. Preepiglottic
space doesnot
contain
lymph
nodes,
but
doescogtgin lymphatic
channel that
allow
cervical
metastasis.'*'"
Tumour involvement
of
tissue deep
to anterior
andposterior
commissures can be detectedby CT
if
thereis
an
increasein
amount
of
tissue
and/or fixation of
tissue.
The anterior and posterior
commissure
werefound
to
be
involved
in
25Vo
and
l5Vo
casesSeven
(357o) casesshowed
involvement
of
pyriform
sinuses
on CT,
not
detected
clinically. Indirect
anddirect
endoscopy
underestimatedthe extension
of
thetumour
rm
sinus
apexwhile CT conectly
reveals
the
apex
of
pyriform
fossa.'''Howev
by
Duggal et al,a involvement
of
pyriform
sinuseswas grossly overestimated, because
majority of
patients
had
undergone tracheostomy
in
their
study and hence,
were
unable
to
perform
modified valsalva
manoeuvre.Reformation
of
imagesin
various
planeswas
donein
all
the patients.
Thesereformatted
imagesprovided
abetter conceptualisation
of
complex anatomic structuresby displaying
themin
additional
planes.We
conclude
that
CT
in
laryngeal carcinoma,
whenused
to
determine
tumour
extent,
hasmarked impact
on
accuracy
of
staging.
This
is best
manifested in
displaying
deeptumor
extension
that
cannot
be
seenduring
evaluationof
mucosal surfaceby
laryngoscopy/endoscopy.
REFERENCES
W.H.O.
I.A.R.C. Cancer incidencein
flve
continents.Scientific Publications No.2, Lyon 1982; Vol lV, 390.
Curtin
HD.
Imagingof
the larynx:
current concepts.Radiology 1989; 173:
l-l
l.
Katsantonis GP, Archer CP, Rosenblum
BN
etal. The
degreeto
which
accuracy of. preoperative stagingof
laryngeal carcinoma has been enhancedby
computed tomography. Otolaryngol Head Neck Surg 1986; 95(l):52-6.
Duggal RK, Jain RC, Knadelwal N, Mehra YN, SuÉ S.
Clinical and CT correlation in transglottic tumours of the
larynx. Ind J Radiol Imag
l99l; l:
8l-5.Med J Indones
Sulfaro S, Barzan
L,
GuerinF
et al.
T
stagingof the
laryngohypopharyngeal carcinoma.
Arch
OtolaryngolHead Neck Surg 1989; 115:613-20.
Beahrs
DH.
Manualof
stagingof
cancer.4û
ed. JBLippincott Co., 1992: p. 34-40.
Barnes
L,
Gnepp
DR.
Diseasesof the
larynx,hypopharynx, and oesophagus.
[n: Surgical Pathology
of
the Head and Neck. New York: Dekker, 1985: p. 14l-226.Jussawalla DJ, Sathe PV. Cancer incidence in Aurangabad city 1981. Indian Journal of Cancer l98y'.;21(2):55. Powell J, Robin PE. Cancer ofhead and neck: the present
state.
In:
R. Rhys Evans, Evans R,
Robin PE, FiellingJWL,
Eds. Head andneck cancer.
Tunbridge Wells:Castle Rouse Publications, 1983: p. 3-16.
Hiranandani
LH. Panel
on epidemiology and etiologyof
f aryngeal cancer. Laryngoscope 197 5; 85: I 197.Phelps PD. Carcinoma of the larynx
-
the role of imagingin
staging
and
pretreatment assessments. ClinicalRadiology 1992;46:7 7 -83.
Sagel SS, Aujderheide JF, Aronberg DJ
et al.
High re-solution computed tomographyin
the
stagingof
car-cinoma of the larynx. The laryngoscope l98l;91:292-300. Archer CR, Sagel SS, Yeager
VL,
Martin S, FriendmanWH. Staging
of
carcinomaof
the larynx: comparativeaccuracy
ofCT
and laryngography. AJR 1981;136:.571-5. CharlinB,
Brazeau-LamontangeL,
GuernierB et al.
Assessment
of
laryngeal cancer:
CT
scan
versusendoscopy. J Otolaryngol 1989;18(6):283-8.
Gerristen GJ, Valk J, Van Velzen DJ, Snow
GB
et al.Computed tomography:
a
mandatory investigational procedurefor T
stagingof
advanced laryngeal cancer.Clinical Otolaryngol 1986;l I :307-16.
Archer
CR,
Yeager
VL,
Herbold DR.
Computed tomography vs histology of laryngeal cancer-
their valuein
predicting laryngeal cartilage invasion. Laryngoscope I 983;93:140-7.Curtin
HD. Imaging
of
the larynx.In
Head and Neck Imaging, 2"d Ed. CV Mosby, 199l:593-692.Hoover
LA, Calcaterra TC, Walter
GA. Preoperative CTscan evaluation for laryngeal carcinoma: correlation with pathological findings. Laryngoscope 1984 Mar; 94:310-5.
Deschepper C, Casselman J, Vande Voorde W et al. The contribution
of
CT
to
the
T
stagingof
laryngeal carcinoma. J Belge Radiol 1989;72(3):191-7.Clerf
LH.
The
preepiglottic space-
its
relation to
carcinomaof
the
epiglottis.Arch
Otolaryngol 1944;9O:177-9.
Dayal VS, Bahri H, Stone PC. Preepiglottic space
-
An anatomic study. Arch Otolaryngol 197 2;95:130-3. Lain KH, Wong J. The preepiglottic spacein
relation to spreadof
carcinomaof
the larynx.Am J
Otolaryngol 1983;4:81-91.Saleh EM, Mancuoso
AA, Stringer SP. Relative roles of
CT and endoscopy for determining the inferior extentof
pyriform
sinus carcinoma: correlative histopathologicstudy. Head and Neck 19931'15:33-52. 5.
6.
7.
9
10.
t2
13
l4
l5
Il.
t7.
l6
18.
t9
20
2t
22
23. I
2.
J.
4
T
Se
Rd(
3æ hiô
ArE Hir dilq
kol€
:rd
*
saut
100 btiS
R€fi
1. n
3.)
Keû
P'